Concussion in sport: the role of assessment tools and other evidence-based strategies
Sport-related concussion is a common sporting injury induced by biomechanical forces. It results in transient impairment of neurological function that typically resolves spontaneously but can be prolonged in some individuals. Differentiating concussion from structural head injuries and other serious pathologies is essential. Evidence-based strategies can guide decision-making when assessing and managing an athlete with possible sport-related concussion.
Sport-related concussion (SRC) is a common athletic injury, with an estimated incidence of 18 concussions per 1000 athlete-hours in contact and collision sports.1-3 In the United States, between 1.6 and 3.8 million sport-related traumatic brain injuries occur each year, most of which are concussions.4 Published estimates of the incidence of concussion, which represent hospital data, likely underestimate the true burden because a large proportion of individuals do not seek any medical attention.5
In recent years, SRC has received a high level of attention in the mainstream media and sports medicine literature, which is in large part due to discussion about the long-term brain health of former athletes and its association with contact, combat and collision sports.6 While the potential relationship between sports exposure and long-term brain health is debated, it is clear that SRC can cause significant morbidity in the first few weeks to months following injury.6 Medical practitioners may be the primary point of contact immediately after injury. More commonly, however, athletes will seek medical care for ongoing symptoms or for a medical clearance to return to sport in the week(s) following injury.
Evidence-based strategies can guide decision making. This article summarises current assessment and treatment strategies and provides an overview of some of the modifying factors that contribute to the incidence and severity of SRC. Useful resources are available to guide assessment and management of SRC; some of these are listed in the Box. Pharmaceutical management of head injury is not covered in this article.
{kind=link}
What is sport-related concussion?
The definition of SRC was updated by the 2017 Concussion in Sport Group (CISG) in the fifth Consensus Statement on Concussion in Sport.7 The common features of SRC can be summarised as follows:
- a direct blow to the head or neck or indirect trauma anywhere on the body with a force transmitted to the head
- rapid (over seconds to minutes) or delayed (over minutes to hours) presentation of symptoms and signs, typically with spontaneous resolution
- negative findings on standard neuroimaging (CT or MRI), reflecting a functional rather than structural injury
- a range of clinical features, frequently (but not always) occurring without loss of consciousness or post-traumatic amnesia, and stepwise resolution.
Initial assessment
The diagnosis of SRC has evolved substantially over the past few decades; however, its immediate and accurate recognition in a clinical setting remains a challenge.7,8 To date, there is no defined magnitude of impact that can identify when a concussion has occurred, nor any currently validated biomarker for making a diagnosis.9,10 Rather, SRC is diagnosed clinically based on the observed mechanism of injury, signs and self-reported symptoms.11 Overt signs, such as loss of consciousness, ataxia, tonic posturing or post-traumatic seizures, are uncommon but immediately diagnostic of a concussion or more substantive brain injury and should result in instant removal of the athlete from the field of play.8,12 Covert signs, such as a blank or vacant stare or quickly-resolving motor incoordination, are often harder to identify, particularly in amateur sport settings. Signs of SRC may be brief and resolved completely by the time the player is assessed by a medical team on-field.13 Furthermore, players may experience symptoms only, and fail to report them to the attending practitioner. Symptoms may present immediately or evolve over time, usually within the first 24 hours.14 The most commonly reported symptom of concussion is headache; other symptoms may include dizziness, fatigue, memory loss, concentration difficulties, insomnia, neck pain, irritability, visual disturbances and feeling ‘in a fog’.15-17
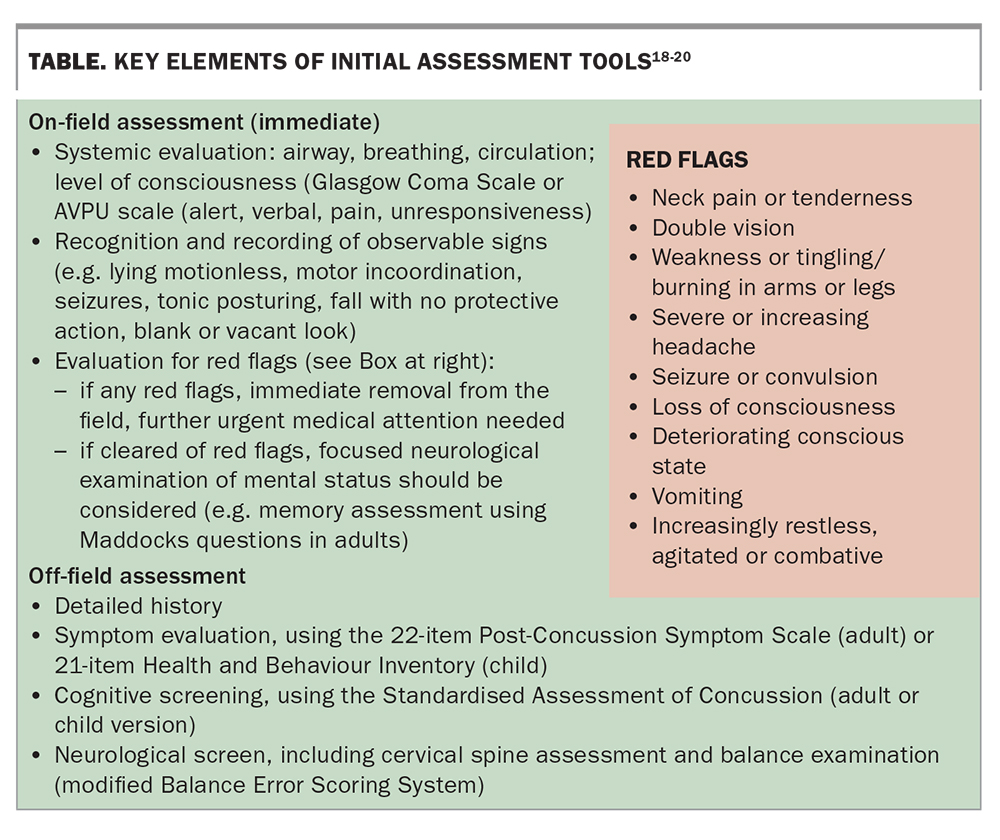
The CISG has developed tools for the diagnostic evaluation of individuals who are suspected of having sustained an SRC, which were updated in 2017 and are freely available online (Box). These include the fifth edition of the standardised Sport Concussion Assessment Tool (SCAT5) and a separate tool for athletes aged 5 to 12 years, the Child SCAT5, which accounts for developmental differences in this age group.18,19 Key elements of assessment tools, recommended to be interpreted by medical professionals, are summarised in the Table.18-20 The SCAT5 has good clinical application over the first three to five days after SRC.8,21 An important component of the initial screening and subsequent medical examination process is to ensure the absence of any life-threatening trauma, such as intracranial injuries, spinal cord lesions, cervical spine fractures or other red flags, which necessitates emergency hospital management. Red flags that are suggestive of these conditions are listed in the Table above.
{kind=link}
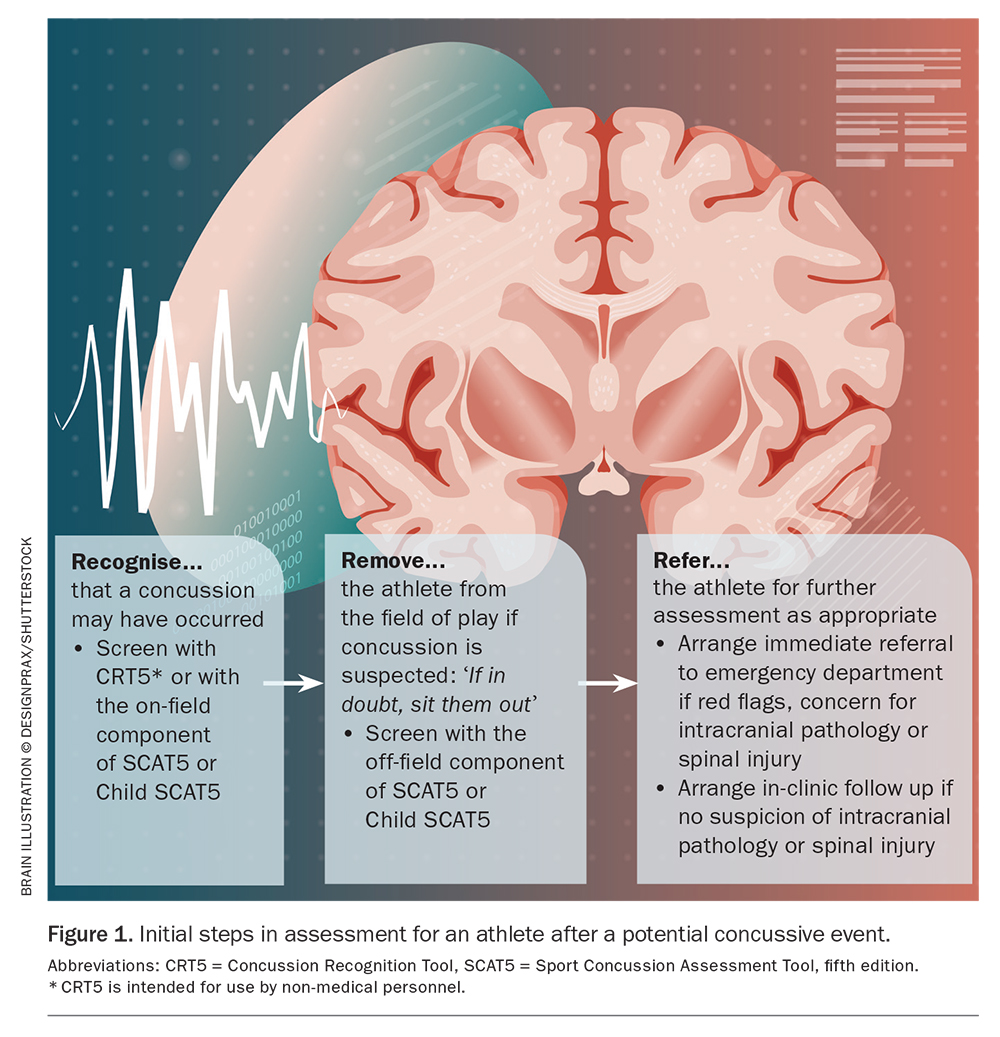
It should be noted that both the SCAT5 and Child SCAT5 are designed as early screening tools and do not replace a comprehensive clinical examination.18 A final diagnosis of a concussion may be based on the observed signs on the field, athlete-reported symptomatology, definable differences in SCAT5 performance or the medical practitioner’s clinical examination, if the neurological disturbance cannot be explained by any other or more serious pathology.22 Initial steps in assessment are summarised in Figure 1.
{kind=link}
The CISG has developed a separate tool, the Concussion Recognition Tool 5 (CRT5), for use by non-medically trained individuals such as parents, coaches, players, officials, sports administrators and teachers.23 The CRT5 is designed to assist in recognising suspected concussion in children, adolescents and adults and to provide information about initial management, including removal from the field of play.23 In the absence of life-threatening trauma or red flags, any athlete who is suspected of having a concussion should not be left unsupervised and should be referred to a medical professional for further assessment.20
If SRC is suspected by on-field healthcare staff or match officials and if there are no medical staff on-site to determine otherwise, the athlete cannot return to play that day.20 In community level sport, where medical personnel and sideline injury surveillance (including video footage of the incident) are not available, it is not possible to adequately evaluate an athlete to determine if they have not suffered SRC and are then able to return to the field of play. In this instance, it is best to remove the athlete from the field of play (following the steps outlined above) and seek medical attention.
At the professional and some semi-professional levels of sport, there are Head Injury Assessment (HIA) protocols set up. If an athlete is returned to play following an HIA, further monitoring over a 24- to 48-hour period is recommended and mandated in nearly every sport worldwide that has an HIA protocol.24 These protocols usually involve reviewing video footage of the incident, if available, which can provide information pertaining to the mechanism of injury and acute signs (e.g. loss of consciousness, motor incoordination, seizures) and a series of medical assessments over the next 24 to 48 hours to confirm or eliminate a suspected concussion.25
The Concussion in Sport Australia Position Statement, which was updated in 2019, is a useful resource with information developed for medical practitioners as well as for other personnel.26 The Statement includes practical guidance for on-field and off-field assessment and management of athletes with suspected concussion and is available online (https://www.sportaus.gov.au/__data/assets/pdf_file/0005/683501/February_2019_-_Concussion_Position_Statement_AC.pdf).
Post-acute assessment
The primary goals of post-acute assessment of an athlete following a concussion are to guide management, educate the athlete about their recovery and to reduce the extent and duration of morbidity.27 Although estimating an individual’s prognosis is not easy, the number and severity of initial symptoms are the best predictors of length of recovery after SRC.20,28 A low level of symptoms (≤7 on the Post-Concussion Symptom Scale) on the first day after injury is considered a favourable prognostic indicator.7,28 A history of SRC is a risk factor for future SRC.29 In some athletes, multiple SRCs are associated with increased physical, cognitive and emotional symptoms.7 Also, heterogeneity in concussion presentations dictates a multifaceted clinical assessment rather than a single measure of symptomatology, neurological or physical function.9
Standard neuroimaging studies (CT, MRI) should only be used to exclude more severe traumatic brain or neck injury. Pre-existing, coexisting and resulting comorbidities (headaches, mood disorders, cervical spine pain, vestibulo-ocular disorders and autonomic dysfunction) should be considered.30
Management
Current CISG guidelines recommend a brief period (24 to 48 hours) of cognitive and physical ‘relative’ rest during the acute phase after injury – that is, only engaging in activities that do not exacerbate symptoms or bring on new symptoms.7 Any additional rest is considered counterproductive and impedes recovery.31 Athletes should be advised to refrain from alcohol, sedatives and recreational drugs, which could exacerbate or mask symptoms after SRC.7
In most adults who experience SRC, complete resolution of symptoms typically occurs within seven to 10 days.7 In children and adolescents, symptom resolution may be slower and can take up to a month.32 About 10 to 30% of individuals will have ongoing symptoms, beyond expected timeframes, which can cause frustration for the athlete and provide a challenge for the clinician.16,33 For athletes who present to their GP with ongoing symptoms, a multidomain assessment based on symptom reports and consideration of the patient’s past medical history is needed – this could include a full neurological examination, balance and coordination check, visual and vestibulo-ocular assessment, mental health and cognitive assessment and musculoskeletal examination of the head and cervical spine.8,16
Current consensus recommends a multifaceted clinical approach to the assessment and management of concussion.16 Practitioners who may assist should ideally have experience in the management of SRC and may include neurologists, psychiatrists, physiotherapists, psychologists, optometrists, speech therapists, exercise physiologists and occupational therapists as required, based on individual needs. A multidisciplinary team approach using targeted, symptom-specific interventions is recommended for athletes presenting with persistent symptoms.16,34-38 There is increasing evidence to support the use of subsymptom threshold aerobic exercise for autonomic dysfunction, targeted physiotherapy for cervical spine or vestibular dysfunction, and a collaborative, cognitive behavioural therapy approach for ongoing mood and behavioural disorders.16,35,36,39-44 Academic and lifestyle adjustments involving sleep, nutrition and hydration may also facilitate recovery.44,45
Pharmacological treatment is rare in SRC but may be used selectively in individuals with persistent symptoms.20
Return to learn
As part of the recovery process, children, adolescents and young adults are frequently required to return to academic studies. Although limited research exists, preliminary evidence suggests that student athletes who sustain SRC have similar 12-month academic outcomes to students who sustain musculoskeletal injuries.46 Although this is comforting and a key focus of early education, studies have shown that, in the short-term, adolescents may require more time off school and often return to school too early.46,47 Greater symptom burden in the initial presentation and symptoms that indicate difficulties with information processing may indicate potential difficulties returning to the classroom – these include concentration difficulty, memory issues, sensitivities to light or sound, or symptom exacerbation with mental activities.48
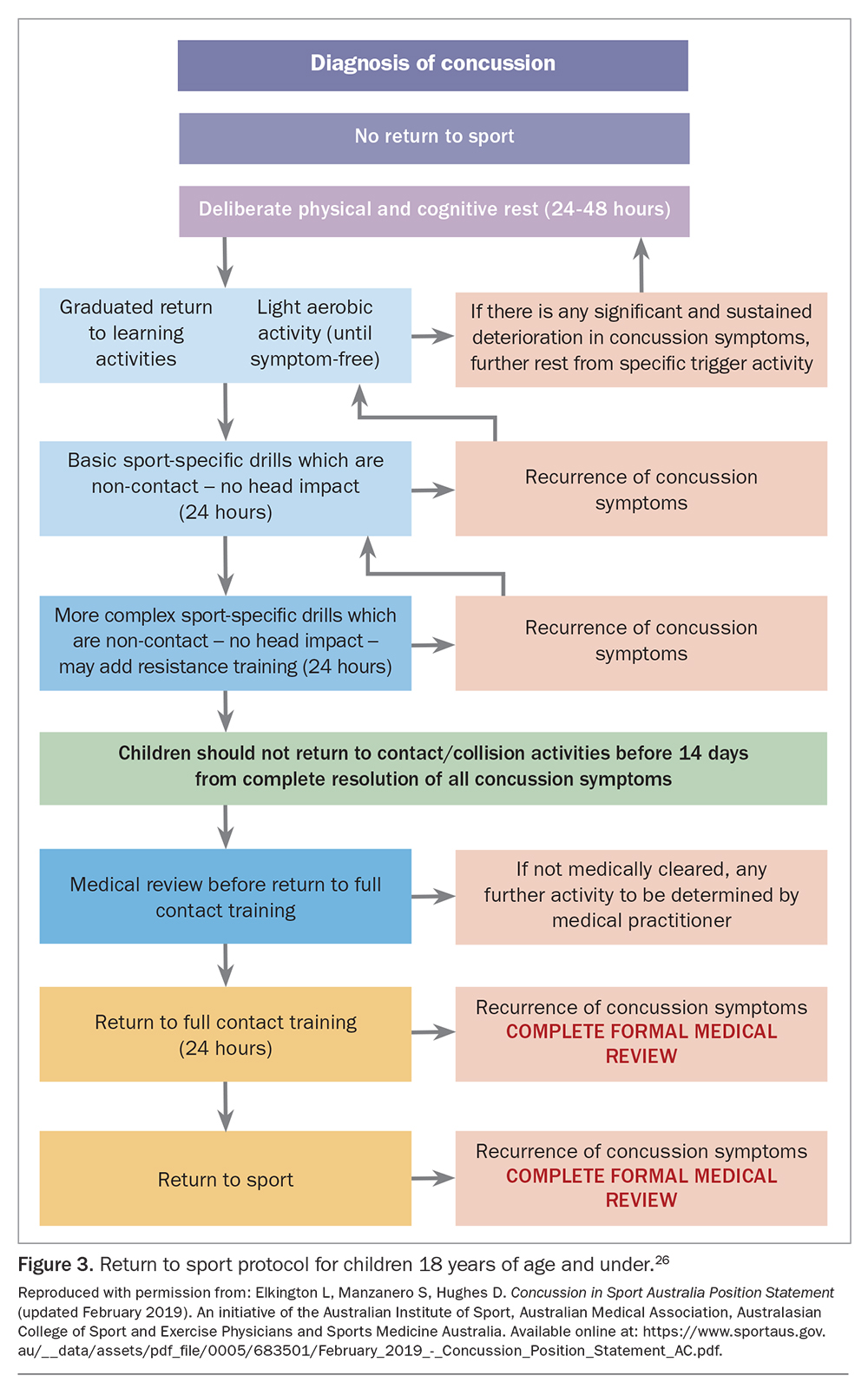
Return to learn/work programs should be considered gradual and progressed without symptom exacerbation. If required, a graded approach may be indicated with appropriate academic/employment accommodations made. These may include symptom-limited activity and study, special considerations for assignments and examinations, and gradual re-introduction to school/work with a phased return. For children and adolescents, successful progression through the graduated return to learn stages (starting with symptom-free learning, followed by school activities at home, then part-time return progressing to full-time return) must precede return to sport, although concurrent commencement of symptom-limited aerobic exercise is recommended.7,48 With standardised protocols in place, students have still been shown to develop new learning difficulties and therefore progressive monitoring of return to academic study is recommended.49 If children and adolescents do continue to show symptoms of concussion, a subsequent complete medical examination may help guide management and appropriate multidisciplinary referral. Consideration should be given to all potential causes of learning difficulties, including neurological, psychological, auditory and visual disturbances or cognitive deficits, as early intervention may potentially prevent lengthy time away from academic study or sport.48
Return to play
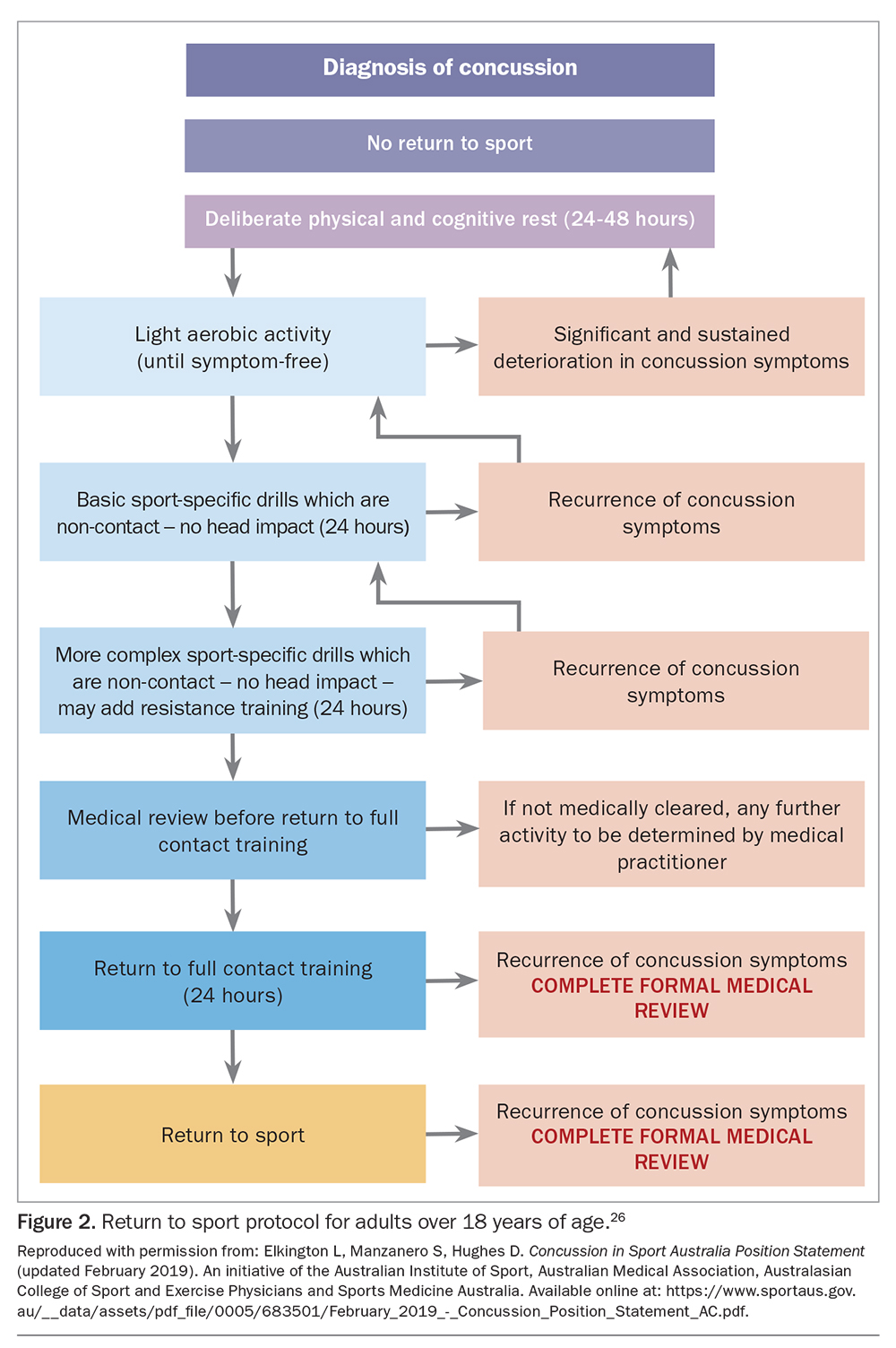
Return to play (RTP) is the process of transitioning back to practice and competition after SRC.7 After the recommended period of relative rest, individuals are encouraged to gradually return to function in a manner that does not exacerbate symptoms.7,49 It is important to educate patients that symptoms may be present during the recovery period and that light activities that do not exacerbate symptoms can be continued. Once the individual is tolerating regular daily activities (after the initial 24 to 48 hours), they can start the RTP framework and progress in a graded manner, with at least 24 hours for every stage. Athletes who experience an aggravation of any concussion-related symptoms should return to the previous asymptomatic level for another 24 hours before attempting to progress again.18 Medical clearance following a complete medical examination must occur before participating in full contact practice. Currently, there is no single measure of brain recovery following a concussion.7 Rather, medical practitioners must rely on their clinical judgment when returning an athlete to sport, by ensuring that the athlete has had a period of cognitive and physical rest followed by a gradual return to activity with monitoring for recurrence of symptoms. Return to sport protocols for adults and children are outlined in the Concussion in Sport Australia Position Statement (Figure 2 and Figure 3).26
{kind=link}
{kind=link}
If symptoms persist, the player should cease activity and return for follow up with their doctor for additional assessment and referral to relevant multidisciplinary team members.
Conclusion
SRC is a common athletic injury with a multitude of clinical presentations. If SRC is suspected, the athlete must be removed from the field of play for further assessment. In the acute setting, screening for red flags and serious pathology is critical. The SCAT5 and Child SCAT5 form part of the initial screening process but do not replace a thorough clinical examination. Follow-up medical assessment is required. A brief period of cognitive and physical rest (24 to 48 hours) and a graded, active return to function are recommended. Most individuals have an uncomplicated recovery but some have ongoing symptoms responsive to treatment. If symptoms persist beyond expected timeframes, a multifaceted assessment of various domains can be used to guide management and facilitate appropriate referrals to members of the multidisciplinary team. Return to learn should precede return to play in children and adolescents. Medical clearance is required before returning to full contact practice. MT
COMPETING INTERESTS: None.
Acknowledgement: The authors thank Associate Professor Andrew J. Gardner, Clinical Neuropsychologist at The University of Sydney, for his review of the manuscript.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.