Eliminating hepatitis C: Part 5. Practical steps in your practice

Dr Baker is a GP at East Sydney Doctors; and Senior Lecturer at the University of Notre Dame Sydney, Sydney, NSW. Dr Balcomb is a GP in Orange; and Honorary Lecturer at The University of Sydney, NSW. Dr O’Loan is a GP at Medeco Medical Centre Inala; Director of the Kombi Clinic; and Senior Lecturer at the University of Queensland, Brisbane, Qld. Dr Howell is a Consultant Gastroenterologist at St Vincent’s Hospital; Postdoctoral Research Fellow in Disease Elimination, Burnet Institute; and Postdoctoral Research Fellow in the Department of Medicine, University of Melbourne, Melbourne, Vic.
Liver diseases
For most people with chronic hepatitis C, treatment with direct-acting antiviral (DAA) therapy is simple and easily incorporated into primary care. GPs can help in the push to eliminate hepatitis C by 2030 through strategies to eliminate hepatitis C from their own practices. This includes finding their patients with hepatitis C, assessing, treating and following up after DAA therapy.
- GPs can help achieve the goal of eliminating hepatitis C in Australia by 2030 through ‘microelimination’ in their own practices.
- Since 2016, over 6000 Australian GPs have treated patients with direct-acting antiviral (DAA) therapy.
- For most people with chronic hepatitis C, treatment with DAA therapy is simple and easily incorporated into primary care.
- Patients can be tested for hepatitis C, assessed, treated and followed up for cure in four GP visits, with an optional fifth visit during treatment.
- Ongoing care for patients after DAA therapy includes care of comorbidities and strategies to prevent and detect reinfection in those with ongoing risk.
Australia aims to eliminate hepatitis C by 2030. The contribution of GPs is essential to achieving this goal, and Australian GPs are leading the world in treating their patients with hepatitis C in primary care. Since the arrival of direct-acting antiviral (DAA) therapy in March 2016, over 6000 GPs have treated one or more people living with hepatitis C.1 GPs are also treating an increasing proportion of patients.2 At the same time, there have been steady improvements in assessment and therapy, which have made the treatment pathway even more straightforward.3
This is the final article in the series on eliminating hepatitis C. Previous articles have reviewed patient testing, assessment, treatment and follow up after DAA treatment.4-7 This article summarises practical ways for GPs to eliminate hepatitis C in their individual practices.
Microelimination in your practice
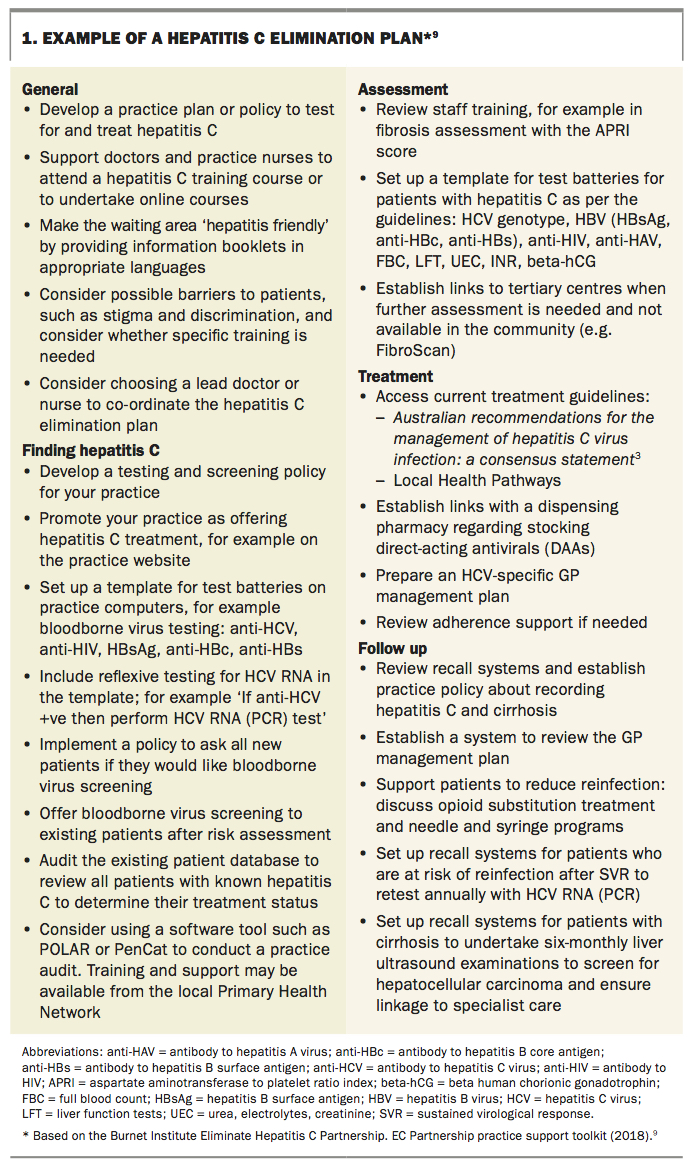
A useful approach for GPs to help achieve the goal of eliminating hepatitis C is ‘microelimination’. This is the concept that we as GPs can focus on pursuing hepatitis C elimination in our own practice or community.8 This involves some planning to tailor an approach for our individual clinic. An example of a hepatitis C elimination plan is shown in Box 1.9
{kind=link}
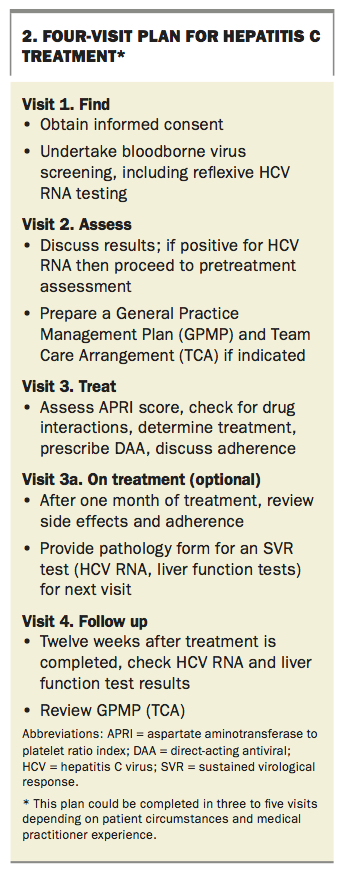
Eliminating hepatitis C involves four steps: finding patients with hepatitis C, assessing, treating and following up. These steps can be achieved in four patient visits, with an optional fifth visit during treatment, as summarised in Box 2. Depending on patient circumstances, medical practitioners experienced in hepatitis C management may be able to achieve the steps in three visits.
{kind=link}
Find patients with hepatitis C
There are two main groups of people with hepatitis C who need DAA treatment:10
- people who are undiagnosed (estimated to be about 20%)
- those who have been diagnosed previously with hepatitis C but remain untreated.
Both groups are important to reach.
Patients who are undiagnosed
Your approach to testing for hepatitis C will depend on your practice profile. One approach is to test everyone. Universal testing (or screening) is recommended as part of antenatal screening in Australia.11 GPs working in high-prevalence practices, such as in homeless health or opioid substitution therapy, might consider offering testing to all patients.
Otherwise, testing for hepatitis C is generally based on risk, as discussed in Part 1 of this series.4 Sometimes, risk factors for hepatitis C may be difficult to identify during a busy GP consultation. In addition, for many patients, risk factors may have occurred in the distant past, such as a period of injecting drug use in their youth.
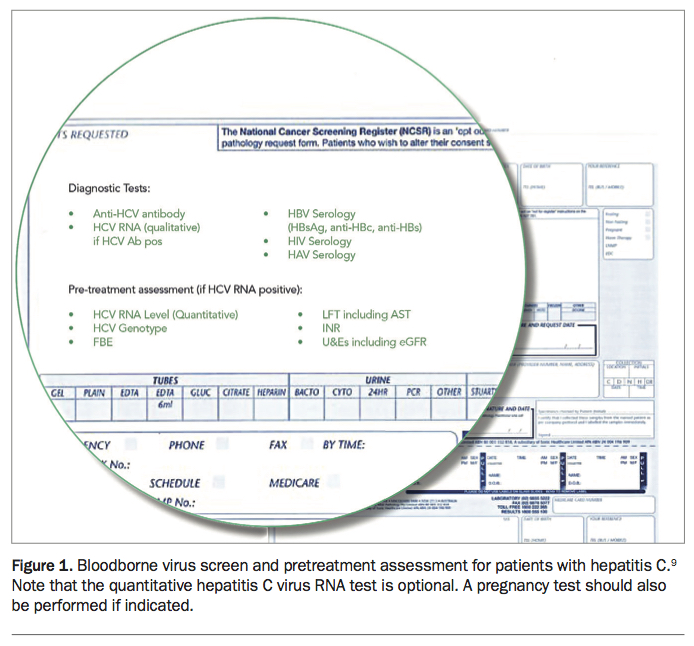
Most GPs take a social history from new patients, and this is an opportunity to enquire sensitively about risk factors such as current or past injecting drug use, along with recording demographic variables such as country of birth and sexual behaviour. This information is also crucial for establishing whether there is a need to test for bloodborne viruses such as hepatitis B virus and HIV along with hepatitis C, which can all be performed as part of ‘a new patient screen’. Tests included in bloodborne virus screening are shown in Figure 1.9
{kind=link}
Existing patients also need to be tested for hepatitis C. There are many opportunities for testing as part of general health checks, sexual health screens, pre-travel check-ups and antenatal screening.
Patients with hepatitis C can also be found by searching the practice management system. Third-party tools such as POLAR (https://outcomehealth.org.au/polar.aspx) and PenCat (https://help.pencs.com.au/dashboard.action) can help find patients with potential risk factors (e.g. abnormal liver function test results) for testing. Advice on using these tools can be obtained from your local Primary Health Network.
Patients who are diagnosed but not treated
Most people living with hepatitis C have been previously diagnosed. This group of patients includes those who have declined treatment and others who are not engaged in regular medical care. Many people living with hepatitis C belong to marginalised populations and may have limited contact with the healthcare system. They are also an important group to engage and to support into treatment. A GP outreach project, the Kombi Clinic, that aims to engage and support people with hepatitis C, especially marginalised populations, into treatment is described in Box 3.
{kind=link}
Assess patients
Assessment of patients was covered in Part 2 of this series.5 The initial test to diagnose hepatitis C is a hepatitis C antibody test. If the result is positive then current infection needs to be confirmed with a qualitative hepatitis C virus (HCV) RNA (PCR) test. If this result is positive then it is followed by HCV genotyping.
Other recommended blood tests after diagnosis of chronic hepatitis C are shown in Figure 1. They include tests:
- to detect hepatitis A, hepatitis B and HIV infection (if not already performed)
- to assess renal and liver function
- to exclude pregnancy.
The most complex part of pretreatment investigation is assessing for advanced liver disease. Patients with cirrhosis need specialist referral and may require changes to the treatment regimen. Most patients do not have cirrhosis and can be treated easily in general practice.
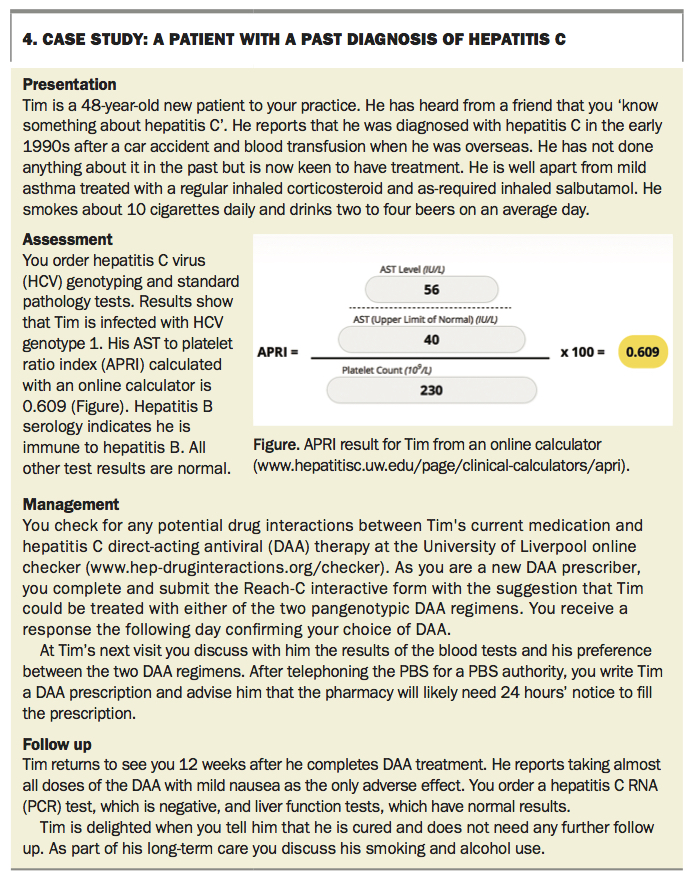
Steps in patient assessment for advanced liver disease are shown in the Flowchart.9 A simple assessment that can be performed with the results of a full blood count and liver function testing is the aspartate aminotransferase to platelet ratio index (APRI). APRI calculators are available online (e.g. www.hepatitisc.uw.edu/page/clinical-calculators/apri). If the APRI score is less than 1.0 then cirrhosis is unlikely, and the patient can be treated without further investigation (see the case study in Box 4). If the APRI score is 1.0 or more then the patient needs further assessment.
{kind=link}
The most useful next investigation is transient elastography, such as FibroScan. In many parts of Australia, this investigation can be performed by a specialist nurse at the GP clinic or local hospital (Figure 2).
{kind=link}
Treat with DAAs
Hepatitis C treatment is straightforward, as described in Part 3 of this series.6 DAA therapy for hepatitis C became available in March 2016 and has continued to evolve. Treatment options are based on the national guidelines, Australian recommendations for the management of hepatitis C virus infection: a consensus statement (September 2018).3
The choice of DAA medication depends on:
- HCV genotype
- presence of cirrhosis
- patient’s renal function
- potential drug interactions and
- patient or provider preference.
Potential drug interactions can be checked using the University of Liverpool’s online interaction checker (www.hep-druginteractions.org/checker).
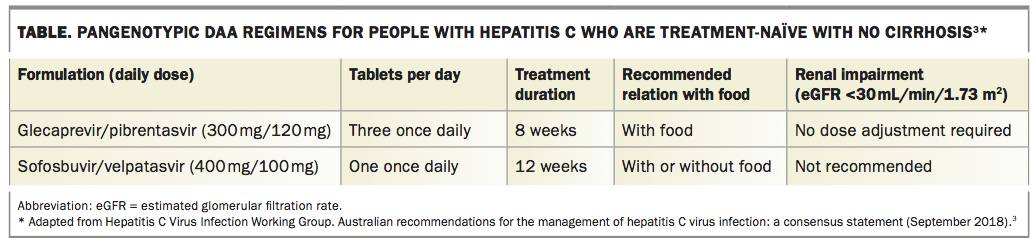
There are two regimens that can be used for any HCV genotype (pangenotypic). Their characteristics are summarised in the Table.
{kind=link}
Minimal monitoring is required during treatment. Many medical practitioners see the patient after four weeks to check on adherence and side effects, but pathology testing is no longer generally needed.
GPs who are not experienced in hepatitis C treatment need to have the treatment plan signed off by a specialist (gastroenterologist, hepatologist or infectious diseases physician). They can communicate with the specialist by telephone, email or fax. A proforma can be used, such as:
- Remote consultation request for initiation of hepatitis C treatment form from the Gastroenterological Society of Australia (http://cart.gesa.org.au/membes/files/Resources/Hepatitis%20C/
Remote_consultation_ form_updated_Aug_2017.pdf) - Reach-C interactive webpage (https://reach-c.ashm.org.au ).
Follow up
Follow up of patients is essential after DAA treatment, as described in Part 4 of this series.7 The key date for follow up is 12 weeks after completion of therapy.
A negative HCV RNA result at this time indicates hepatitis C cure, termed a sustained virological response (SVR12). This is truly a ‘miracle of modern medicine’ and a delightful message to convey to a patient.
Patients who are cured and have normal liver function test results and early liver disease need no further follow up, unless there is ongoing exposure to HCV, such as continuing injecting drug use. If liver function test results continue to be raised, indicating liver disease, or the patient has been diagnosed with cirrhosis then they need specialist review.
Patients with cirrhosis need lifelong monitoring with six-monthly liver ultrasound examinations because of the risk of hepatocellular carcinoma. Monitoring can be done by the GP or specialist. Built-in recall systems in GP software are helpful for this.
HCV reinfection is possible as past infection does not provide any immunity to reinfection. Patients with an ongoing risk of HCV infection (e.g. continuing injecting drug use) need regular HCV RNA tests at least once a year as long as they remain at risk. Note that the anti-HCV test will give positive results for life, and this test is thus not useful for monitoring for reinfection and does not need to be repeated.
Complete patient care
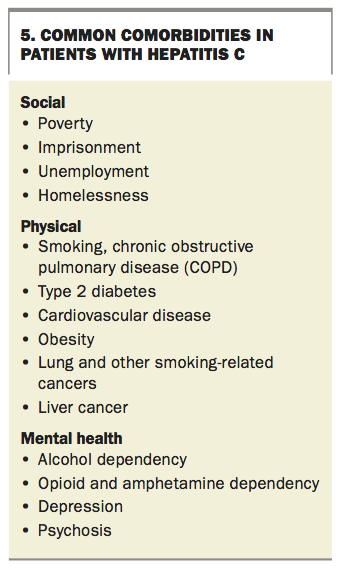
Most people living with hepatitis C have comorbidities.12 These can be:
- hepatitis C-related, such as cirrhosis, liver failure and type 2 diabetes
- associated with hepatitis C acquisition, such as injecting drug use and imprisonment
- associated with marginalisation and poverty, such as smoking, alcohol abuse and mental illness.
These problems require ongoing GP care and sometimes referral to other healthcare workers.
Some health problems that are more common in people living with hepatitis C are listed in Box 5. These health problems will probably persist after curative treatment of hepatitis C and impact on quality of life. Patient engagement in hepatitis C care can provide an opportunity to consider other health problems. Patients should be offered appropriate health screening according to the guidelines of the Royal Australian College of General Practitioners.13
{kind=link}
Preventing reinfection is important. This may include offering opioid substitution therapy and encouraging safer injecting (e.g. needle and syringe exchange). It is also helpful to encourage patients to support their partner and friends to access hepatitis C treatment, which will also reduce the likelihood of reinfection.
Treating hepatitis C around Australia
GP referral to a specialist is a longstanding model, and referral is appropriate for patients with advanced liver disease or major comorbidities, such as chronic hepatitis B or HIV infection. However, treatment of chronic hepatitis C for most people is now simple and can be easily incorporated into primary care. Less experienced GPs can obtain specialist support and advice on a treatment plan by contacting a specialist by telephone, by email using the Reach-C proforma or by fax using the GESA proforma.
Rural GPs may need to manage all stages of diagnosis and treatment of hepatitis C, including the care of patients with cirrhosis (Box 6). GP outreach models have also been developed, in which GPs provide assessment and care in the community, as described above (Box 3).
{kind=link}
Conclusion
Australian GPs are leading the world in curing hepatitis C. GPs can treat and cure most people living with hepatitis C with well-tolerated DAA therapy. Finding and treating patients with hepatitis C is straightforward and fits well with the skills that GPs use every day. Curing hepatitis C can be rewarding for the treating doctor as well as life changing for the patient. Eliminating hepatitis C from your practice is a great step towards hepatitis C elimination in Australia. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.