Death, dying and dementia – a pivotal role for the GP

Dementia
End of life issues
Identifying patients nearing the end of life is important so that patients, families and their GPs can prepare and work together to provide quality care and comfort to the patient according to their wishes and preferences.
- Dementia is a chronic, neurodegenerative, terminal illness with widely variable survival times of three to 12 years that make predicting death difficult.
- Throughout the course of dementia, the goals of care should be to improve quality of life, maintain as much function as possible and maximise the person’s comfort.
- A palliative care approach for patients with dementia should be implemented in a timely and personalised way, not in the last few days of life but in the last 12 months or even earlier.
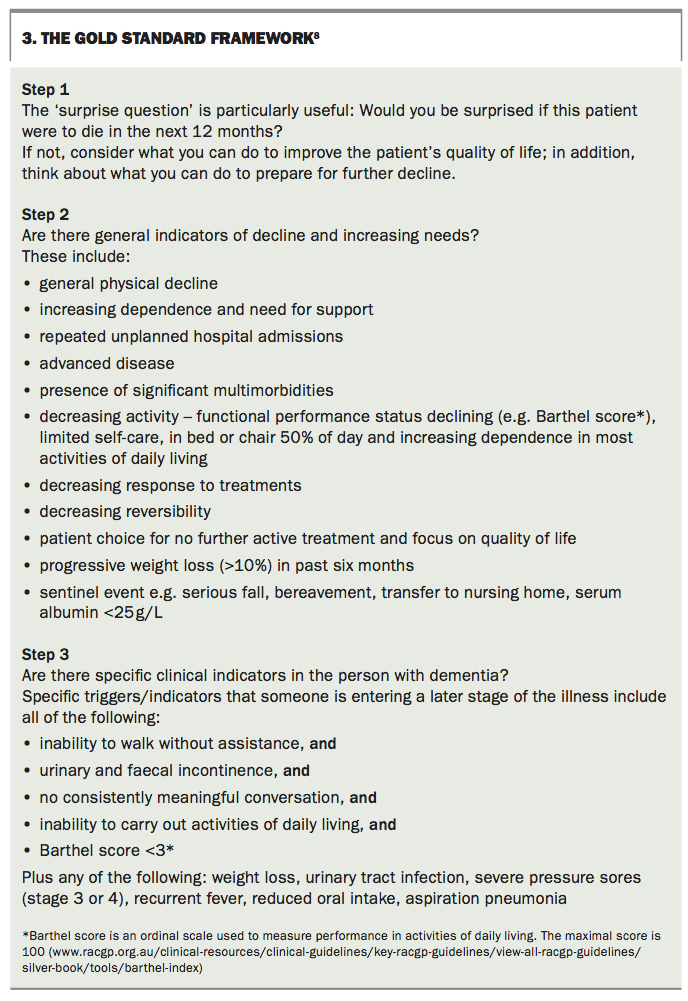
- The Gold Standard Framework is aimed at helping to identify people in the last year of life, and to assess their needs, symptoms and preferences and plan care on that basis.
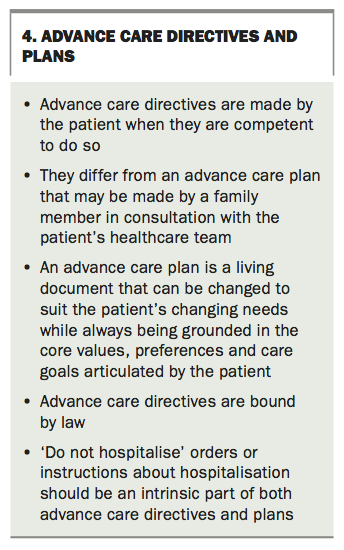
- An advance care plan needs to be distinguished from a legally binding advance care directive made by the patient; in many ways it can be more helpful because it is dynamic in accordance with the person’s needs.
- The key to managing behaviour change in patients with dementia is to work out the underpinning biological, psychological or social/environmental cause(s), including unmet needs.
- Effective pain management can not only provide relief from pain, but also relief from agitation in people with dementia.
What constitutes quality care at the end of life for terminal illnesses such as cancer is well defined. However, the needs of people living and dying with dementia are very different, and barriers to providing quality palliative care in this context are challenging for a number of reasons, not the least being the lack of recognition of dementia as a terminal illness and misinterpretation of what palliative care means. Considering the progressive functional and cognitive decline associated with dementia, it is essential to plan ahead for end-of-life care while the patient can still contribute to decision-making relating to their care. GPs are well placed to have these early discussions as they know the patient and their family well, and although not easy in practice, patients look to their GPs to initiate these conversations.
Dementia is a terminal illness. In Australia in 2017, dementia was the leading cause of death in women and the third leading cause of death in men.1 Dementia shortens life, although progression is widely variable depending on the timing of diagnosis, the disease type and comorbidities.2 Healthcare professionals therefore need to be skilled and prepared in dealing with dementia at the end of life. Management of death and dying in dementia is intrinsically part of the clinician’s role, particularly for GPs who are usually in it for the long haul with their patients.
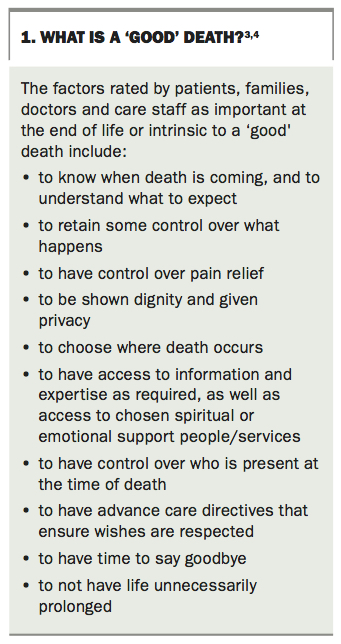
Quality of dying is the number one priority of care towards the end of life. However, what quality of dying means to the patient, their family, their doctor and their care staff varies greatly. Factors rated as important at the end of life or intrinsic to a ‘good’ death include, for example, being in control, mentally aware, free from pain and at peace with God, knowing when death is coming and what to expect, being shown dignity and given privacy, choosing where death occurs and having time to say goodbye and access to expertise (Box 1).3,4 As variable as these are, they are differentially ranked as important by patients, doctors, families and care providers.3 Therefore, achieving a consensus for goals of care that are driven by the patient’s will and preferences is an important clinical goal for end-of-life care in dementia. The best death is the one that is wanted by the patient and the family. Human rights of equitable access to health care, to the relief of distress and pain and to autonomous decision-making are at stake here.5
{kind=link}
In order to achieve such a consensus while honouring the patient’s ‘will and preferences’, clinicians need to talk about death and dying sooner rather than later.5 However, there are significant constraints that limit communication about death and dying between patients and their doctors. Some clinicians avoid dealing with death and dying until it is imminent, which poses a considerable barrier to providing the best end-of-life care.6 Dementia is often not perceived as life-limiting, which means a palliative approach to care may be lacking.2 How can discussions about treatment limitations, fears, timing and place of death – all considered priorities by patients – ensue, if discussions about death and dying are not on the table?3
It is crucial to provide timely, personalised and appropriate end-of-life care to all patients with dementia. Throughout the course of dementia, the goals of care should be to improve quality of life, maintain as much function as possible and maximise the person’s comfort. Although particular goals will change over time, these priorities should be consistent at all stages of the illness, including the end of life.7
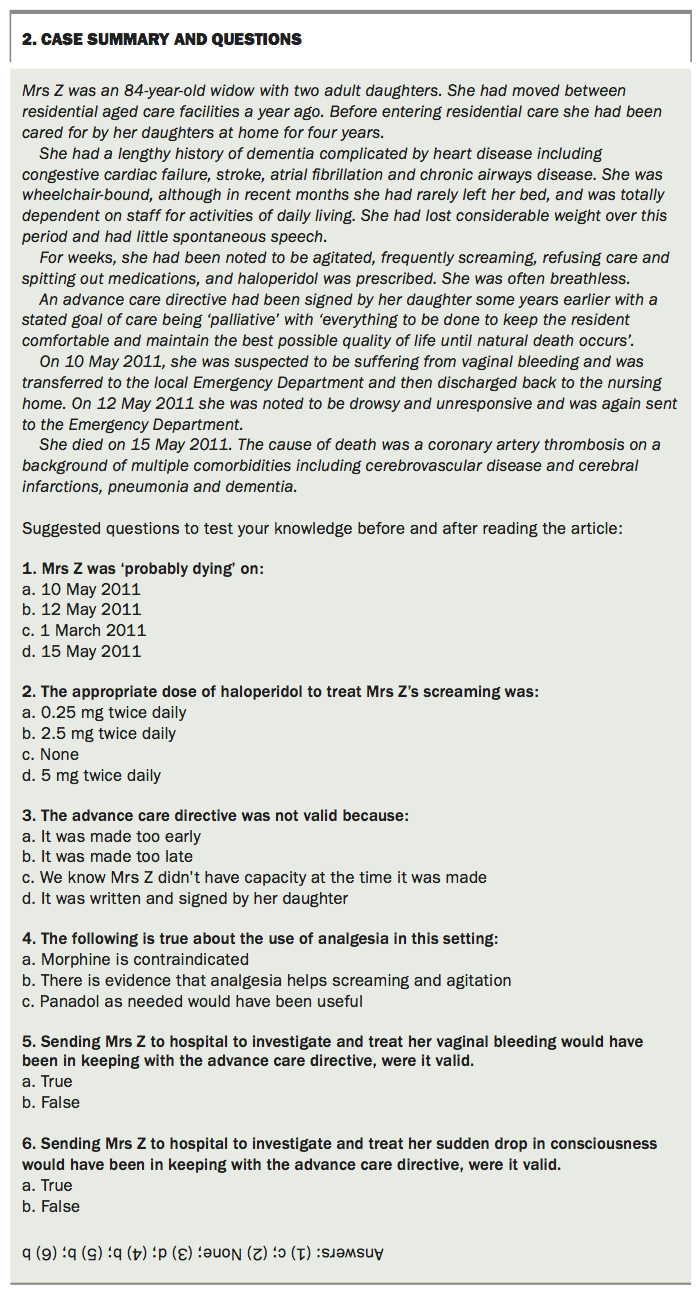
In this article, we seek to provide a practical guide to GPs for achieving the best possible quality of dying for their patients with dementia. We outline an approach to the ‘when’ and ‘how’ of discussing death and dying, the role of palliative care and the importance of understanding advance care planning and end-of-life law in the context of dementia. We suggest that, before you read the article, you test your current understanding by answering the questions in Box 2, then repeat the quiz for self-assessment after reading the article.
{kind=link}
Initiating discussions about death and dying
Sooner rather than later
Earlier identification of people nearing the end of their life benefits patients, carers and healthcare professionals alike. The Gold Standard Framework (GSF), first developed in the United Kingdom in 2000 from within primary care, is aimed at helping to identify people in the last year of life, and to assess their needs, symptoms and preferences and plan care on that basis (Box 3).8 According to the GSF, benefits of doing so for patients and carers include:
{kind=link}
- enabling patients to have more involvement and control over their care, fostering a collaborative approach
- allowing patients to let carers, family and healthcare professionals know their wishes, highlighting patient choices
- helping patients to set their own goals, priorities and expectations for future care
- allowing more time to be prepared for the future, discuss important issues and get their affairs in order
- increasing the likelihood that people will live and die in the place and manner of their choosing.
Being in control over choices at the end of life is a priority for patients;3,4 however, institutional deaths, which comprise 86% of deaths, are often associated with a perceived lack of control.9 When discussions about death and dying are delayed or avoided, people and their families do not have the opportunity to prepare for death, and the quality of death is rated as poor.9 Further, effective communication at the end of life has been linked to improved patient outcomes such as pain control, adherence to treatment and psychological functioning in patients.10 How well patient wishes are followed and treatments are explained is associated with higher-quality dying.11 Conversely, when discussions are avoided or delayed, referral to palliative care services can be perceived as a sign of impending death, inducing fear and uncertainty in patients and families.12 Anecdotally, we have found that late referral to palliative care is often rejected by families for exactly this reason.
The World Health Organization – supported by the Australasian Chapter of Palliative Medicine – defines palliative care as ‘an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual’.13
The key phrase here is ‘early identification’, and this applies equally to dementia as it does to cancer and other more obvious life-threatening diseases. The role of any clinician involved in dementia care is to demystify palliative care and to educate patients and families that a palliative approach does not signal impending death (or worse still, ‘stopping treatment’), but rather prioritises quality of life as the target of treatment.
Early discussions of death and dying benefit healthcare professionals by:8
- reducing the risk of a reactive crisis intervention through proactive planning
- helping clinicians to make the most appropriate decisions
- facilitating good communication and coordinated, person-centred care
- reducing the risk of unwanted hospitalisations or interventions
- helping to plan allocation of services and resources
- providing a common language for professionals involved in end-of-life care.
For these reasons, a ‘diagnosis of dying’ is no longer limited to the last hours or days of life or when death is imminent.
The place of prognosis
Dementia is a chronic, neurodegenerative disease with widely variable survival times of three to 12 years that make predicting death difficult.14 The GSF Prognostic Indicator Guidance states that people are approaching the end of life when they are likely to die within the next 12 months – giving rise to the ‘surprise question’ (Box 3).8 This is a rough indicator only and meant to act as a trigger for discussion. Using this approach, on the one hand, the family is not blindsided by discussions pre-empted by impending death, and on the other hand, death is not ‘diagnosed’ too early.
Clinicians need to recognise the limitations of prognostication: that it does not provide an accurate prediction of death but can be used as an impetus for starting discussions about death. It especially provides an opportunity to discuss previously expressed end-of-life wishes, ideally articulated earlier in an advance care directive (see below) when the person was more able to participate in discussions.
Why is it so difficult to discuss death and dying?
Although the GSF provides a guide to the appropriate timing of discussions about death and dying, this does not mean that patients and families will always want to talk about death and dying. For some, such discussions are catastrophic. Discussing death and dying is usually more distressing for families than for patients. Yet, many patients want GPs to take the initiative to discuss end-of-life issues, and welcome the opportunity.10
GPs may be best placed to have discussions about death and dying, but it is not always easy for them. Perhaps the biggest obstacle for the clinician in talking about death and dying is their own feelings. Many doctors feel uncomfortable talking about death and dying, sometimes because of their own ‘death anxiety’, particularly among those who have had less involvement with deaths, or because of a sense of therapeutic failure.15 As a result, doctors may overestimate the chances of recovery, or focus on treatments to prolong life.
Given the uncertainty of prognostication, it is easier and more appropriate to introduce the concept of moving towards the end of life while focusing on what is important, namely, the goals of care and quality of life. The framework’s concept of ‘living well and dying well’ can be useful for this.
Areas to consider after discussions have been initiated
Meeting preferences and determining goals of care
Standard 3c of the revised Australian Aged Care Standards requires that ‘the needs, goals and preferences of consumers nearing the end of life are recognised and addressed, their comfort maximised and their dignity preserved’.16
Providers are expected to ensure that:
- the person’s needs, goals and preferences for their end-of-life care are reflected in their care and services plan, including the situation, environment and place where they wish to die
- processes are in place to support conversations with the person (and others they may nominate) about their cultural, spiritual and physical needs
- there is a timely response if a person is in distress in order to relieve or prevent suffering and maintain dignity at the end of their life.
These standards highlight the importance of meeting the goals and preferences of patients. Ideally, these have been articulated earlier by the patient in an advance care directive before death and dying has been ‘diagnosed’. An advance care directive is a legal document written by the person (not by their family) that can be used to communicate specific instructions about types of treatment (including refusal of treatment) or to communicate general care or treatment preferences (e.g. place of death). This allows healthcare professionals to understand and respect the person’s wishes and preferences in the event that they cannot make them known. Because they have a holistic understanding of patients, their illnesses and their families, GPs are the best-placed professionals to work proactively with people to develop advance care directives.17 A toolkit and training package has been designed to equip GPs, practice nurses and practice managers in Australia to support advance care planning and palliative care in everyday general practice (www.theadvanceproject.com.au/tabid/5218/Default.aspx).
For an advance care directive to be valid, it must be made by a person with capacity to make one (competent to make an advance care directive).18 Clinicians must follow a valid and applicable advance care directive, and may be liable under civil and criminal law if they do not.19
In people with late-stage dementia, when death and dying is usually diagnosed, the ability to give consent for such complex decisions as making an advance care directive may be lacking, although this capacity always needs to be tested. It can be assumed that a previously made advance care directive was validly and competently made. If, after testing, the person is found to lack capacity to make an advance care directive, a collaborative advance care plan should be made instead, involving the person (as far as possible), their family, their doctor and senior care staff. An advance care plan made in this way needs to be distinguished from a legally binding advance care directive made by the patient (Box 4). In many ways an advance care plan can be more helpful, because it can, and needs to be, dynamic in accordance with the person’s needs. The model of care of the European Association for Palliative Care stresses the importance of changing care goals throughout the course of dementia.20 Recognising this, we suggest that competent patients who draw up advance care directives could be encouraged to include a statement aimed at canvassing wider opinion as their disease progresses to enable the dynamic and multitudinous facets of their disease to be addressed while respecting the initial expressed autonomy of the patient.
{kind=link}
It is important in this process to understand that even in the absence of capacity to make a directive, the person may still have capacity to make smaller, less complex decisions, including articulating their wishes, that help shape goals of care. They have a right to supported decision-making to facilitate their involvement in their own end-of-life care.21 When this is not possible, substitute-decision-making regimens in all states and territories in Australia are used to determine who the appropriate decision-maker is.18 Decision-making at the end of life, although guided by healthcare professionals, is never solely in the hands of the medical practitioner, or the residential care facility (RCF) or aged-care provider.
One of the most important and relevant instructions in an advance care directive for patients in RCFs is the ‘do not hospitalise’ order.18 This is often overlooked, and much confusion ensues when the person who is not for resuscitation or active treatment is sent to the emergency department. Few families understand the adverse effects of hospitalisation for someone with dementia. Transfer to hospital in the last 12 months of life is not necessarily conducive to quality of life and in many instances triggers great distress.22-25
Australian research has shown that doctors have significant gaps in knowledge about the law on withholding and withdrawing life-sustaining treatment from adults who lack decision-making capacity.19 For medical professionals, criminal responsibility could arise for murder or manslaughter (where treatment is withheld or withdrawn unlawfully) or for assault (where treatment is provided without consent).19 Some helpful resources explaining end-of-life law are listed in Box 5.
{kind=link}
Palliative care and symptom relief
Equitable access to palliative care, including pain relief, is a human right owed to all, including those in residential care. Pain is common in older people, particularly those in RCFs, and those with dementia.26-28 The difficulty is that by the later stages of dementia, there are a number of obstacles to the identification and consequent relief of pain, not the least of which include the patient’s dysphasia, rendering it difficult to articulate the experience of pain.
A laborious pain-communication chain exists between the experience of pain and its relief in RCFs, as patients with severe dementia do not press a buzzer and request ‘prn paracetamol’.29 Instead, pain or any distress or discomfort in patients with severe dementia will often manifest as behavioural and psychological symptoms of dementia (BPSD), such as screaming, resistance to care, agitation, insomnia or aggression.30 Accordingly, effective pain management can not only provide relief from pain, but also relief from agitation in people with dementia.31 There is current debate around the use of the term BPSD for this reason – the agitation or other behavioural manifestation is not a symptom of dementia but an expression of an unmet need, in this case the need for pain management.
Among 175 nursing home residents with moderate to severe dementia, individual daily treatment of pain for eight weeks according to a stepwise protocol beginning with paracetamol then using either morphine, a buprenorphine transdermal patch or pregabalin significantly reduced agitation. The effective management of pain also reduced other neuropsychiatric symptoms, potentially mitigating the requirement for harmful medications such as antipsychotics.32
Additionally, behaviours and psychological symptoms, such as anxiety or paranoid delusions, may cause distress or suffering at the end of life. Aggression may interfere with the provision of care and again lead to the inappropriate use of antipsychotics or other psychotropic medications to ‘manage’ aggressive residents in RCFs. It is crucial to understand and manage behaviour change and psychological symptoms at the end of life, including the last 12 months of life, when quality of life is a priority.
The key to managing behaviour change is to work out the underpinning biological, psychological or social/environmental cause(s), including unmet needs (Box 6). Best practice for treating BPSD is first-line nonpharmacological management, rather than reaching for the prescription pad, which should be reserved for severe behaviour that puts the person or others at risk. Consider the following:
{kind=link}
- Is the person unwell?
- Do they need something and can’t express it?
- Are they in pain, frightened or lonely?
This is very individual and may also be influenced by personal life experiences, hence ‘person-centred care’ is necessary. Information and resources on managing behaviour change and person-centred care are available online at https://empoweredproject.org.au. Important causes of distress at this stage include pressure injuries and neglect of oral care. The usual palliative approaches must be assiduously adhered to, as the total symptom burden is similar to that in those dying with cancer.2
People with advanced dementia are usually bed-bound and at risk of pressure sores and contractures, variably interested in food yet at risk of aspiration and infections.33-35 There is little evidence that artificial hydration and nutrition improve nutritional status, reduce the risk of aspiration pneumonia, prolong life or enhance quality of life.2 This may be one of many ways that approaches to palliative care in dementia need to be differentiated from approaches to other terminal illnesses such as cancer. Until now, end-of-life care for people with dementia has been borrowed from other disease states. However, there is a need to establish best practice palliative approaches specific to dementia, as the needs of patients are very different (e.g. multiple comorbidities, frailty and variable capacity for making important decisions about their care).
A set of quality indicators has been developed using a robust framework that provides clear definitions of aspects of palliative care that are dementia specific, although there are recognised gaps where quality indicators are still lacking. These gaps are related to behaviour changes, including appropriate pharmacological management and implementation of nonpharmacological, psychosocial strategies in care, all of which are fundamental to comfort and quality of life for people with dementia.36 A range of psychosocial interventions including music therapy and life review have been shown to reduce emotional and existential distress and improve quality of life at the end of life.37
Finally, dementia is a risk factor for delirium, and it is a common end-of-life complication in people with dementia. Delirium is distressing for patients, families and caregivers alike.38 Medications such as antipsychotics will not necessarily relieve this distress and can worsen symptoms. In patients receiving palliative care, individualised management of delirium precipitants and supportive strategies are more efficacious in treating distressing delirium symptoms than risperidone or haloperidol.39
Notwithstanding the variable availability and quality of palliative care in RCFs, for some, living and dying in a nursing home can be a positive experience because of the potential to develop long-term relationships with staff and other residents and the demedicalisation of the patient’s experience, especially their dying experience.40,41 This is particularly why it is preferable for patients to avoid hospitalisation at the end of life, providing that the facility can provide a quality dying experience and is committed to doing so.
Dealing with family distress and conflict
At the end of life conflicts may occur within families, between families and health professionals and between treating teams.42 Conflicts can lead to delays in decision-making, and can prolong a person’s discomfort, distress or pain. Family discord is associated with stronger preferences for life-prolonging treatments, and weaker preferences for palliative care.43 Conversely, increased family satisfaction with decision-making and feeling supported during decision-making is associated with withdrawing life support and the documentation of palliative care indicators.44 Another potential source of conflict that needs to be understood by clinicians is the variety of values and preferences among racially or ethnically diverse groups.45 As advocated above, earlier discussions and consensual decision-making can help prevent conflict, or at least not feed conflict. The experience of end-of-life care in dementia can be improved through the provision of sensitive and timely information about the natural progression of dementia, so that people know what to expect.46 This can also minimise and prevent any underlying conflict that may be present.47
Conclusion
GPs have a key role to play in identifying patients nearing the end of life, so that patients can receive quality care and comfort that is based on their own wishes and preferences. For this to occur, GPs need to talk about death and dying sooner rather than later – this will help to ensure that patients and their families can plan ahead for end-of-life care in dementia that is timely, personalised and appropriate. Earlier discussions can also help people to know what to expect and minimise potential conflict. Although this may not be easy in practice, patients often look to their GPs to initiate these conversations. It is therefore important for GPs to understand their own resistances to fears about discussing death and dying and to follow a palliative care approach with a focus on providing adequate symptom relief, maximising comfort and maintaining quality of life. MT
Acknowledgement
This is a piece of work from the Empowered Project supported by funding from the Australian Government under the Dementia Aged Care Services Fund.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.