Death certificates: to sign or not to sign

This series highlights common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, the series is based on actual cases, with details changed for privacy and some issues summarised for the sake of discussion. In this scenario, a locum GP is asked to complete a death certificate for a patient who dies suddenly in an aged care facility. It explores potential medicolegal issues for doctors, particularly when the death is unexpected or they do not know the patient well.
The death of a patient, particularly if unexpected, may require doctors to navigate several medicolegal issues. In many cases, doctors will need to decide whether they can complete the medical certificate stating cause of death (‘death certificate’) or whether the death needs to be reported to the Coroner.1 The task of completing a death certificate often falls to junior hospital doctors, GPs and locums, who may feel under pressure to sign the death certificate so as to avoid delays and distress for the patient’s family. Even in more straightforward situations, the law can be confusing, and doctors can be unsure about their obligations. The following scenario involving a patient who dies unexpectedly in an aged care facility illustrates some of the pitfalls that GPs can encounter.
Case scenario
Dr Kay works as a locum GP in a regional centre in NSW. The practice where she works provides GP services for several aged care facilities in the wider region. Late one evening, a nurse at one of these facilities telephones to ask the GP on call to complete a death certificate for an older patient. The nurse explains the staff found the patient, Mrs Long, sitting in the garden and believe she died of heart failure. Her family were relieved to hear she died peacefully. They are with her now and anxious to transfer her body to the funeral home as quickly as possible.
Dr Kay checks Mrs Long’s patient records and sees that she is a longstanding patient of the practice. She was diagnosed with vascular dementia many years ago and has a history of heart failure. Her dementia has been progressively deteriorating.
Dr Kay is unable to contact Mrs Long’s regular GP, who is travelling for several weeks, and decides to drive out to the aged care facility. An hour later, Dr Kay arrives to find a large family group gathered around Mrs Long’s bed in some distress. She does not want to disturb them unnecessarily so does not examine Mrs Long’s body; nor does she ask any further questions of the nursing home staff or check the nursing home patient records. She completes the death certificate, recording ‘heart failure’ as the cause of death.
A few days later, Dr Kay is visited at the general practice by police asking her for a statement for the Coroner in relation to Mrs Long’s death. She later learns that a staff member of the aged care facility disclosed that Mrs Long may have died as the result of an accident, and the police were contacted. The Coroner is now investigating.
Medicolegal issues
A range of health professionals, including nurses, midwives and paramedics, can verify ‘life extinct’ in some states. However, the Medical Certificate of Cause of Death (death certificate) must be completed by a doctor, or the death must be reported to the Coroner. Completing the death certificate often raises questions for doctors including:
- whether they can sign a death certificate without examining the body of the deceased
- what they can do if they are uncomfortable about completing a death certificate
- what they should record on the death certificate, particularly in the case of patients who are older or who have complex comorbidities, where identifying a single cause of death can be difficult
- whether and in what circumstances they can amend a death certificate
- whether they should record anything in their patient records.
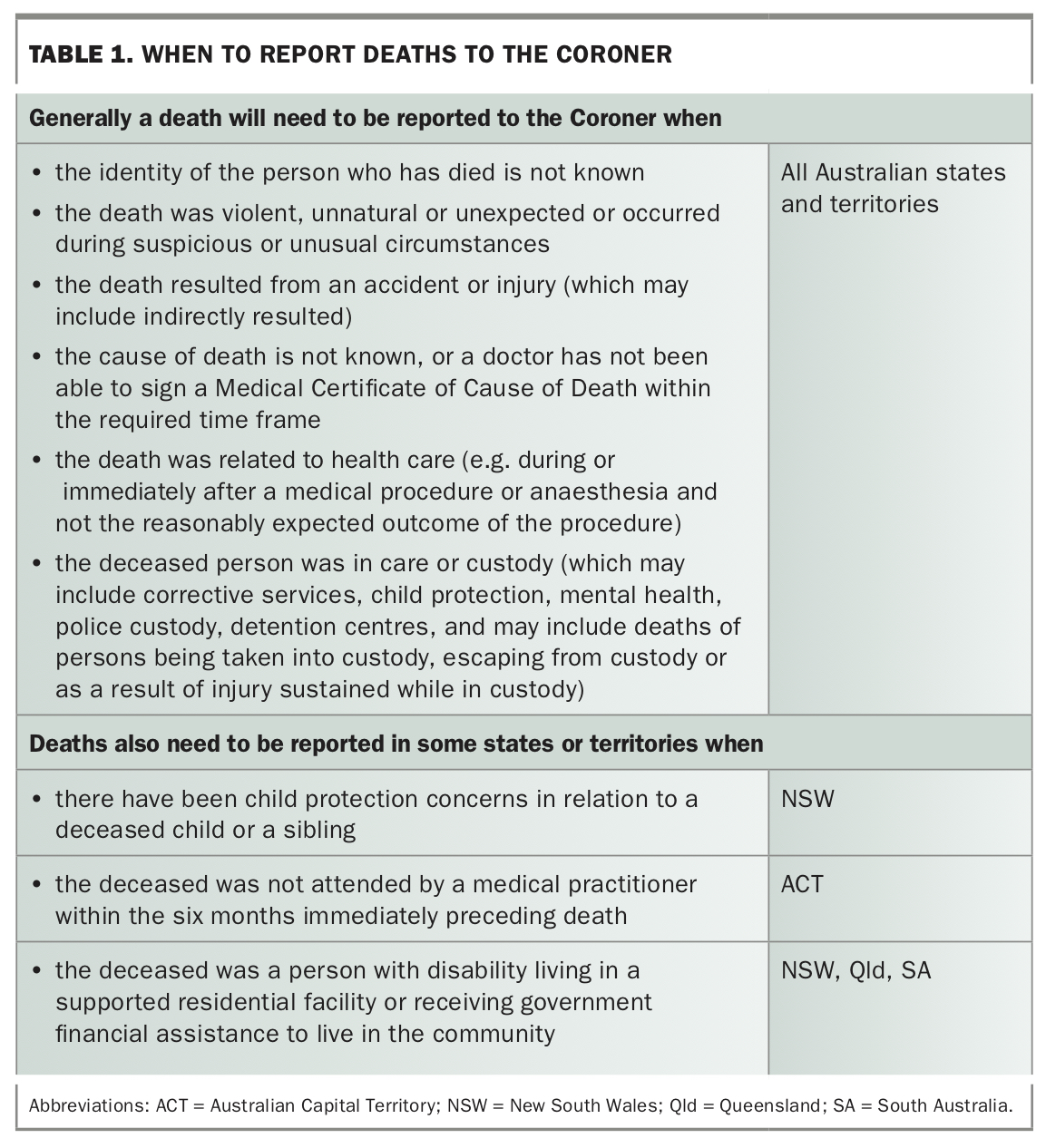
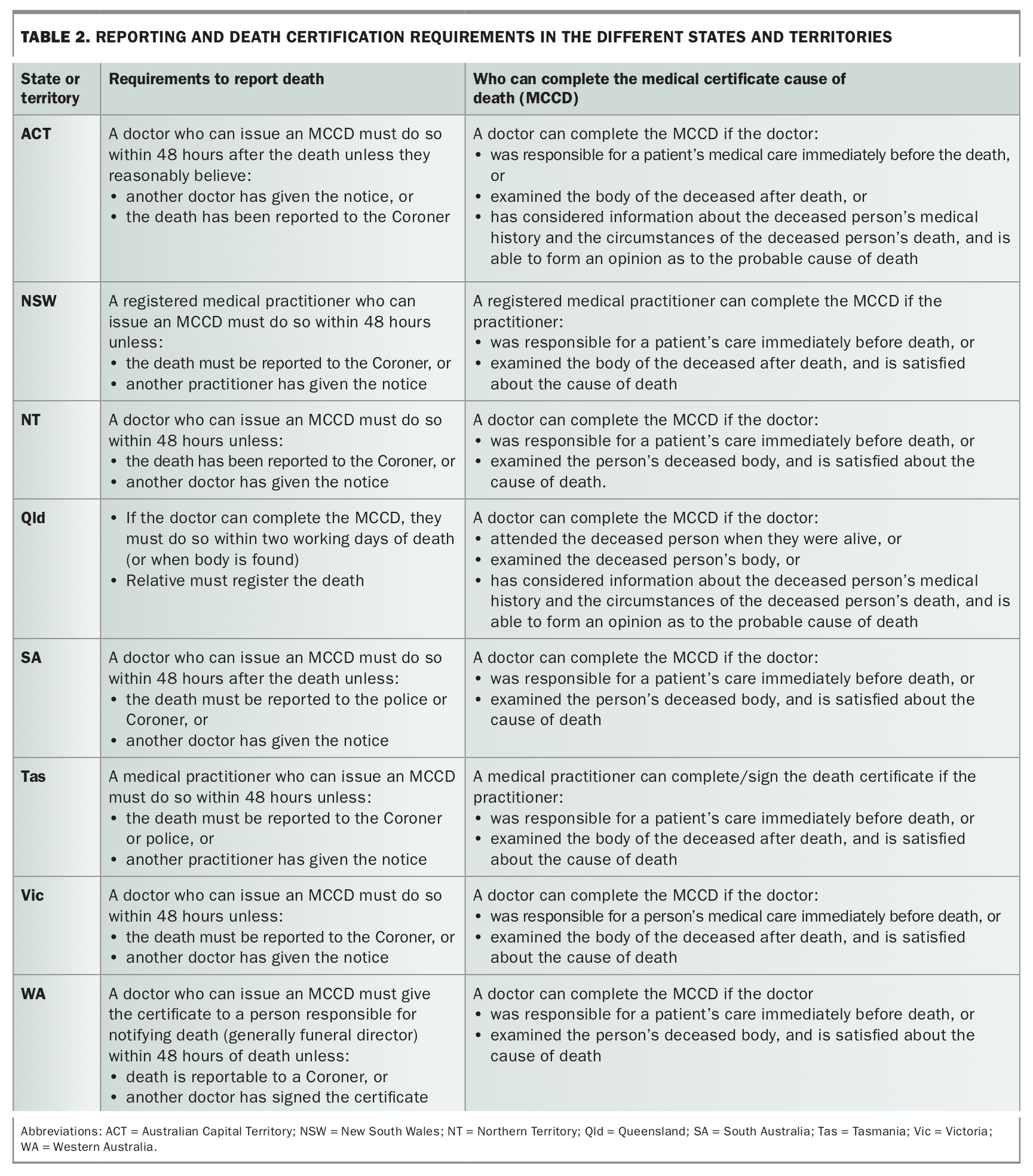
The relevant laws differ between Australian states and territories, and it is important to check the legal position in your place of practice (see Table 1 and Table 2). However, some general principles apply in all jurisdictions.
{kind=link}
{kind=link}
Discussion
Certain deaths must always be reported to the Coroner, including deaths that are violent or unnatural, that occurred in suspicious circumstances, or where the identity of the patient or the cause of death are unable to be determined (see Table 1).
Who can complete the death certificate?
In cases where the death is not required to be reported to the Coroner, the death certificate can be completed by one of the following:
- the doctor responsible for the person’s medical care immediately before death
- any doctor who can comfortably determine the cause of death, including:
– a doctor from the same practice as the doctor responsible for the person’s medical care who has access to the patient’s medical record
– a doctor who saw the deceased after death, has sufficient information (e.g. through review of the medical record or discussion with the treating doctor) and is satisfied about the cause of death.
Do you need to examine the body of the deceased before completing a death certificate?
We strongly recommend that doctors examine the body of the deceased before issuing a death certificate. Examination is not always legally required (see Table 2). However, without an examination it can be difficult to determine the cause of death or to assess whether the death needs to be reported to the Coroner. Doctors can find their conduct coming into question if they issue a death certificate and later there are questions about the cause of death.
Two questions are key for doctors when deciding whether to issue a death certificate:
- Are you are satisfied the death does not need to be reported?
- Are you are comfortable that you are satisfied with the cause of death, through your knowledge of the patient, review of the records or examination of the body?
What can you do if you are unsure about issuing a death certificate?
In all states and territories except Queensland, a doctor is required either to complete the death certificate or to report the death (to the police or the Coroner) within 48 hours of the death occurring if:
- the doctor has been called about the death of a patient they were treating immediately before the death; or
- the doctor has attended and examined the body of the deceased patient.
Queensland has a provision where doctors can certify that life is extinct, even if they are unable to certify the cause of death. For more information on requirements for your state or territory, see Table 2.
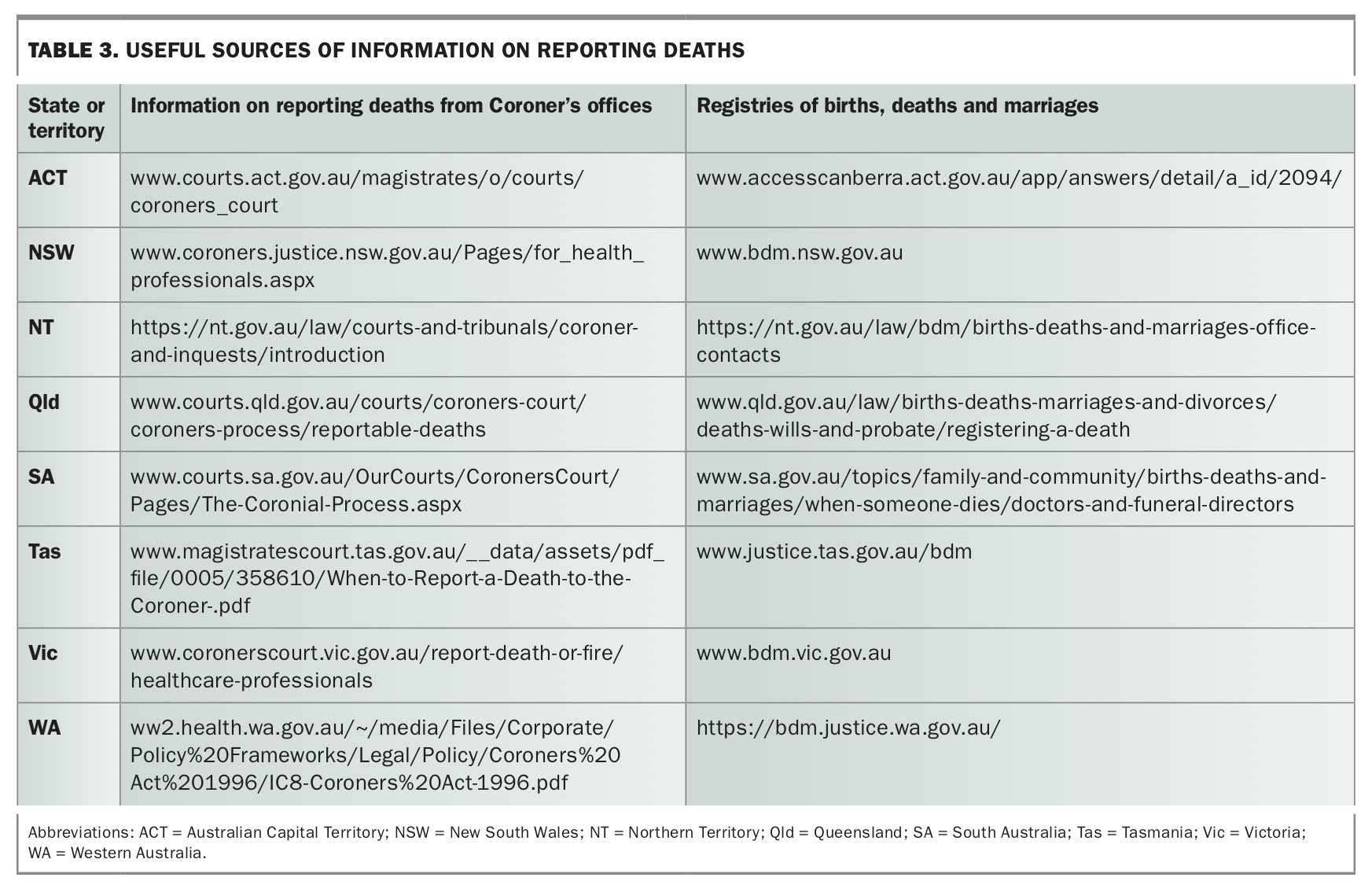
Sometimes, doctors report that they feel pressure to sign the death certificate so that the body can be moved. Based on experience at our medical defence organisation, we strongly advise doctors to seek advice if they are not comfortably satisfied of a natural disease or condition that is more likely than not to have led to the death, or if they have any concerns that the death might need to be reported to the Coroner. Doctors should consider contacting their medical defence organisation. In many states, you can also contact the Coroner’s office for advice (see Table 3). In a hospital, doctors may also be able to contact the duty forensic pathologist.
{kind=link}
If your concerns are purely about the cause of death, you may also be able to contact the patient’s treating doctor who may be able to complete the certificate.
Always take careful notes of your discussions and any advice in case there are questions later.
What should you record on the death certificate?
The Medical Certificate of Cause of Death form is similar in each state and territory. Information in death certificates is collected for statistical reporting, and the form asks for information about the disease or condition leading to death, as well as any other significant conditions contributing to death.1 It also requires you to note the approximate interval between the onset of the condition and the death of the patient. This can become particularly important if questions are later asked about a person’s capacity.2
Part II of the form asks for any other significant conditions contributing to the death but not related to the disease or condition that led to death.
In the case of patients with complex comorbidities, it can be difficult sometimes to know the exact cause of death. In general, it is advisable to be as specific as possible about the disease or condition that directly led to the death and to provide as much information about the context. For example, if you know that the patient died of aspiration pneumonia associated with vascular dementia you would note both of these conditions on the certificate. You would only write ‘vascular dementia’ as the cause of death if you believed it was the cause and you did not have any information about which associated condition actually directly led to the death. As the scenario of Mrs Long illustrates, you should document a cause only when you have formed an opinion that this represents the most probable cause of death. Contacting the Coroner’s office for advice on completing the death certificate can be helpful in such cases.
Can you ever amend a death certificate?
Generally this question arises when the doctor is advised of an administrative error on the death certificate. Scenarios include where the legal name reported by the family is different to the name the patient is known by in the practice and on their Medicare card or where there has been a typographical error or a mistake with time or cause of death.
If you discover an error that means the death should have been reported to the Coroner, for example an error that means you are no longer sure of the cause of death or the identity of the deceased, you need to bring the error to the Coroner’s attention.
If the error is administrative only and does not change your ability to issue the death certificate, the error can be corrected and a new certificate issued. The old documents are still part of the medical record, so should not be destroyed or made illegible. The appropriate way to correct the document is to strike through the incorrect entry, mark it ‘written in error’ and print the author’s name, signature, designation, date and time.
If the certificate has already been provided to the Registrar of Births, Deaths and Marriages, each state registry also has a process for notifying the registry of the error. More information can be obtained from your local registry office.
What should you record in the patient records?
All aspects of the process involved in writing the death certificate should be recorded in the patient records. This is particularly the case if you decide you cannot complete a certificate because you are unsure about the cause of death. If you contact the Coroner’s office for advice, make careful notes of that discussion.
Outcome
In the case of Mrs Long, the death was the subject of a coronial inquest. Closed circuit television footage from outside the aged care facility showed that Mrs Long had tripped in the garden and fallen. She appeared to have lain there for nearly an hour before she was discovered by staff, who returned her to her room.
In this case, which occurred in NSW, the Coroner found that the actions of some aged care staff amounted to a ‘cover-up’, and that Dr Kay had been called to attend the facility and certify the death of the patient without being fully informed by staff of all that had actually occurred. The Coroner also noted the shortcomings in Dr Kay’s approach to certifying the death, in that she did not question the staff further, check nursing home records or examine Mrs Long’s body.
Conclusion
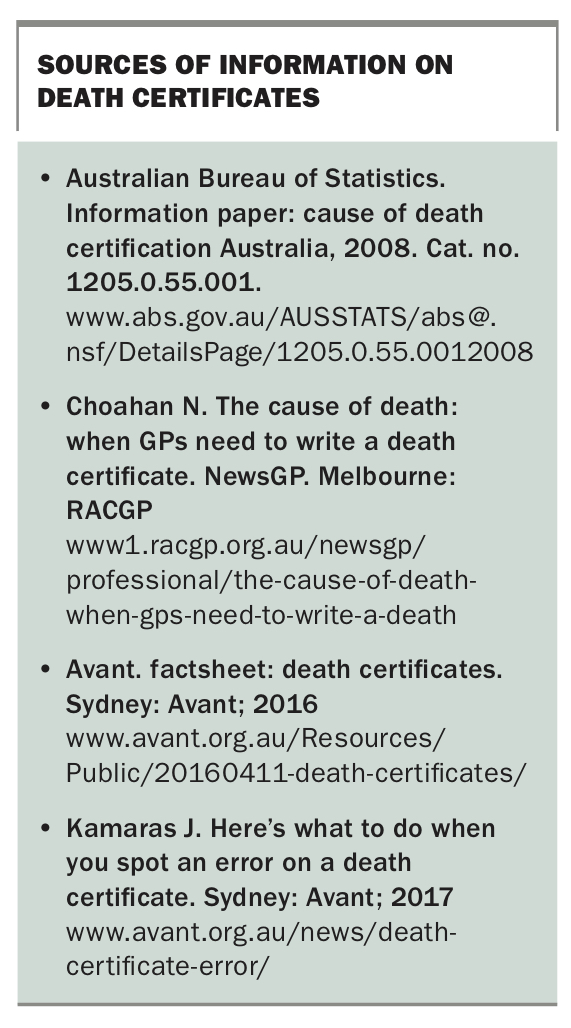
Certifying a patient’s death is an important part of a doctor’s role. Doctors may feel under pressure from the patient’s family or police to certify the cause of death. However, it should be remembered that certificates are also legal documents. If the death is reportable or you cannot confidently state you are satisfied as to the cause of death, you should not sign the certificate. Useful sources of information on death certificates are listed in the Box. If you have any doubts, seek medicolegal advice or contact the Coroner’s office. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.