Managing patients with rhinosinusitis

Rhinosinusitis is a common disorder that ranges from acute to chronic, with GPs at the forefront of patient management. There have been recent developments in the understanding of this heterogeneous disease, and as such it is important that GPs are aware of the latest medical and surgical treatments that have evolved in order to better inform and manage patients under their care.
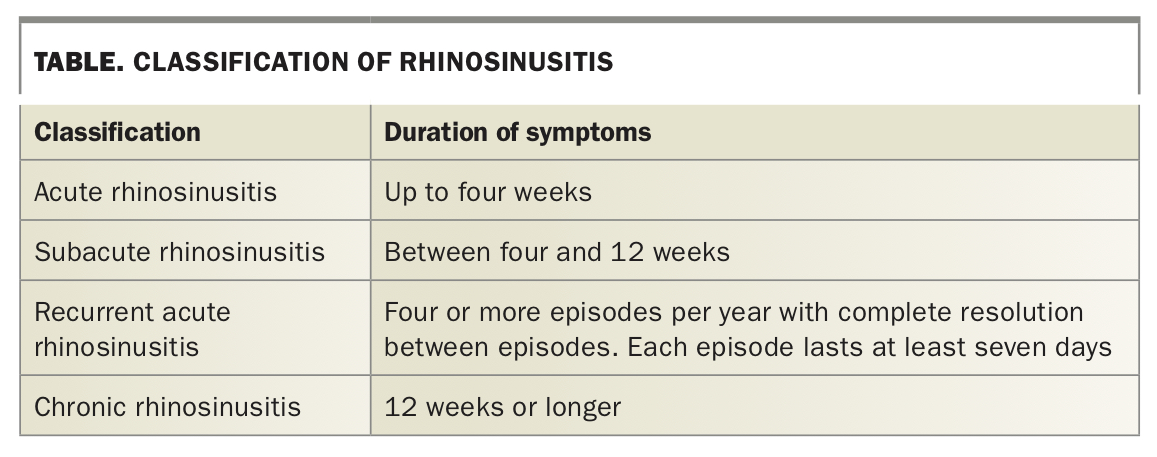
Rhinosinusitis is a common presenting complaint to primary care physicians. The term ‘rhinosinusitis’ describes a constellation of disease entities with a common feature – inflammation of the mucosa lining the nasal cavity and the paranasal sinuses. Rhinosinusitis is best characterised as acute, subacute, recurrent acute or chronic according to the duration of symptoms (Table). Acute rhinosinusitis (ARS) is estimated to affect between 6 and 15% of the population and a recent national health survey has shown that 10% of people in Australia suffer from chronic rhinosinusitis (CRS).1
{kind=link}
Acute rhinosinusitis
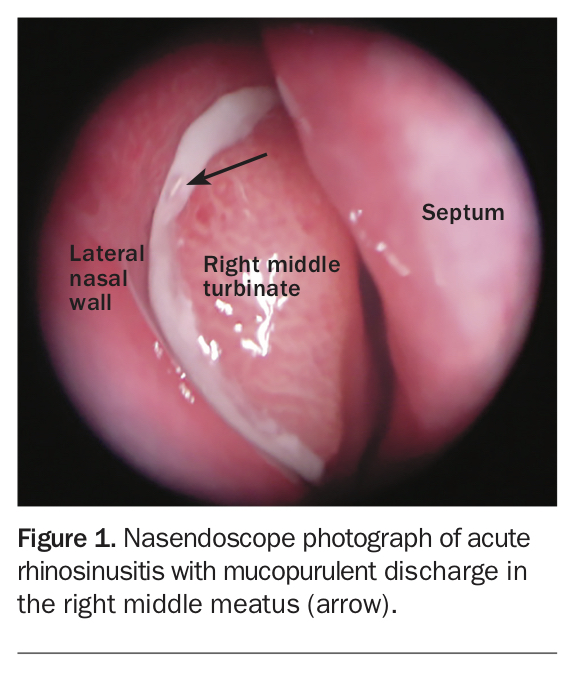
ARS is a common disorder that is frequently caused by an acute viral infection associated with the common cold, but bacteria have also been implicated primarily, or as a result of secondary infection after a viral upper respiratory tract infection (Figure 1). The principal bacterial pathogens involved in ARS are Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis and Streptococcus pyogenes.2 Key diagnostic criteria include symptoms after upper respiratory tract infection, purulent nasal discharge, unilateral maxillary sinus tenderness, maxillary tooth or facial pain and a history of initial improvement followed by a worsening of symptoms.3 Other nonspecific symptoms include malaise, halitosis, nasal congestion, hyposmia/anosmia, fever and cough. Allergic inflammation and cigarette smoking are thought to predispose patients to ARS due to decreased ciliary motility and function.
{kind=link}
Management of acute rhinosinusitis
Meta-analyses have shown that ARS resolves without antibiotic treatment in many patients.4 Symptomatic treatment and reassurance is the preferred initial management strategy for patients with mild symptoms as most of these are viral in origin. Antibiotic therapy should be reserved for patients with severe ARS, especially with the presence of high fever or severe unilateral facial pain (Flowchart 1).5 Medical practitioners need to weigh the moderate benefits of antibiotic treatment against the potential for adverse effects. For initial treatment, the most narrow-spectrum agent active against the likely pathogens (S. pneumoniae and H. influenzae) should be used. Amoxicillin is usually an excellent first-line therapeutic choice, with a beneficial effect seen in up to 90% of cases; amoxicillin/clavulanic acid has greater efficacy against beta-lactamase-producing H. influenzae, and can be used when amoxicillin fails. Treatment should be given for five days only as meta-analyses have shown no benefit from more prolonged therapy.
Intranasal corticosteroids are effective and can be used together with oral antibiotics. Oral corticosteroids are indicated for short-term relief of headache, facial pain and other acute symptoms. Surgery is reserved exclusively for complications of ARS such as orbital or intracranial spread.
Chronic rhinosinusitis
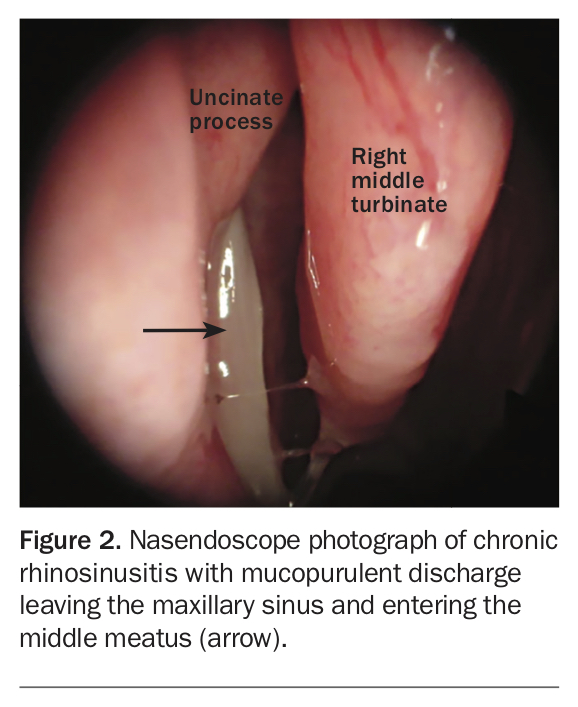
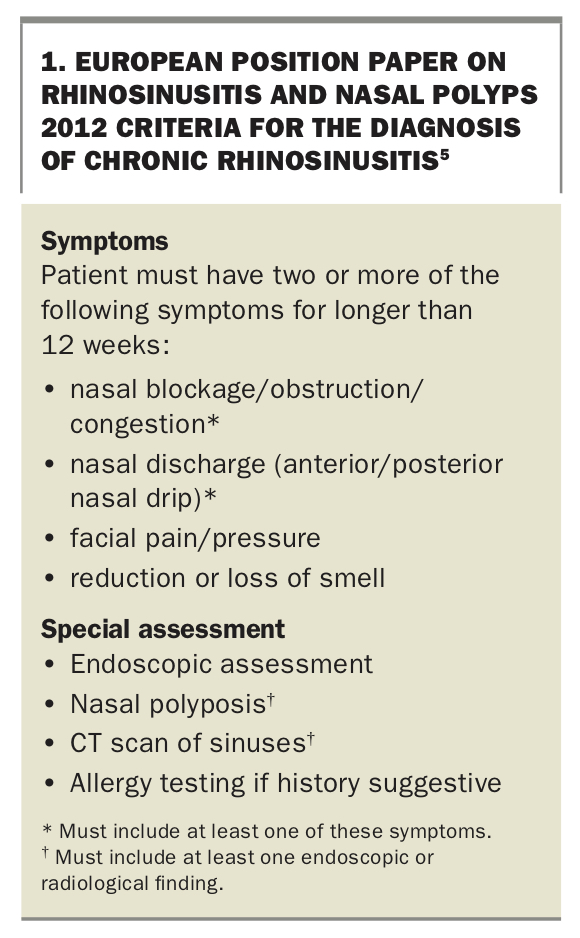
Although many of the symptoms are similar, understanding the distinction between the acute and chronic forms of rhinosinusitis has both clinical and scientific importance. In chronic rhinosinusitis (CRS) (Figure 2) the duration of symptoms is greater than 12 weeks, and although disease fluctuations occur, the signs and symptoms of CRS never completely resolve, setting CRS apart from ARS, subacute rhinosinusitis and recurrent ARS. Patients complain that it seems like they have a constant cold that never completely gets better despite multiple attempts at medical therapy. The criteria for the diagnosis of CRS are summarised in Box 1.5
{kind=link}
{kind=link}
CRS has significant socioeconomic implications, with an estimated annual direct health care cost in the US of $US 5.8 billion. Patients with CRS visit primary care clinicians twice as often as those without the disorder, and have five times as many prescriptions filled.6 CRS is the second most prevalent chronic health condition in the US.7-9 Although there are no directly comparable statistics for the Australian population, a recent study suggests that the productivity costs of CRS in the Australian context are higher than for common chronic conditions such as diabetes, chronic pain and migraine, and severe asthma, and represent a significant economic burden, estimated at almost $11,000 per patient per year.10 CRS is also extremely detrimental to the quality of life of those who have it, with quality of life measures similar to or worse than those for chronic obstructive pulmonary disease (COPD), chronic back pain and congestive cardiac failure.11
Management of chronic rhinosinusitis
Treatment of CRS is medical in the first instance, as outlined in Flowchart 2. Empirical antibiotics, systemic and intranasal topical corticosteroids and saline douches are used as the first-line treatment and about 30% of patients respond to this treatment alone. There is no agreed upon antibiotic regime for patients with CRS. In a multicentre randomised trial, amoxicillin/clavulanic acid (875 mg/125 mg twice daily) was shown to have a higher clinical response rate (95% vs 88%) and a lower relapse rate (0% vs 8%) than cefuroxime axetil (500 mg twice daily).12 In a double-blind study, ciprofloxacin and amoxicillin/clavulanic acid were shown to have similar clinical cure (60%) and bacterial eradication rates (90%).13 However, ciprofloxacin had a much higher cure rate at 40 days after treatment and with fewer gastrointestinal complaints. The author recommends low-dose doxycycline (100 mg daily) for 21 days. Doxycycline is a tetracycline antibiotic and confers immunomodulation at subantimicrobial doses. Doxycycline has been shown to reduce postnasal drip and the size of nasal polyps – an effect that is sustained for up to 12 weeks after treatment.14
Intranasal corticosteroids (INCS) and saline irrigations have been shown in multiple studies to improve symptoms and outcomes in patients with and without underlying allergic rhinitis. INCS should be continued after cessation of symptoms in patients with underlying allergic rhinitis to reduce the risk of further exacerbations. Immunotherapy might also be of long-term benefit in this group of patients.
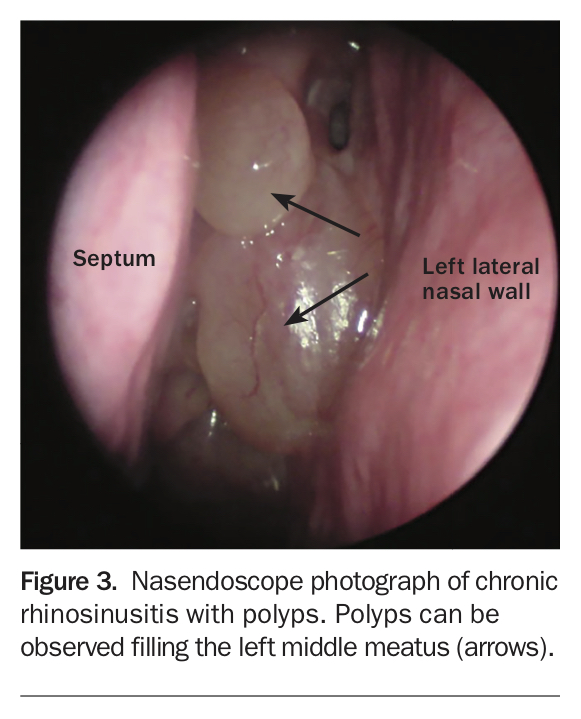
In patients with CRS with polyps (Figure 3), systemic corticosteroids are beneficial but the effect is often short lived and therefore their use must be weighed against the potential for long-term side effects. In CRS without polyps, there is some evidence to support use of long-term, low-dose macrolide antibiotics for 12 weeks. Patients with a normal serum IgE levels are most responsive to this treatment.5,15
{kind=link}
Role of surgery
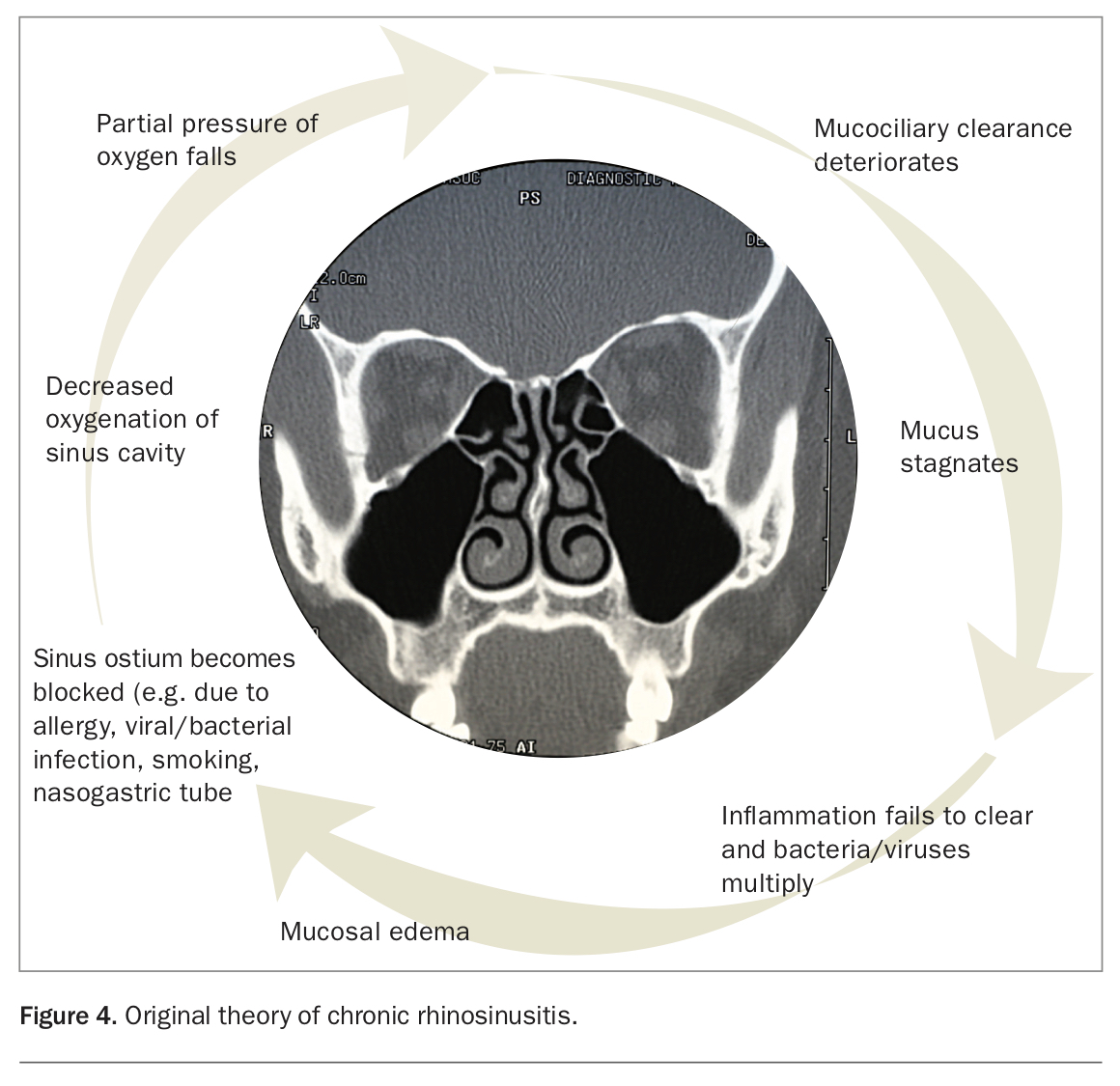
Until recently, CRS has been attributed almost entirely to lack of ventilation (Figure 4), with endoscopic sinus surgery (ESS) the accepted treatment of choice for CRS refractory to medical treatment. ESS has been shown to be a more effective intervention at improving overall quality of life at a lower overall cost compared with continued medical therapy for patients with refractory CRS.16,17 However, a small but nonetheless significant number of patients fail to see improvements in symptoms despite adequate ‘ventilation’ surgery and often undergo multiple surgeries without durable results.
{kind=link}
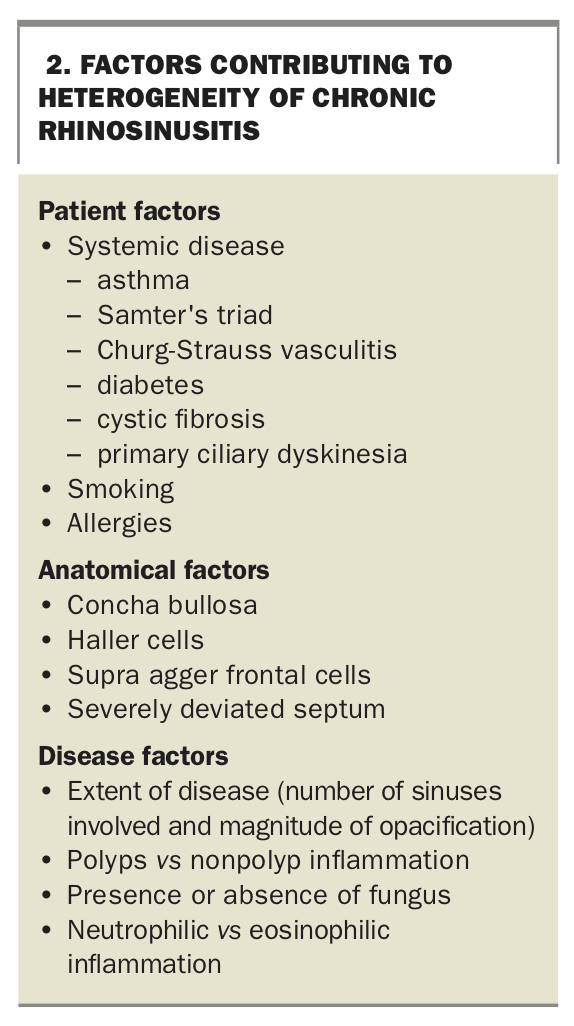
We now know that CRS is a heterogeneous disease and multiple factors contribute to inflammation of the sinuses (Box 2). The role of sinus surgery has therefore evolved to acknowledge that inflammation and mucostasis are the major pathophysiological processes involved in CRS. Surgery is merely a tool to intervene in this process. The goals of ESS are to reventilate the sinuses, remove inflammatory mediators and facilitate topical therapy.
{kind=link}
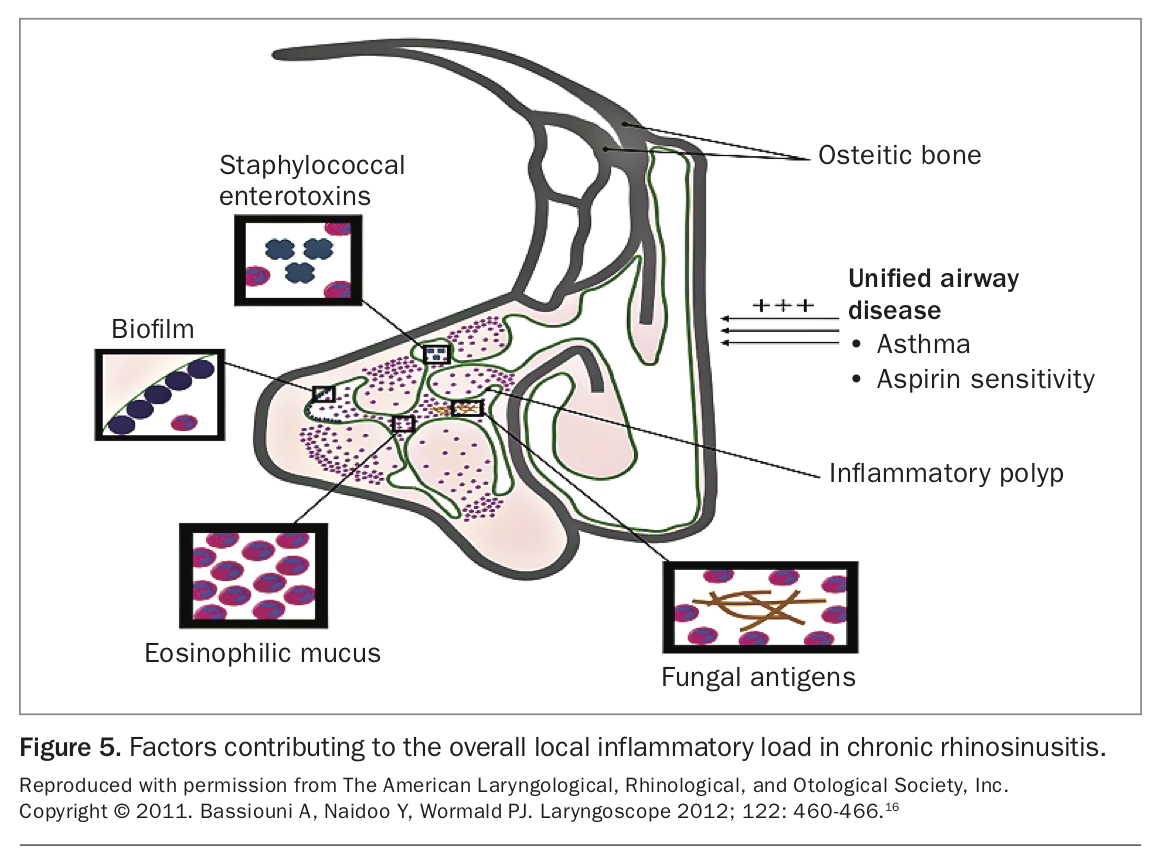
There are a number of factors affecting the ‘inflammatory load’ in the sinuses including biofilm formation, eosinophilic mucin and fungal antigens (Figure 5).18 Leaving inflammatory mediators behind by not addressing a sinus when it is diseased exposes the patient to persistent symptoms. Surgery not only allows for intraoperative removal of this inflammatory load, it also dramatically improves penetration of topical therapy to the sinuses. Topical therapy is key to the long-term reduction of sinonasal mucosal inflammation, improvement in mucociliary clearance and reduction in mucostasis.
{kind=link}
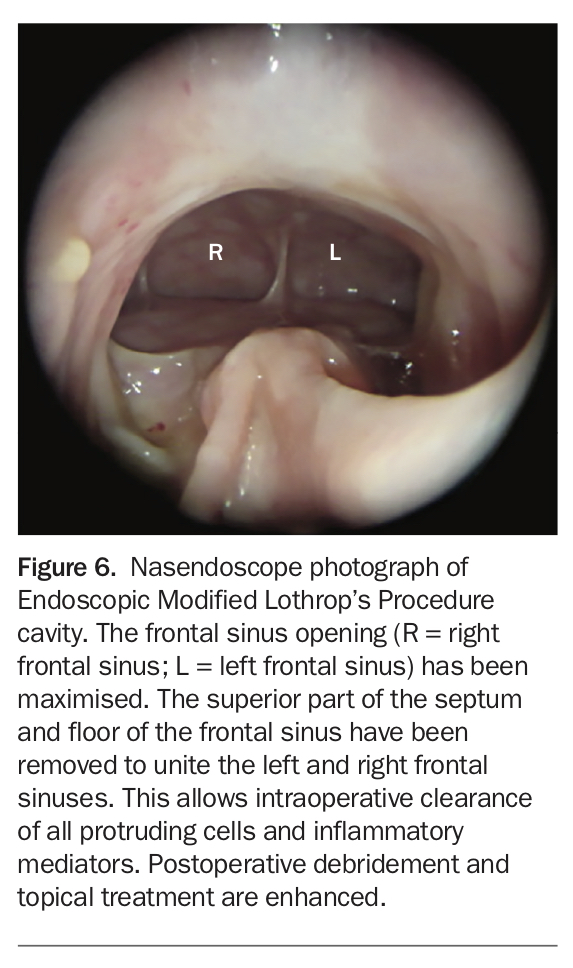
A number of new techniques have been devised to achieve total clearance of all inflammatory mediators. In particular, the Endoscopic Modified Lothrop’s Procedure (EMLP) has been increasingly used to treat the chronically diseased frontal sinus. The EMLP unites the left and right frontal sinus through a common opening by removing the floor of the frontal sinus and superior part of the nasal septum (Figure 6).19,20 Its success in treating recalcitrant disease is thought to be through facilitating complete removal of inflammatory mediators within the frontal sinus intraoperatively and allowing topical treatment postoperatively.
{kind=link}
New treatment modalities
Eosinophilic lower airways disease (i.e. eosinophilic asthma) often coexists in patients with CRS. Indeed, the chronic sinus disease they suffer from can be considered a form of ‘asthma of the nose’. Often, they struggle with both upper and lower airways inflammation, despite adequate surgery, long-term topical corticosteroid therapy and immunotherapy.
Dupilumab is a monoclonal antibody that inhibits signalling of interleukin (IL)-4 and IL-13, key drivers of type 2 inflammation, and has been approved for use in atopic dermatitis and asthma. In a recent randomised double-blind placebo-controlled trial, dupilumab was shown to reduce polyp size, sinus opacification and severity of symptoms, and was well tolerated.21 These results support the use of dupilumab for patients with severe CRS with polyps who might otherwise have few therapeutic options.
Conclusion
Rhinosinusitis is a common disorder with a significant impact on health and quality of life. The diagnosis is made using a combination of symptoms, signs and radiological findings. Medical treatment alone is often sufficient to resolve symptoms. Surgical treatment is reserved for cases that fail medical treatment or with acute complications. ESS has evolved dramatically over the past five years, with a focus now on extensive surgery to completely clear the disease burden and facilitate long term topical treatment. Immunotherapy and new monoclonal antibody therapeutic agents are increasingly being used for patients with recalcitrant disease. See box for information on rhinosinusitis and Covid-19. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.