Allergen immunotherapy for allergic respiratory disease

Patients have access to a wider range of effective immunotherapies for allergic rhinitis (hay fever) and allergic asthma that decrease the severity of symptoms with subsequent allergen exposure and lessen the need for medications – the closest thing to a ‘cure’ for allergy and an example of ‘personalised medicine’.
- Minimising exposure to allergic triggers and using medication to treat patients with allergic respiratory disease (allergic rhinitis and/or allergic asthma) may provide incomplete relief for allergy symptoms.
- Allergen immunotherapy aims to reduce or eliminate underlying allergic sensitivity.
- Emerging evidence shows aeroallergen immunotherapy may reduce the risk of new asthma development as well as improve existing asthma symptoms and need for medication.
- Immunotherapy options in Australia have expanded, with the availability of standardised allergen tablets for sublingual immunotherapy (SLIT) as well as traditional subcutaneous immunotherapy (SCIT).
- Assessment of benefit is largely subjective but objective scoring systems are available; repeat allergy testing is not used to assess benefit.
- To optimise selection of patients and allergens, allergen immunotherapy is usually prescribed and initiated by specialists with training in allergic disease; most injections can be administered by general practitioners and practice nurses who have had training.
- Barriers to accessing immunotherapy include knowledge of availability, access to specialist services, cost and convenience.
Allergic rhinitis is one of the most common chronic health conditions of teenagers and young adults and affects 15% of the Australian population overall.1 It has a significant personal impact, affecting sleep quality, emotional wellbeing and academic performance and causing up to a third of affected individuals to reduce allergen exposure by limiting outdoor activity.2,3 There is also a significant economic impact, contributing to ‘presenteeism’ and reduced productivity, with over-the-counter medication costs of $227 million in 2010.4
Allergic rhinitis usually lasts for many years, with one study describing that 45% of American college students were symptomatic 23 years after initial diagnosis.5 In another study of adults with respiratory allergy and a single sensitisation, 65% developed additional allergies over the next 10 years, and 32% of those who initially had only allergic rhinitis developed allergic asthma.6 In a study of remission incidence in participants with allergic rhinitis who were followed up after eight-years, only 17% underwent remission.7 Although 75% of school-aged children will outgrow asthma by adulthood, adults are less likely to experience asthma remission.8,9 Thus those hoping for spontaneous short-term resolution will often be disappointed.
Approaches for managing allergic respiratory disease
Options for patients with allergic rhinitis and/or allergic asthma are limited to the following approaches.
- Reduce exposure to allergic triggers (feasible for animal allergy; sometimes helpful for those with dust mite allergy; but avoidance of pollen and mould spores is not possible).
- Medication, which is usually effective and safe if used regularly but is not curative, and relapse occurs once withdrawn.
- Allergen immunotherapy, with the aim of altering the natural history of disease by altering and dampening the immune response so that fewer symptoms occur with allergen exposure.
There is conflicting evidence as to whether dust mite avoidance measures are effective, and high-efficiency particulate air (HEPA) filters to remove pet allergen have doubtful clinical benefit.10-14 Even if a pet is removed from the house, animal dander is very stable and can take many months to degrade. Furthermore, allergen exposure may occur outside the home, such as in schools or childcare centres, even where pets are absent. Removing indoor mould and pot plants may assist someone who is allergic to mould, but mould spores are present in the air independent of such measures. Seasonal triggers such as grass, weed and tree pollen are windblown and not easily avoided; drying bedding in springtime and removal of causative trees near the house might have some modest benefit. Furthermore, many people are allergic to multiple triggers.
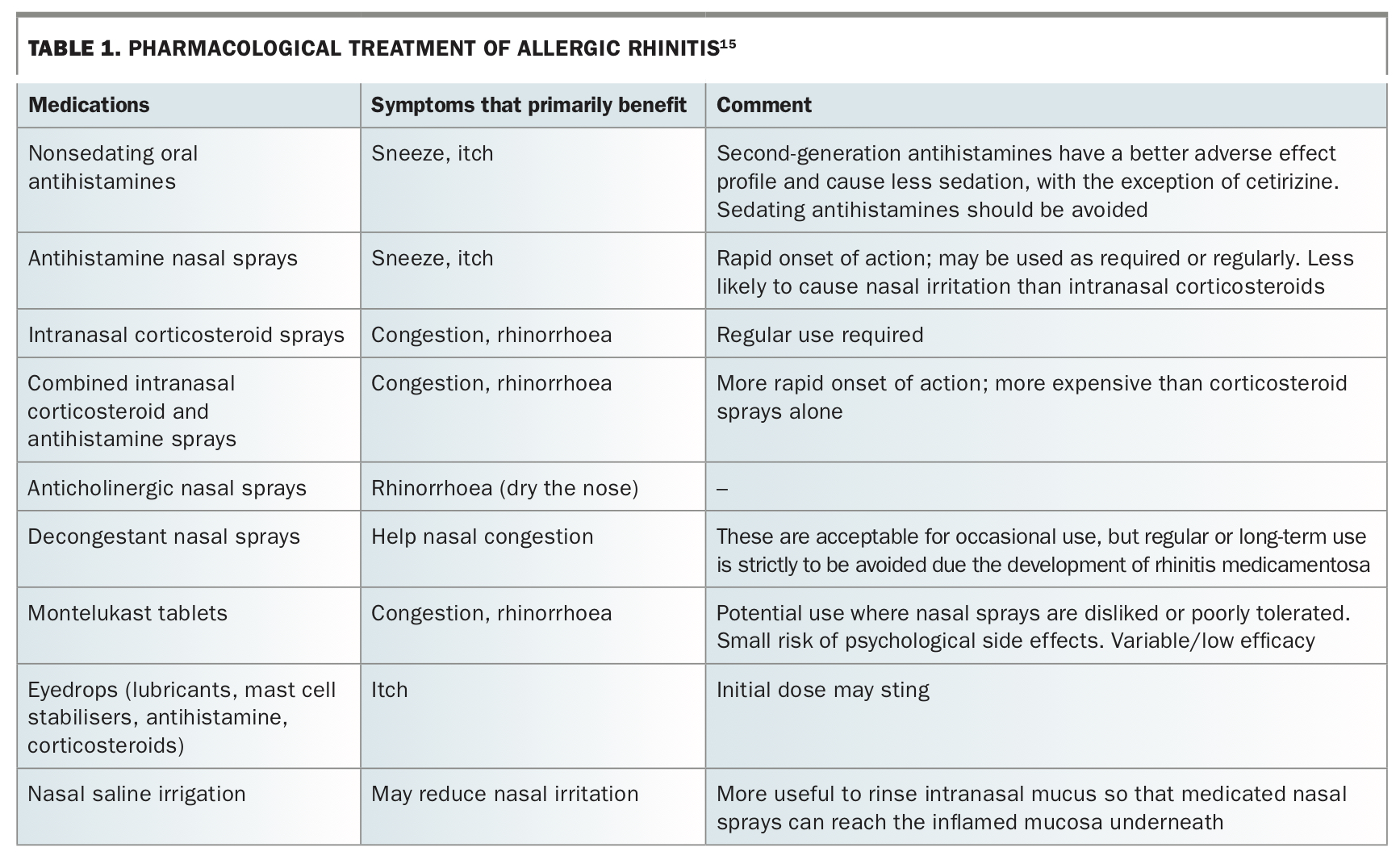
Pharmacological options for the treatment of allergic rhinitis are summarised in Table 1.15 Although effective treatments are available, not all achieve adequate control and relapse occurs when withdrawn. Allergy medicines are very safe with prolonged use in the vast majority and significant side-effects are rare.
{kind=link}
Allergen immunotherapy
Allergen immunotherapy involves the regular administration of a commercially prepared extract of a substance that a person is allergic to (allergen), with the aim of altering the immune response to allergen exposure. Effective immunotherapy for allergic rhinitis (hay fever) and allergic asthma decreases the severity of symptoms with subsequent allergen exposure and lessens the need for medications. It is the closest treatment to a ‘cure’ for allergy and an example of ‘personalised medicine’.
Allergen immunotherapy may be indicated in the management of patients with:
- allergic rhinitis with or without allergic conjunctivitis
- allergic asthma.
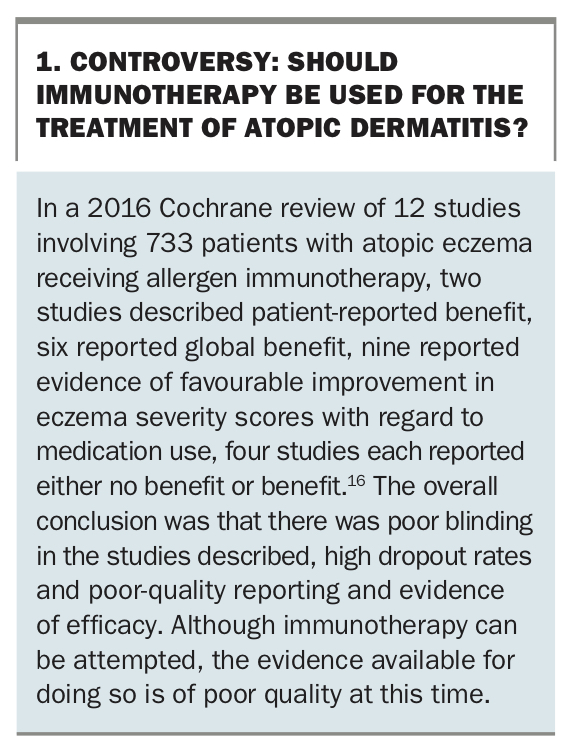
Immunotherapy is also effective in the management of stinging insect anaphylaxis. It is not currently recommended for the treatment of atopic eczema due to lack of convincing evidence of benefit (Box 116), although a trial of immunotherapy (usually to house dust mite) may be offered in some very motivated patients. Immunotherapy is not currently recommended in Australia or New Zealand for the treatment of food allergy outside of research centres, due to high rates and unpredictability of adverse reactions including anaphylaxis.16,17 There is no proven benefit for immunotherapy in the management of oral allergy syndrome and no evidence that it alters the natural history of nasal polyposis.18
{kind=link}
When to consider allergen immunotherapy
Use of allergen immunotherapy may be considered in patients for whom:
- allergic triggers are difficult to avoid (e.g. grass pollen)
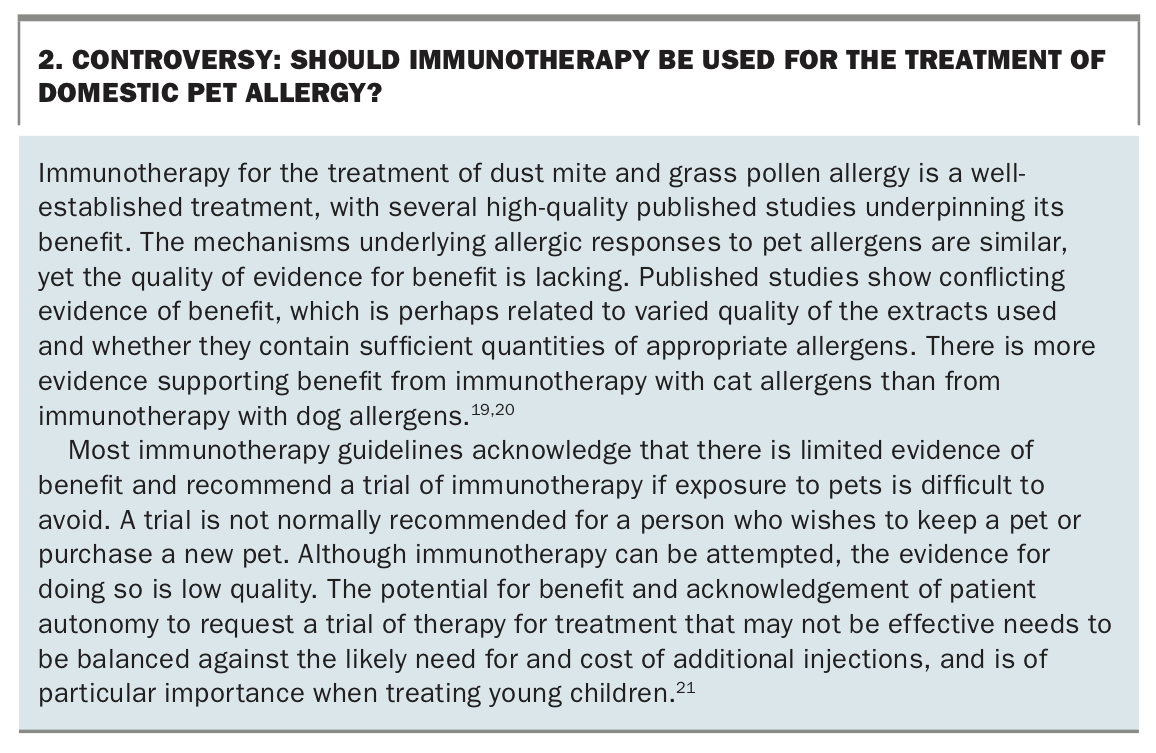
- avoidance of allergic triggers is not possible or desirable (e.g. occupational exposure to animals, or the person is resistant to rehousing a pet [Box 219-21])
- medication is ineffective, poorly tolerated, is disliked or is not taken regularly enough to be effective.
{kind=link}
Other issues when considering allergen immunotherapy include:
- patient treatment preference (taking the above factors into consideration)
- patient ability to commit to and adhere to a long-term treatment program
- potential cost-effectiveness compared with ongoing medication for many years18
- potential to help mitigate the severity of allergy-induced asthmatic symptoms, particularly in those allergic to ryegrass who are therefore prone to thunderstorm asthma
- it may alter the natural history of atopic disease (e.g. by reducing the risk of asthma development in children presenting with allergic rhinitis)22,23
- there is high-quality evidence that dust mite and grass pollen immunotherapy is effective, but lesser quality evidence that pet or mould allergen immunotherapy is effective.
Mechanism of allergen immunotherapy
The basis of allergen immunotherapy is that regular exposure to the allergen results in an early reduction in the inflammatory response to allergen exposure, development of immunoglobulin (Ig) G4 ‘blocking’ antibodies that inhibit the binding of allergen to IgE, and a long-term reduction in allergen-specific IgE.24
Benefits of immunotherapy for allergic rhinoconjunctivitis
Several controlled studies have shown improvement in symptoms of allergic rhinitis and conjunctivitis and a reduction in the need for allergy-related medication.25 Similar changes have been observed in the treatment of asthma, although without significant changes in objective measures of lung function.26,27 Treatment duration of three to five years is recommended, and studies of sublingual/oral immunotherapy (SLIT) and subcutaneous immunotherapy (SCIT) have shown sustained benefit after treatment cessation for at least three years.
Immunotherapy and thunderstorm asthma
During the thunderstorm asthma event of 2016 in Melbourne, there were over 3500 acute asthma presentations, 10 deaths and an overwhelmed health service in the context of over 100 pollen grains per cubic metre of air, rising humidity, a drop in air temperature and gusty winds. A nonrandomised observational study showed a lower risk of asthma symptoms during that event among those taking oral grass pollen immunotherapy tablets. In this group, 29% needed reliever medication only, compared with 35% needing reliever medication only and 41% suffering an acute asthma exacerbation in the group taking only pharmacotherapy.28
Immunotherapy and new asthma development
Emerging evidence shows immunotherapy for aeroallergens may reduce the risk of asthma development as well as improve existing asthma. The GAP study enrolled 812 children with grass allergy aged between 5 and 12 years of age and allocated them to either standard oral grass tablet immunotherapy or placebo. Seventy-five percent completed the study, and follow up was two years after study completion. Substantial benefit was observed for those in the immunotherapy arm in terms of hay fever severity and a reduction in the proportion of new asthma development from 20% on placebo tablets to 15% in those on active treatment (odds ratio 0.66).22 A dust mite immunotherapy trial in 111 high-risk babies aged five months allocated participants to dust mite tablets or placebo for 12 months. When assessed at the age of six years, those in the intervention arm had a reduction in dust mite sensitisation from 45% to 28%, with a reduction in definite asthma from 13.5% to 2.9%.23 These results are consistent with several ‘real-world’ European studies examining the use of new asthma-related medication in patients receiving immunotherapy for treatment of allergic rhinitis.29
More treatment options are now available for respiratory allergy
Two types of injectable aeroallergen immunotherapy products containing native allergens have been available in Australia for some time. They are aqueous formulations and aluminium hydroxide conjugated products that are administered by subcutaneous injection (subcutaneous immunotherapy [SCIT]), slowly increasing the dose over two to three months until a maintenance dose is achieved. This is followed by a maintenance phase over three to five years to achieve a sustained benefit even after treatment is ceased.
More recently, polymerised allergen (allergoid) injections have become available in Australia and New Zealand. They are considered to have fewer side-effects than other SCIT products due to lower IgE binding. Although comparative studies with other injectable extracts are not available, similar clinical benefit and changes in allergen-specific IgG4 and IgE levels have been observed in placebo-controlled double-blind studies using allergoids.30 Because they have a greater safety margin, up-dosing to the maintenance dose with allergoid is generally done over a shorter time – a matter of weeks rather than months. All the currently available injectable aeroallergen extracts are registered for use on a ‘named patient’ basis, although selected TGA-registered SCIT products may return to the local market in the next 12 months.
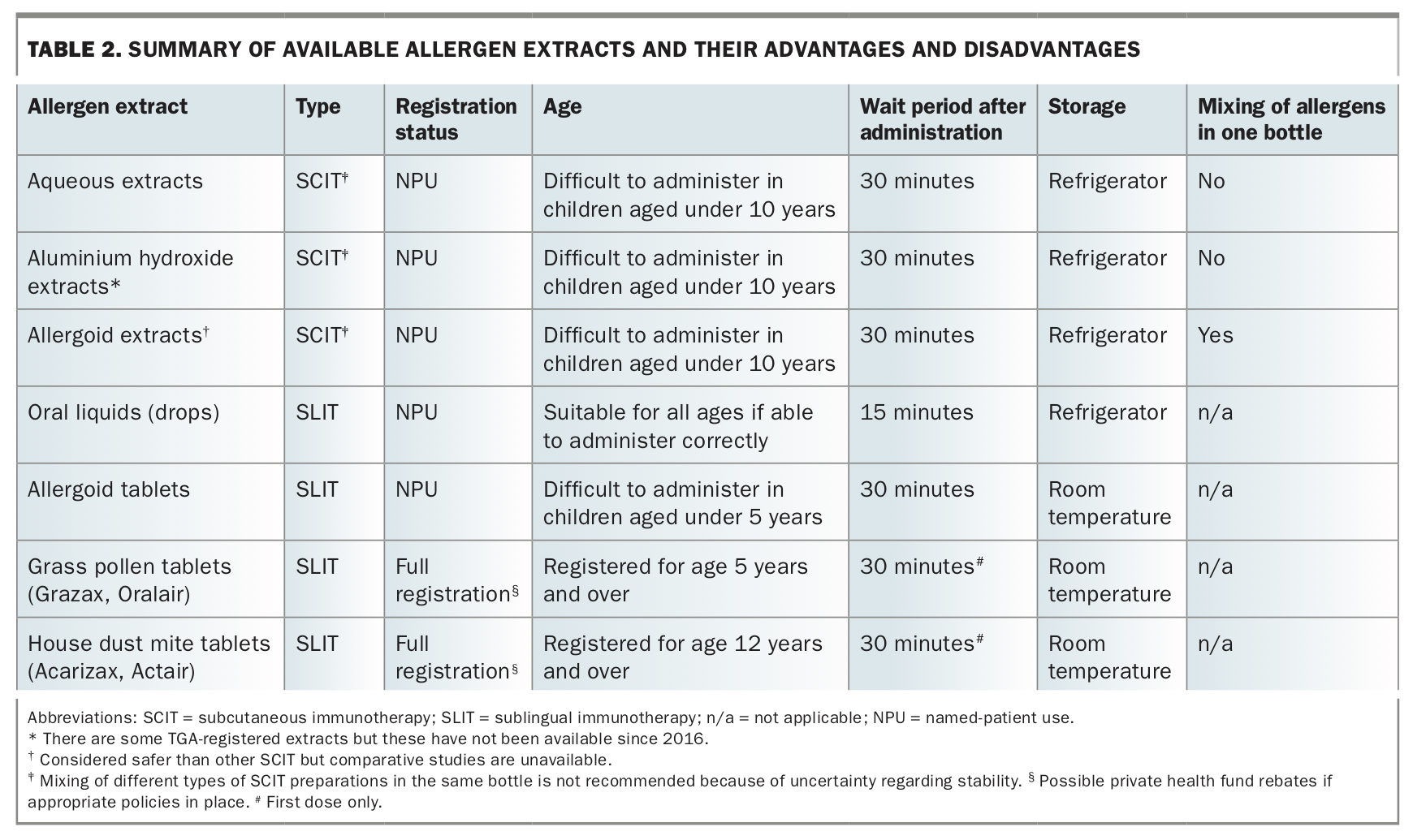
SLIT has had a long tradition of use in Europe and has been available in Australia and New Zealand for over a decade. Available products include sublingual drops and sublingual allergoid tablets (named-patient basis) as well as fully TGA-registered standardised sublingual dust mite and grass pollen tablets. The available allergen extracts and their advantages and disadvantages are summarised in Table 2. It is possible to undertake immunotherapy directed at more than one target at the same time;31 however, mixing nonallergoid SCIT extracts in the same bottle is discouraged because of the risk of enzyme degradation and the potential for dilution to reduce effectiveness.
{kind=link}
No aeroallergen immunotherapy extract is subsidised under the PBS, although private rebates may be available for TGA-registered products. There is a Medicare subsidy for medical consultations associated with both SCIT and SLIT. (Venom immunotherapy treatments are subsidised through the PBS.)
Who should prescribe allergen immunotherapy?
Allergen immunotherapy is usually prescribed and initiated by paediatricians and physicians with training in clinical immunology and allergy. This optimises selection of patients and allergens and enhances the likelihood of benefit.18 Most injections can be administered by GPs and practice nurses who have had training. Free e-training on allergen immunotherapy and management of anaphylaxis (which is a risk with SCIT and, in rare cases, initiating SLIT) is provided by the Australasian Society of Clinical Immunology and Allergy (ASCIA).32
Contraindications and precautions
Pregnancy
If a patient is pregnant or planning pregnancy in the near future, commencement of SCIT is best deferred, owing to the risk of systemic allergic reaction that may affect a developing fetus. SLIT has a larger margin of safety and could be commenced if a patient is not yet pregnant, as the maintenance dose is reached within days and significant adverse reactions usually occur within days or weeks of treatment commencement. There is no evidence that immunotherapy causes fetal malformations, so if a patient is stable on SCIT or SLIT there is no need to stop therapy.
Underlying disease
Poorly controlled asthma, advanced age and cardiovascular disease may all have an impact on the safety of allergen immunotherapy and should be considered before initiating treatment. Although autoimmune disease, malignancy and immune deficiency are often mentioned as relative contraindications to allergen immunotherapy in product information sheets, there is no convincing evidence that affected individuals are at increased risk of an adverse reaction. Patients with arm lymphoedema (e.g. after cancer surgery) should have injections on the nonaffected side.
SLIT may be considered in those who have had anaphylaxis to SCIT; however, it must be initiated with caution, as anaphylaxis to SLIT, although extremely rare, has occurred in people with previous anaphylaxis to SCIT. Eosinophilic oesophagitis is a contraindication to SLIT; SCIT is the only option for patients with this condition. Beta blocker use, especially nonselective beta blockers, may impede the management of anaphylaxis with adrenaline, so beta blockers should be avoided if allergen immunotherapy is prescribed.
Practical and safety aspects of SCIT
SCIT is administered as deep subcutaneous injections, halfway between the shoulder and elbow over the deltoid region. Ideally, a 26/27 gauge diabetic needle and syringe should be used without dead space. Local itching and swelling are common and can be reduced by antihistamines taken before each injection. Vigorous exercise within two to three hours of an injection is discouraged because delayed systemic reactions may be triggered by physical exertion. Doses are best deferred if the patient has a fever or infectious illness or unstable asthma at the time. Influenza-like symptoms after injection are rare but may prompt cessation in some cases. A 30-minute wait period, under observation in the clinic waiting room, is recommended in case a more serious reaction occurs such as delayed asthma, rash or anaphylaxis. For this reason, medical staff with the skills and equipment to treat anaphylaxis must be available at any facility in which immunotherapy injections are administered. It is usually difficult to undertake SCIT in young children, although application of a local anaesthetic patch one hour before treatment may improve tolerance.
Practical and safety aspects of SLIT
SLIT tablets or drops are administered under the tongue, retained for two minutes, then swallowed. Patients are advised to not eat or drink for 10 minutes afterwards. Studies have shown that if this practice is followed, the allergen remains in the mouth for a couple of hours, interacting with immune cells, including dendritic cells, locally.
Most side effects are local, manifesting as brief transient local itch and swelling which usually subside after the first couple of weeks of treatment. Tablets appear to be more potent than drops in causing such side effects. A 30-minute wait period in the doctor’s surgery is recommended after the initial dose in case tongue or throat swelling occurs. Antihistamines taken on a regular basis for the first couple of weeks usually improve tolerance. If less common side effects such as stomach pain, indigestion, severe tongue or throat swelling or eosinophilic oesophagitis occur, then treatment should be ceased. Allergoid tablets prescribed on a named-patient basis are less likely to trigger local side effects but evidence for their efficacy is limited. Until there are more safety data, these products should also be avoided in individuals with eosinophilic oesophagitis.33
The major advantages of oral treatment are the ability to start immunotherapy in young children, room temperature storage of some preparations (tablets) and convenience. The major downside is cost. The dose of oral allergen needed to alter an immune response is much greater than that required for subcutaneous therapy, so the cost of SLIT is usually higher than the cost of SCIT, especially if allergen immunotherapy directed against multiple targets simultaneously is undertaken.
Assessment of benefit
Assessment of benefit is largely subjective, based on patient perception of reduced frequency and severity of symptoms and reduced need for medication on exposure to allergic triggers. Various scoring systems such as the Sino-Nasal Outcome Test (SNOT) and the Control of Allergic Rhinitis and Asthma Test (CARAT) are available to provide some objectivity in assessing benefit.34,35 Repeat allergy testing does not have a role in assessment of benefit from immunotherapy since even successful immunotherapy, with substantial symptom relief, usually leaves skin prick tests still positive.
Generally, review may occur in the first six to 12 months of treatment and, if shown to be effective, treatment may be continued for a total of at least three years. If treatment is ineffective, options that can be considered include ongoing medication, ongoing allergen immunotherapy (which usually improves in effectiveness with further time in SCIT and SLIT studies), or a change in method of administration (e.g. SLIT to SCIT or vice versa, although there are no published studies using this approach).
Which is better: SCIT or SLIT?
There are few studies directly comparing tablets and injections in the same trial and these are too small (about 20 to 30 subjects) to show any meaningful difference.25 Compared with older and sometimes much smaller placebo-controlled studies of SCIT that showed benefit, the evidence base for SLIT, especially for tablets, is more recent and of much higher quality. Anecdotally, some patients appear to do better on one method than another and tablet SLIT appears to be much more effective than use of the older sublingual drops, probably because of better allergen standardisation and much higher doses administered.
Access to allergen immunotherapy
There are several barriers to accessing allergen immunotherapy for allergic respiratory disease in Australia and New Zealand, including knowledge of availability, access to specialist services, time off work (if undertaking SCIT) and the financial cost of aeroallergen extracts.
There is no local manufacture of injectable allergen immunotherapy extracts. Extracts are used under named-patient basis and are imported and generally take a couple of months to arrive from overseas. The implication is that careful planning is needed to prevent interruptions to treatment. By contrast, fully registered oral tablet immunotherapy may be purchased at the local pharmacy on prescription, making access much easier.
When to refer for immunotherapy
The primary reasons to refer patients for allergy assessment are:
- they have symptoms that are difficult to control and the cause is difficult to avoid;
- they require multiple regular medications to control allergic respiratory disease;
- they have complex multisystem allergic disease.
Nonetheless, even patients with mild symptoms should be made aware of the therapeutic options available beyond medication, so that if symptoms worsen, the option of immunotherapy can be explored.
Conclusion
Decision-making about immunotherapy for allergic respiratory disease first involves deciding whether to proceed to immunotherapy or continue avoidance strategies and medication management. The next decision is which allergens to target. Allergy testing conducted by a clinical immunology/allergy specialist is recommended to ensure allergen immunotherapy is not undertaken unnecessarily. The method of treatment is then decided as this will determine cost as well as other factors such as risk, convenience and adherence. MT
References
2007_economic_impact_allergies_report_13nov.pdf (accessed September 2021).
ASCIA_PCC_Allergen_minimisation_2019.pdf (accessed September 2021).
ASCIA_AIT_Guide_2019.pdf (accessed September 2021).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.