Long-term opioid use: assessment of mental health issues
Long-term opioid use is strongly associated with mood disorders, post-traumatic stress disorder, personality disorders and both attempted suicide and suicide. More than half of people who use illicit opioids fit the criteria for a psychiatric diagnosis. Another emerging issue of concern is the high rate of psychiatric comorbidity among individuals who develop dependence on pharmaceutical opioids, often in the context of chronic pain. Sensitive questioning by the GP about psychological distress and suicidal behaviours may enable better management of these often-overlooked issues.
Opioids are commonly used drugs both legally and illicitly, with illicit use accounting for just over half of all opioid use.1 Opioids have the highest dependence liability of all illicit drugs, with an estimated one in four users of heroin developing dependence. Other members of the opioid class include morphine, codeine, methadone, oxycodone and fentanyl. In recent years, the use and abuse of pharmaceutical opioids has become a major public health concern, particularly in North America but increasingly too in Europe and Australia.1
Trajectories into long-term opioid use may be considered to fall into two broad categories: first, illicit use, predominantly of heroin, in individuals typically aged in their 20s and 30s; and second, an older cohort who use pharmaceutical opioids to manage chronic pain.1 Mental health problems are common issues faced by both groups. Indeed, despite key differences in how individuals from these groups may present, the nature of the mental harms faced are surprisingly similar and both groups present significant challenges. GPs may be more likely to come into contact with the latter group, for whom chronic pain care is largely based in the community, whereas people who use illicit drugs are less likely to seek help on a regular and reliable basis.2
Risk factors for psychiatric disorders
Several factors in early childhood increase the risk for long-term illicit use of opioids, specifically heroin. These include social disadvantage, early onset of both psychological problems and antisocial behaviours, and exposure to childhood abuse or neglect.1 Parental factors such as drug dependence, psychopathology and separation or absence during childhood also contribute to risk.1 Exposure to these early-life risk factors also significantly increases risk for psychiatric disorders, accounting to some degree for the very high rates of mental health problems in people who use illicit drugs.
Illicit drug use, which often entails polysubstance use, may exacerbate existing pathology or engender high levels of distress due to the pharmacological effects. Factors such as social isolation, impoverished lifestyle and exposure to situations that are psychologically distressing, for example, witnessing an overdose or being subject to sexual or physical attack, are associated with ongoing illicit substance use. Among individuals taking opioids for chronic pain, the importance of these early-life exposures is not yet fully understood. Importantly though, chronic pain is associated with childhood abuse and neglect.3
Assessing past trauma is therefore important as it is a common risk factor affecting the onset and course of substance use, chronic pain and mental health difficulties. The subject of trauma should be broached sensitively in a safe clinical environment where there is trust that information provided will be responded to appropriately. Trauma-informed care as an approach to management focuses less on diagnosis and more on the recognition of trauma, the provision of safe treatment settings and the mobilisation of individual strengths.4
Mood and anxiety disorders
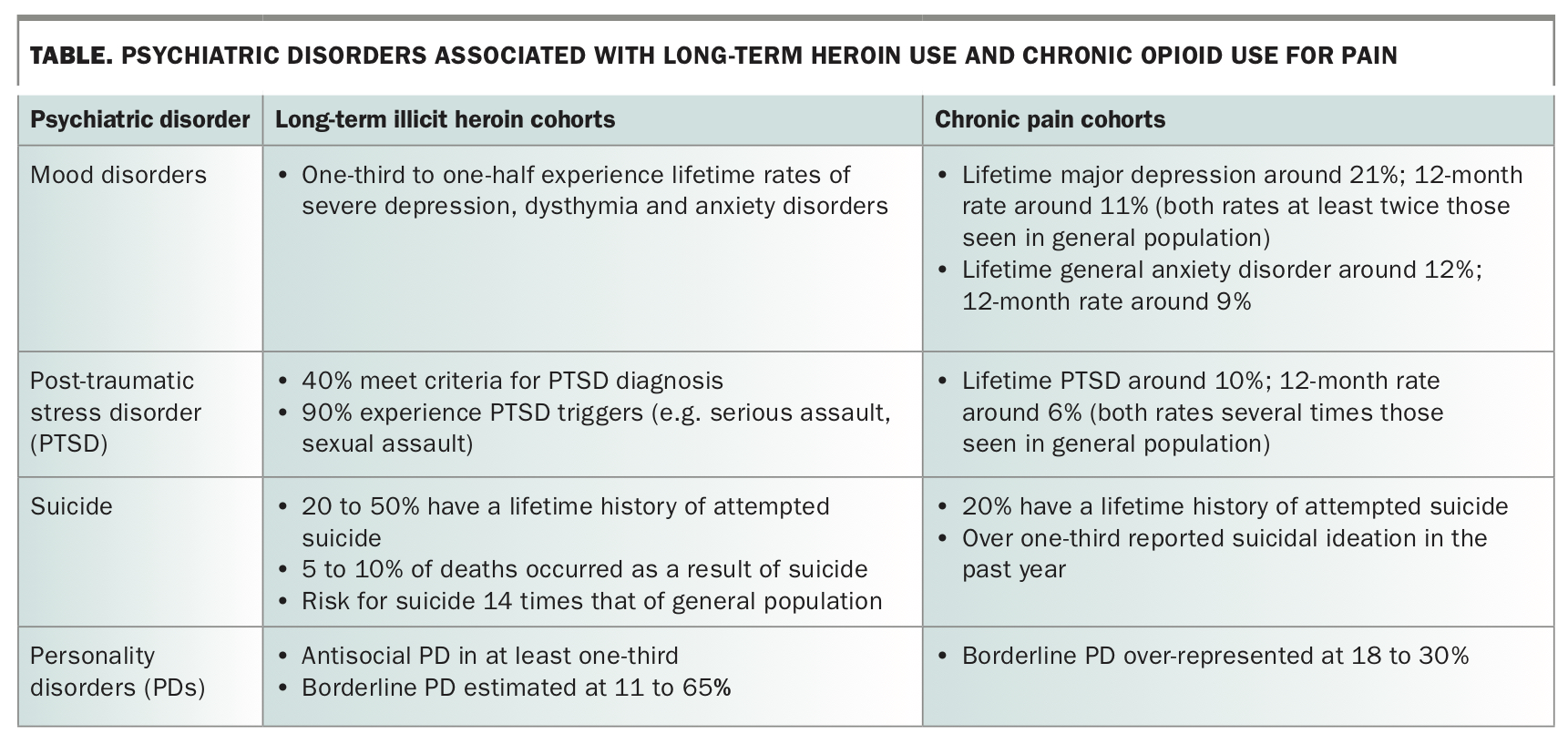
Mood disorders are common in people who use illicit drugs, with lifetime rates of severe depression in the order of one-third to one-half of long-term heroin users (Table).1,5 It has been suggested that the experience of severe depression may motivate users, particularly women, to seek treatment for their opioid use.6 This may prove an important opening for the GP to discuss management of long-term opioid use.
{kind=link}
Post-traumatic stress disorder (PTSD) is the most common anxiety disorder among people who use illicit drugs and is characterised by re-experiencing of traumatic event(s), elevated arousal (muscle tension, disturbed sleep, elevated startle response), avoidance of situations or conversations that serve as reminders of trauma, and negative mood and thought content. In some individuals, these features may be seen in combination with emotional dysregulation and poor interpersonal function.
Reflecting widespread exposure to sexual abuse and violence, a history of exposure to potential PTSD triggers (e.g. serious assault, sexual assault) is present in about 90% of illicit opioid users; more than 40% of these individuals meet criteria for a PTSD diagnosis and a third to half have experienced childhood sexual and/or severe childhood physical abuse.1,5 Half or more of people who use illicit opioid drugs report emotional abuse and physical neglect.1 Lifetime rates of anxiety, depression and PTSD are also high in community-based samples of people taking opioids for chronic pain, and suicidality is two to three times more common than among the general population.7,8
Eliciting signs and symptoms of depression, anxiety and PTSD and acknowledging the burden of these experiences are important first steps in managing people who use illicit opioids. The GP can then start a dialogue with the individual about mental health symptoms by helping them recognise common feelings of sadness, guilt, shame and anger. Explaining how these symptoms impact negatively on overall wellbeing and function may enable individuals to consider trialling an antidepressant or being referred to a psychiatrist or other mental health professional. Such discussions may need to be initiated by the GP opportunistically, as individuals may present with issues related to physical rather than mental health.
Suicide and suicidality
Suicide and suicidality are major clinical concerns among people who use both illicit and pharmaceutical opioids (Table). The general population lifetime prevalence of attempted suicide is less than 5%, whereas estimates for people who use heroin range between 20 and 50%.9,10 The risk of completed suicide is about 14 times that of the general population. Indeed, 5 to 10% of deaths among people who use heroin are the result of suicide.11 Rates of suicidal thoughts and attempts in people prescribed pharmaceutical opioids in the community for chronic pain are also extremely high: over one-third reported suicidal ideation in the past year and one in five made a lifetime suicide attempt.7
Among community-based individuals taking opioids for chronic pain, risk for experiencing suicidal ideation in the past 12-months is associated with higher pain scores and lower pain self-efficacy.7 Lifetime suicidal ideation after the onset of chronic pain is more likely among those who have a depression diagnosis, who screen positive for borderline personality disorder and who report abuse in childhood.7 Deliberate self-harm behaviours such as self-mutilation are also common among people who use illicit opioids, although evidence suggests that the increased prevalence is associated with features common to drug dependence in general, such as high rates of screening for borderline personality disorder, previous suicide attempts and childhood sexual maltreatment, rather than with opioid dependence specifically.12
There can be reluctance among health professionals to enquire about suicidal risk in case this might significantly increase suicidal thoughts. There is no evidence that this is the case, either in general or at-risk populations.13 Rather, if the GP can broach discussion of these highly-stigmatised thoughts and behaviours, the patient comes to understand that they are not alone in having these feelings and that help is available. Important factors to include in assessment of suicide risk are prior attempts and access to means (tablets for overdose, firearm) as each strongly predicts both subsequent attempts and completion. This also highlights the need for caution in prescribing high-lethality drugs commonly used in overdose, such as benzodiazepines, barbiturates and tricyclic antidepressants.
Personality disorders
Personality disorders (PDs) may also be observed, most commonly antisocial or borderline types, among long-term users of illicit opioids. Antisocial PD is seen in around one-third of people who use heroin;10 however, the diagnosis is based on antisocial behaviours, for example performing illegal acts. In reality, it is difficult to distinguish between the presence of PD and behaviours generated by illicit drug dependence.
Borderline PD is characterised by intense and frequent affective dysregulation, marked impulsivity, chronic feelings of emptiness and disturbances of identity and interpersonal function.1 The prevalence of borderline PD among people who use illicit opioids ranges from 11 to 65%, which is higher than that of the general population (around 2%) (Table).1,10 Borderline PD rates are also notably higher among individuals taking opioids for chronic pain, with recent estimates ranging from 19 to 30%.14,15 Among this group, daily benzodiazepine use and dependence on opioids are common, supporting the suggestion that individuals with borderline PD may over-use opioid medication in attempts to manage their chronic pain.14 Individuals with borderline PD frequently use health services and thus may present regularly to their GP. These issues, together with the increased rates of both suicidal thoughts and lifetime suicide attempts among people with borderline PD can make engaging in constructive therapeutic planning challenging. It is important that there is clear and effective communication between all health professionals involved in care planning and that, when possible, there is access to a psychiatric expert.
Treatment
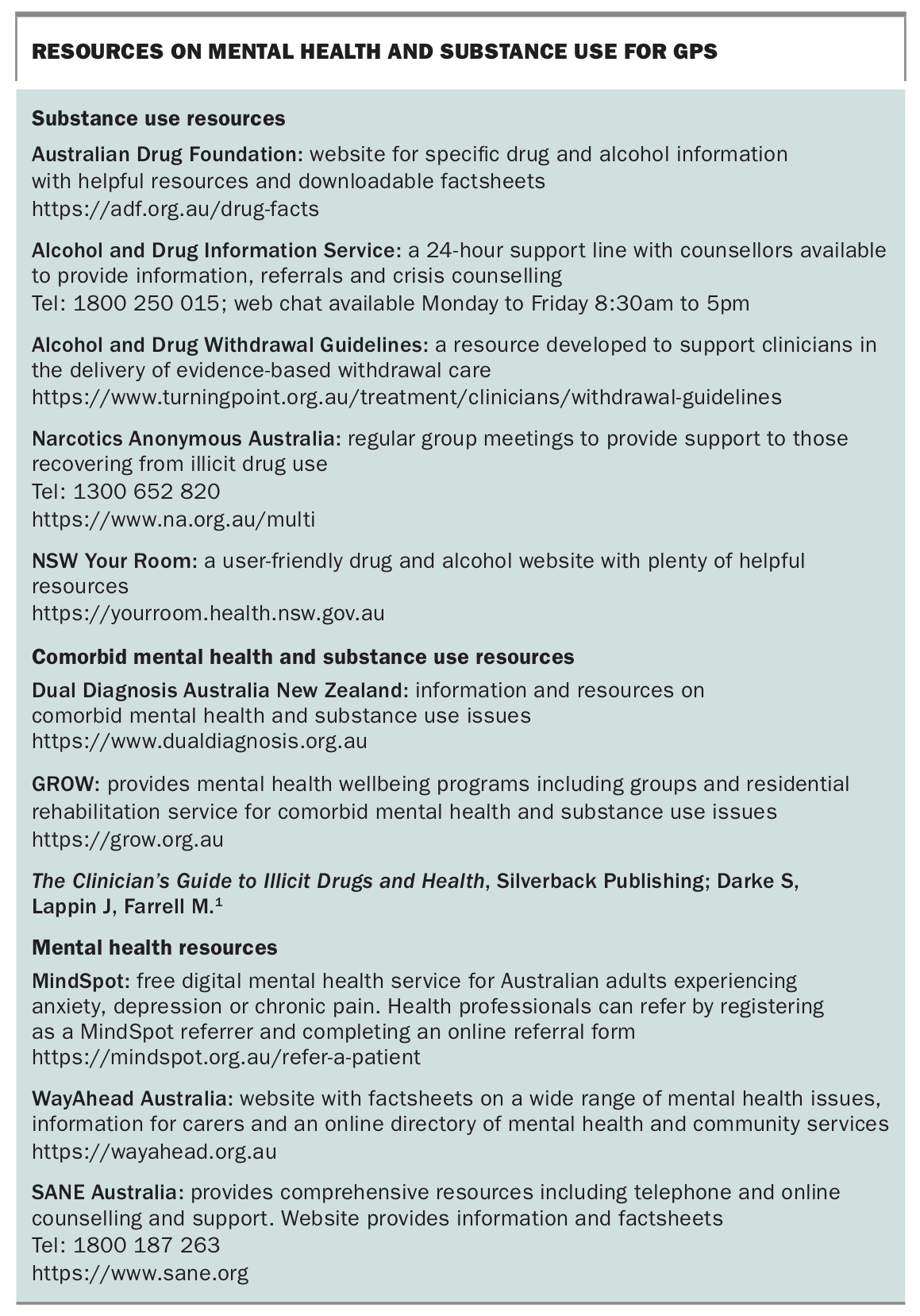
Treatment for long-term opioid use is an important consideration for patient management that should be encouraged by GPs. Often an individual may be unwilling to accept the suggestion that they are dependent on opioids. Those who are willing to accept treatment may find it difficult to access services because of the high demand for opioid detoxification to manage withdrawal and subsequent maintenance treatment.1 The mainstays of treatment for maintenance are residential rehabilitation and opioid substitution (available as an outpatient) using the opioid agonists methadone and buprenorphine. Narcotics Anonymous attendance after stopping treatment can improve abstinence rates, particularly if attended at least weekly.1 Finally, it is to be expected that individuals will cycle through periods of relapse and abstinence. This can be disheartening for the patient and their support networks including the GP, and mechanisms of support should be made available to those caring for such individuals when needed. A list of resources for GPs and their patients can be found in the Box.
{kind=link}
Conclusion
The issues surrounding long-term opioid use and mental health are complex. Although long-term opioid use and the reasons underlying it are difficult to treat, significant improvements in wellbeing and quality of life may be achieved through addressing psychological distress. The important relationship between the GP and patient provides opportunity to sensitively develop a discourse around mental health issues and to acknowledge the patient’s burden. MT