Self-harm. Intervening early can save a life

Mental health
Adolescent mental health
Non-lethal self-harming is a common problem in young people in Australia and an important risk factor for subsequent suicide. Effective intervention represents one of the best opportunities for suicide prevention worldwide. The GP, with their knowledge of the family and personal background of the patient, is in an ideal position to intervene early.
Self-harm is an important public health problem, and a powerful risk factor for suicide. Self-harm – also referred to as self-injury – is defined as the direct, intentional injuring of body tissue that is done without suicidal intentions.1 It refers to a range of behaviours and does not itself constitute a mental disorder or illness. The most common methods of self-harm among young people are cutting and deliberately overdosing. Other methods include burning (with cigarettes), hitting or scratching body parts, hanging, binge eating or starvation, or deliberate and repeated exposure to dangerous situations.
People self-harm for many reasons, including cognitive impairment (dementia), severe depression, obsessive-compulsive disorder, alcohol and drug use and cultural identification (such as female genital mutilation).2 There are also the much rarer forms of self-harm and bodily mutilation caused by psychotic delusions or auditory hallucinations commanding self-harm. This article will focus on the repetitive self-harming particularly seen in young people with chronic dysthymia and/or a personality disorder usually due to childhood trauma (emotional, physical, sexual abuse or neglect).
Characteristics of self-harm
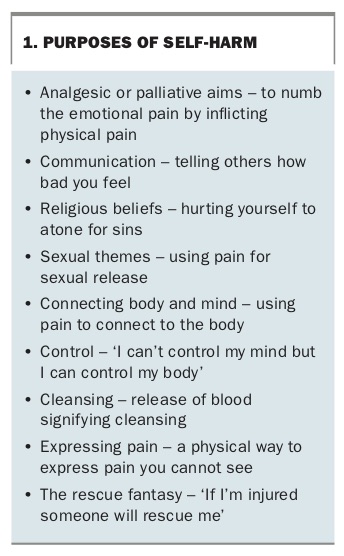
Self-harming is often not intended to be fatal but it is a coping mechanism – to alleviate intense emotional pain or overwhelming negative thoughts or memories (Box 1).3 In some cases it is intended as self-punishment, to replace emotional pain with physical pain, to show others how bad they feel or to see blood to confirm they are actually alive (as they ‘feel dead inside’). It can become a compulsive and dangerous activity.4,5
{kind=link}
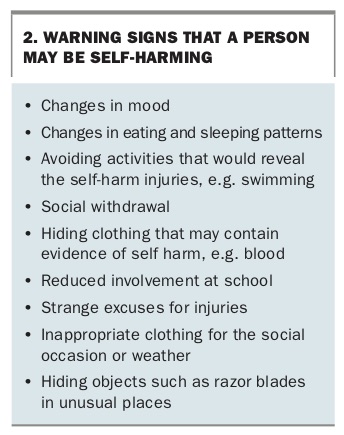
Characteristics of self-harmers include impulse dyscontrol, unstable relationships, fear of change, poor self-care, low self-esteem and rigidity of thinking. Many young people try to conceal their self-harming behaviour by injuring parts of the body usually hidden by clothing, such as their thighs and upper arms. Only 50% seek help and then often not through professional sources. (See Box 2 for signs that indicate a person may be self-harming.)
{kind=link}
The number of young people who die by suicide in Australia each year is low compared with the number who self-harm. Australian Bureau of Statistics data from 2016 show there were 814 (0.3%) male suicides and 324 (0.1%) female suicides in the 18 to 24 year age group (320,000 people),6 whereas the lifetime prevalence rate of self-harm in Australia is 17% for females aged 15 to 24 years and 12% for males of the same age.3 The incidence of hospital-treated self-harm is 117 people per 100,000 population a year, which is likely an underestimate, because it does not account for non-treated or community-treated episodes of self-harm.7
Suicide and self-harm account for much of the burden of disability and mortality among young people. The most common methods of self-harm are self-poisoning and cutting. There are rarer forms of self-harm such as severe self-mutilation, which differ from other forms of self-harm in that there is often delusional ideation. There may be loss of bodily function and psychosis is usually present. Examples include amputations (limbs, penis) and self-immolation.8,9
Risk factors for self-harm include:
- sociodemographic factors – being female, having a low socioeconomic status, being lesbian, gay, bisexual, transgender or intersex
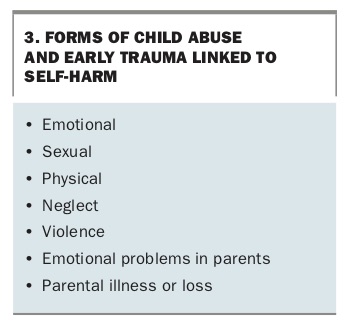
- life events – parental separation, history of abuse, family history of mental disorder and bullying (Box 3)
- psychiatric factors – depression, anxiety, attention deficit hyperactivity disorder, drug use, low self-esteem, perfectionism, hopelessness and personality disorder.
{kind=link}
More than 80% of people who self-harm have a psychiatric illness, of which depression, anxiety and alcohol misuse are the most common.10 Attention deficit hyperactivity disorder and conduct disorder are common among adolescents who present with self-harm.
Older adults who self-harm often have a higher level of lethal intent and less impulsivity, and there are higher rates of self-harm in Aboriginal and Torres Strait Islander people.6
Self-harm is a powerful risk factor for subsequent suicide, with the risk of suicide being many times greater than that in the general population.11 About 30 to 40% of people who die from suicide have harmed themselves in the previous year.7,11 The more lethal the method of self-harm, the more likely a subsequent suicide, e.g. ingestion of pesticides, hanging and gassing.
Assessment and management
Effective intervention for self-harm probably represents one of the best opportunities for suicide prevention worldwide. Psychosocial assessment – encompassing social and family circumstances, relationships, mental health, drug use, suicidal ideation, access to means to suicide, coping mechanisms and strengths – decreases the risk of repeat self-harm especially if there is no formal psychiatric history.12 It is also important to find out if there is a previous history of self-harm as there is a 55% increased risk of repetition.12,13
The GP’s relationship with the person is the single most important factor in managing self-harm. It should be empathic and understanding and should encourage communication. It is important to show respect for the person, foster an atmosphere of collaboration, validate their emotional distress and engender hope. Focus on the person’s emotional state rather than their behaviour. Educate your staff (receptionist, practice nurse) and emphasise empathy. Move from risk assessment to needs assessment. Be sure to follow up anyone who does not return for appointments.
A useful mnemonic to guide staff dealing with people who repeatedly self-harm is REASSURE:13
- Respond sensitively
- Explore the reasons
- Accept the repetitive nature of the self-harm
- Support the person
- Seek support for yourself
- Understand the underlying reasons
- Recognise it is a coping strategy
- Examine associated stresses.
Managing countertransference
Strong countertransference feelings may be expressed in various ways: the wish to discharge a patient or transfer them to another facility; to become overinvolved in the case; to be punitive or critical; or to berate a colleague for not doing something more effective to prevent a repeated self-injury.
You and your staff will often need support and the opportunity to disclose these uncomfortable and conflicting feelings in a confidential and trusting environment such as individual supervision or staff groups. Junior doctors can benefit from individual sessions with senior colleagues, but only if their relationship with their senior feels safe.14
Reducing the risk of repeated self-harm
There are no widely accepted tools to assess risk of repeated self-harm, but psychosocial interventions can help to reduce the risk of repetition.15 These interventions include therapies such as cognitive behavioural therapy (CBT), psychodynamic interpersonal therapy and problem-solving therapy, and outreach such as care-provider initiated contact, rapid crisis response, solution-focused counselling and motivational support to engage in therapy.
Self-harm is markedly increased in people with borderline personality disorder, with a prevalence of 75%.1 Psychological interventions have been shown to reduce repeated self-harm in people with borderline personality disorder. Dialectical behaviour therapy, CBT, mentalisation-based therapy and psychodynamic interpersonal therapy are helpful when added to a recovery-based model of care.16 Pharmacotherapy has no effect on repeated self-harm unless there is an associated major depressive disorder. Referral to a psychologist or psychiatrist trained in these therapies is recommended, in partnership with ongoing support from the GP.
For children and adolescents, CBT and dialectical behaviour therapy reduce repetition. Group therapy is helpful. Five factors are important when designing interventions for children and young people: motivation to change; maintaining sobriety; familial or non-familial support; healthy sleep; and promoting positive affect.
With older adults, reduction in self-harm requires a multifaceted, multilayered approach including managing depression and addressing factors such as social isolation and chronic pain.
There are higher rates of self-harm in Aboriginal and Torres Strait Islander communities, and it is essential for members of those communities to determine interventions, keeping in mind postcolonisation history (incarceration, collective grief, trauma and loss) and psychosocial factors such as unstable accommodation, poor access to health care, unemployment, social exclusion, stress, trauma and substance misuse.17
GPs can refer patients to online self-help programs that can reduce suicidal thoughts and hopelessness. Online resources are available at ReachOut Australia (https://au.reachout.com), SANE Australia (www.sane.org), Help Guide (https://helpguide.org) and beyondblue (www.youthbeyondblue.com). GPs also have access to the Royal Australian and New Zealand College of Psychiatrist guidelines on the management of deliberate self-harm.18
Conclusion
Self-harm is a common sign of distress in adolescents and young adults, who will often make contact with the health system through a GP. An empathic, supportive and nonjudgemental approach in general practice can go a long way to reducing repetition, and effective ongoing intervention may save a life. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.