Body dysmorphia in boys and young men

Body dysmorphic disorder shares anorexia nervosa’s hallmark clinical feature of disturbed body image, but it occurs as often in men as women. Young men and boys who are excessively concerned by perceived flaws in their appearance may hide their symptoms out of shame or embarrassment, but careful screening and questioning in general practice can uncover the problem.
Well known eating disorders such as anorexia nervosa (AN) or bulimia nervosa occur predominantly in women and girls, whereas body dysmorphic disorder (BDD) is a lesser known disorder that occurs at similar rates in both sexes.1 Although BDD is classified as an obsessive compulsive disorder, it shares AN’s hallmark clinical feature of disturbed body image.2,3 BDD is more common than AN and has an estimated prevalence of 2.2% in adolescents.4 However, there is lower awareness of the disorder among doctors and the community and it remains underdiagnosed in men and boys, who may be secretive about their symptoms because of embarrassment or shame, leading to reluctance to seek psychiatric treatment.5
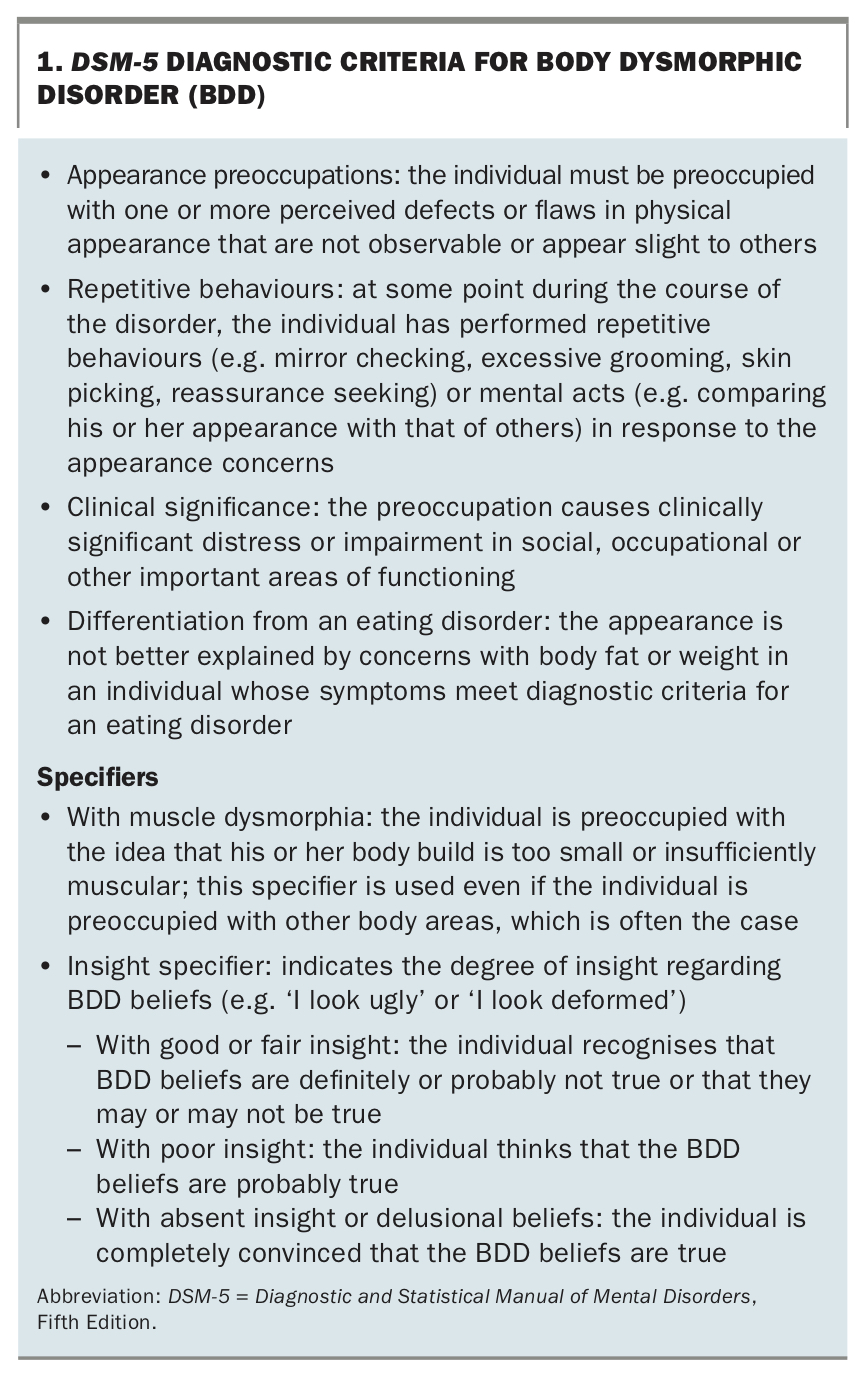
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnostic criteria for BDD are given in Box 1. BDD is characterised by excessive concerns about perceived flaws in one’s physical appearance (which appears normal to an objective observer), with associated behavioural or mental acts to try to hide or reduce these perceived flaws.2 Although dissatisfaction with appearance – or ‘dysmorphic concern’ – is relatively common in teenagers generally, the ‘imagined ugliness’ that characterises BDD results in individuals spending many hours a day preoccupied with their appearance.6 This can disrupt their functioning to the point of being socially isolated or even housebound, with a profound negative impact on their studies and work.7
{kind=link}
The intensity of impaired insight can vary both between individuals and over time, with about half of those with BDD maintaining their beliefs with delusional conviction.8 The DSM-5 criteria therefore detail an optional specifier of ‘with absent insight or delusional beliefs’ for patients who hold a high level of conviction that their BDD beliefs are accurate and aligned with reality (Box 1).2
Common presentations
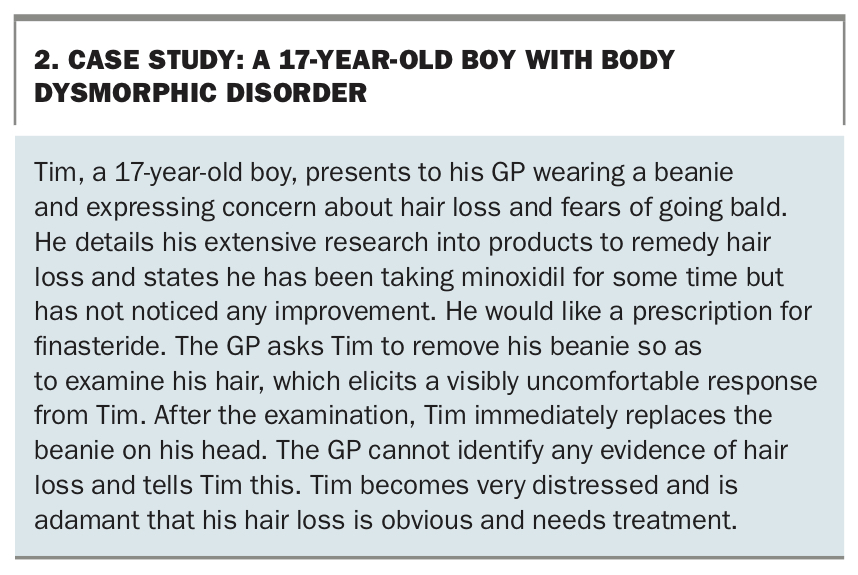
In addition to the hallmark feature of a disturbed body image, BDD has other similarities to eating disorders with marked body image concerns, particularly AN. These include onset in the mid teens, a chronic course (with fewer than 10% of patients achieving full remission) and a high intensity of negative emotions, with maladaptive control of intrusive thoughts.9-11 However, the key difference lies in the physical area of concern: people with AN are predominantly concerned with body weight and shape, whereas the most common areas of concern for people with BDD are the head and face, specifically the skin, hair and nose (see case study in Box 2).12
{kind=link}
The patient’s perceived flaws induce intense shame and are often perceived as a problem that can be remedied by cosmetic procedures, rather than psychiatric treatment. Dermatologists are the physicians most often seen by patients with BDD.13 However, cosmetic procedures usually do not decrease BDD symptoms, and the patient’s subsequent disappointment can manifest in intense distress and anger.12 This has prompted calls for BDD screening in cosmetic treatment settings.14
Heightened awareness and symptom screening are also recommended for sexual-minority adolescents, among whom body dissatisfaction levels may be higher.15-17
Muscle dysmorphia
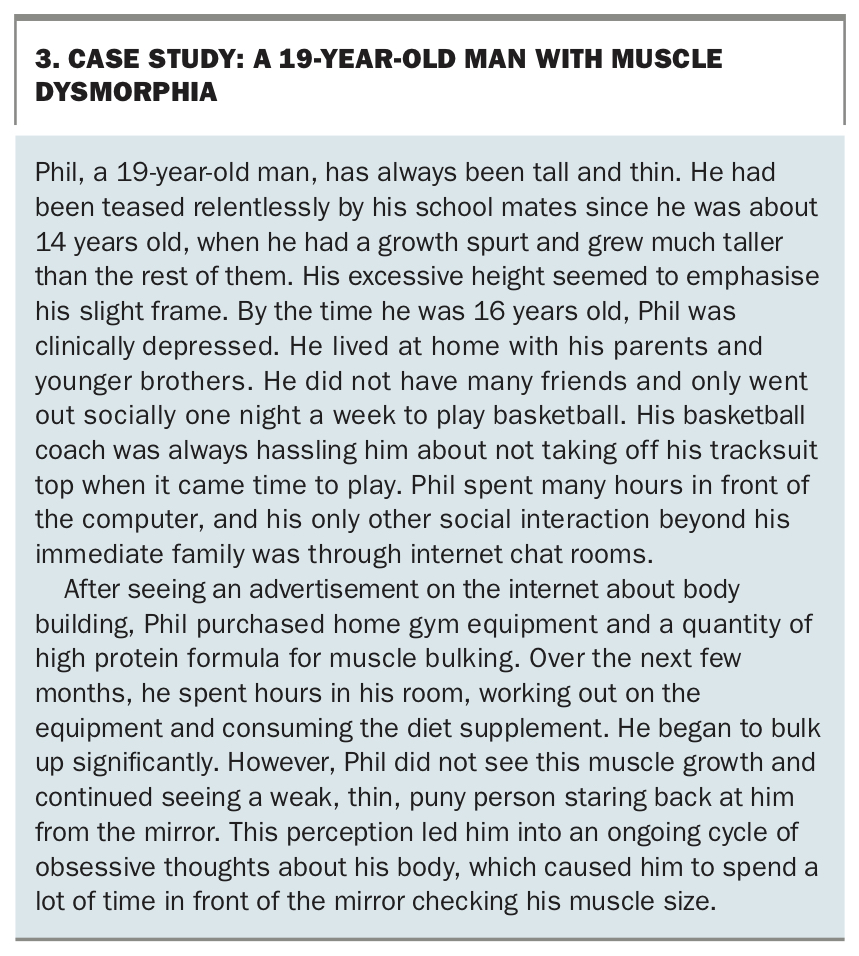
A specific form of BDD that is more common in adolescent boys than girls is muscle dysmorphia (Box 1).2 Often termed ‘reverse anorexia’, muscle dysmorphia is characterised by the belief that one’s body is too thin and puny, resulting in extreme behaviour to gain muscle mass.12 It is believed to be partly caused by internalisation of media messages showcasing an idealised male physique.17 In an attempt to achieve a muscular appearance, people with muscle dysmorphia may adopt specific diets, spend many hours in the gym, use anabolic steroids or wear padded clothing to enhance their perceived muscularity (see case study in Box 3).12
{kind=link}
Comorbid conditions
The inclusion of BDD in a spectrum of ‘body image’ disorders has been widely proposed because of its substantial overlap with eating disorders.18,19 Although they remain distinct conditions, AN is more common in individuals with BDD and, conversely, a large proportion of people with AN show dysmorphic concern beyond that about their weight and shape.20
BDD is also associated with increased rates of comorbid mood and anxiety disorders. Given that dysmorphic concern may arise as a symptom of various psychiatric conditions, it is important to delineate the symptoms of BDD.6 Social anxiety and avoidance are particularly common, as individuals with BDD may believe that their perceived flaws will be an object of derision, leading to significant disability in social and occupational functioning.12 Living with the constant burden of feeling deformed contributes to low self-esteem and lack of self-worth, with depression being the most frequent comorbid condition.21 Suicidality is a profound concern; people with BDD are four times more likely to have suicidal ideation and 2.6 times more likely to attempt suicide than the general population.22
Screening
The Dysmorphic Concern Questionnaire (DCQ) can be used as an aid in recognising BDD symptoms. The DCQ is a brief questionnaire that assesses cognitive, affective and behavioural processes associated with preoccupation with a perceived physical flaw.23,24 Screening is instrumental in facilitating discussion between GPs and patients about appearance concerns, using the following questions:
- Have you been very concerned about some aspect of your physical appearance?
- Have you considered yourself misformed or misshapen in some way (e.g. nose, hair, skin, sexual organs, overall body build)?
- Have you considered your body to be malfunctional in some way (e.g. excessive body odour, flatulence, sweating)?
- Have you consulted or felt you needed to consult a plastic surgeon, dermatologist or physician about these concerns?
- Have you been told by others or your doctor that you are normal in spite of you strongly believing that something is wrong with your appearance or bodily functioning?
- Have you spent a lot of time worrying about a defect in your appearance or bodily functioning?
- Have you spent a lot of time covering up defects in your appearance or bodily functioning?
In answering these questions, respondents rate their concern about their physical appearance relative to others on four-point scale ranging from 0 (not at all) to 3 (much more than most people). The DCQ is scored by summing all items, with possible scores ranging from 0 to 21. A score of 9 or higher indicates the need for further psychiatric assessment.
Treatment
A primary barrier to successful treatment of BDD is the patient’s engagement with, and acceptance of the need for, a psychiatric or psychological treatment. Given that up to half of individuals with BDD do not seek support for their disorder and may request a referral for cosmetic treatment, GPs are ideally placed to hold initial conversations with patients to educate them about the disorder and the effective treatments available.25 As people with BDD hold strong convictions about their perceived flaws, conversations should focus on exploring the distress and disability associated with the perceived flaws, rather than details of the flaws.
In these conversations, it is also useful for GPs to explore actions that the patient has taken to hide or remove the perceived flaws, so they can gauge the extent of associated distress and potential need for a psychiatric referral.13 This could include asking additional questions, such as ‘Do you spend lots of time grooming and checking your physical appearance?’ and ‘Are there specific aspects of your looks that you really do not like and would change if you could?’.
An expert in the field should be involved in treatment planning for a patient with BDD. Recommended treatment approaches that have proven beneficial include psychological treatments, notably cognitive behavioural therapy. Selective serotonin reuptake inhibitors (SSRIs) are the mainstay of pharmacological treatment.26 Serotonergic antidepressants may provide additional benefit in treating comorbid psychiatric conditions, including depression, anxiety and obsessive compulsive disorder.27 As in obsessive compulsive disorder, people with BDD might require higher doses of SSRIs than are usually used to treat depression (up to 400 mg of sertraline or equivalent dose of another SSRI) and may take some months to show the full effect. Long-term treatment is required to reduce the risk of relapse.
If an SSRI alone is not sufficient to ameliorate BDD symptoms, additional pharmacotherapy might be required. This may include off-label use of an atypical antipsychotic agent, which should ideally be initiated by a psychiatrist.
When to refer
BDD is a complex disorder and requires expert treatment. GPs play an important role in recognising the symptoms, making the diagnosis, engaging with the patient and providing continuity of care, but referring the patient to a health professional versed in cognitive behavioural therapy is recommended. A psychiatrist or psychologist can also assist with diagnostic clarification if required.
Psychiatric review of medications is warranted, especially if the patient does not respond adequately to an SSRI and before using doses above those specified in the product information for the particular agent. A full risk assessment, dealing with suicide risk in particular, is imperative, and urgent psychiatric review might be required for this.
Conclusion
Body image concerns are common in the general population, particularly among teenagers. Although eating disorders predominate in women, young men are just as prone to BDD as women and, compared with women, much more so to muscle dysmorphia. These disorders can be highly distressing and disabling. For young people with body image disorders, GPs have a key role in detecting symptoms, engaging with the patient and providing ongoing treatment. Established treatments are available for these disorders, and GPs can work with their psychological and psychiatric colleagues to offer patients effective and comprehensive care. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.