Fuchs’ endothelial dystrophy. Not to be forgotten in cataract patients

Fuchs’ endothelial dystrophy (FED) causes loss of corneal clarity bilaterally and is the most common indication for corneal transplantation. Not all patients with FED are symptomatic; however, more advanced disease results in decreased vision and pain. Cataract surgery may hasten progression of this disease.
Fuchs’ endothelial dystrophy (FED) is a genetic condition that manifests bilaterally and affects the innermost layer of the cornea. It causes a reduction in the number and function of the endothelial cells. Endothelial cells, which lie on their basement membrane (Descemet’s membrane) pump fluid out of the cornea and into the anterior chamber. This process is critical to maintain deturgescence and clarity of the cornea, which has a tendency to imbibe fluid. FED is the most common indication for corneal transplantation worldwide, with an incidence of around 4% and a slight female preponderance. The pattern of inheritance is most commonly sporadic, although autosomal dominant variants do occur.1,2
FED is usually diagnosed in the fifth to sixth decade of life when the structural changes are seen as an incidental finding during an eye examination by an optometrist or ophthalmologist, or when the patient starts to become symptomatic. It is an important consideration when patients require cataract surgery, which is associated with loss of endothelial cells to a variable degree.
Symptoms of Fuchs' endothelial dystrophy
Many patients with FED are asymptomatic. In mild disease, patients may complain of transient blurred vision in the morning. The cornea normally swells overnight with the eyelids closed. This is mainly caused by reduced osmolality of the tears during sleep due to a decrease in evaporation. Opening the eyes in the morning allows the cornea to dehydrate and the vision to clear. As FED progresses, the blurred vision can last longer and eventually not clear at all due to the cornea becoming oedematous. Patients with more advanced FED can develop bullous keratopathy, where blisters form in the epithelial layer of the cornea due to severe oedema. This can become painful if the bullae rupture or from mechanical rubbing of the bullae on the eyelid with blinking. Ruptured bullae expose the cornea to the risk of infectious keratitis. Patients with FED may also experience significant glare or haloes due to abnormal scattering of light.
Differential diagnoses
The differential diagnosis for FED includes:
- postoperative corneal oedema (which usually settles over days to weeks)
- pseudophakic bullous keratopathy (late postoperative corneal decompensation due to surgical trauma to endothelial cells)
- other corneal endothelial dystrophies, usually diagnosed in childhood
– congenital hereditary endothelial dystrophy
– posterior polymorphous corneal dystrophy - iridocorneal-endothelial syndrome (which is rare, and causes unilateral endothelial changes)
- viral stromal keratitis such as herpes simplex keratitis
- corneal oedema due to previous trauma or diseases such as uveitis and glaucoma.
Assessment and diagnosis
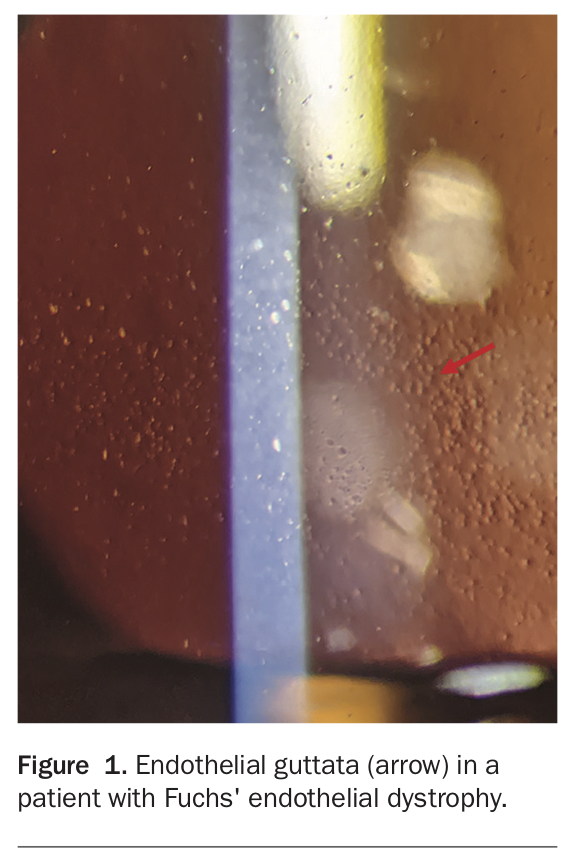
The diagnosis of FED is made through clinical examination of the patient’s eyes using a slit lamp. Hyaline excrescences of Descemet’s membrane occur and appear clinically as guttata. These guttata create a typical ‘beaten metal’ appearance of the endothelium and are best seen on retroillumination or specular reflection of the cornea (Figure 1). In more advanced disease, stromal and epithelial oedema may be visible; and eventually, small blisters called bullae can be seen in the epithelium in late-stage disease. Descemet’s folds are striae in Descemet’s membrane which occur in an oedematous cornea.
{kind=link}
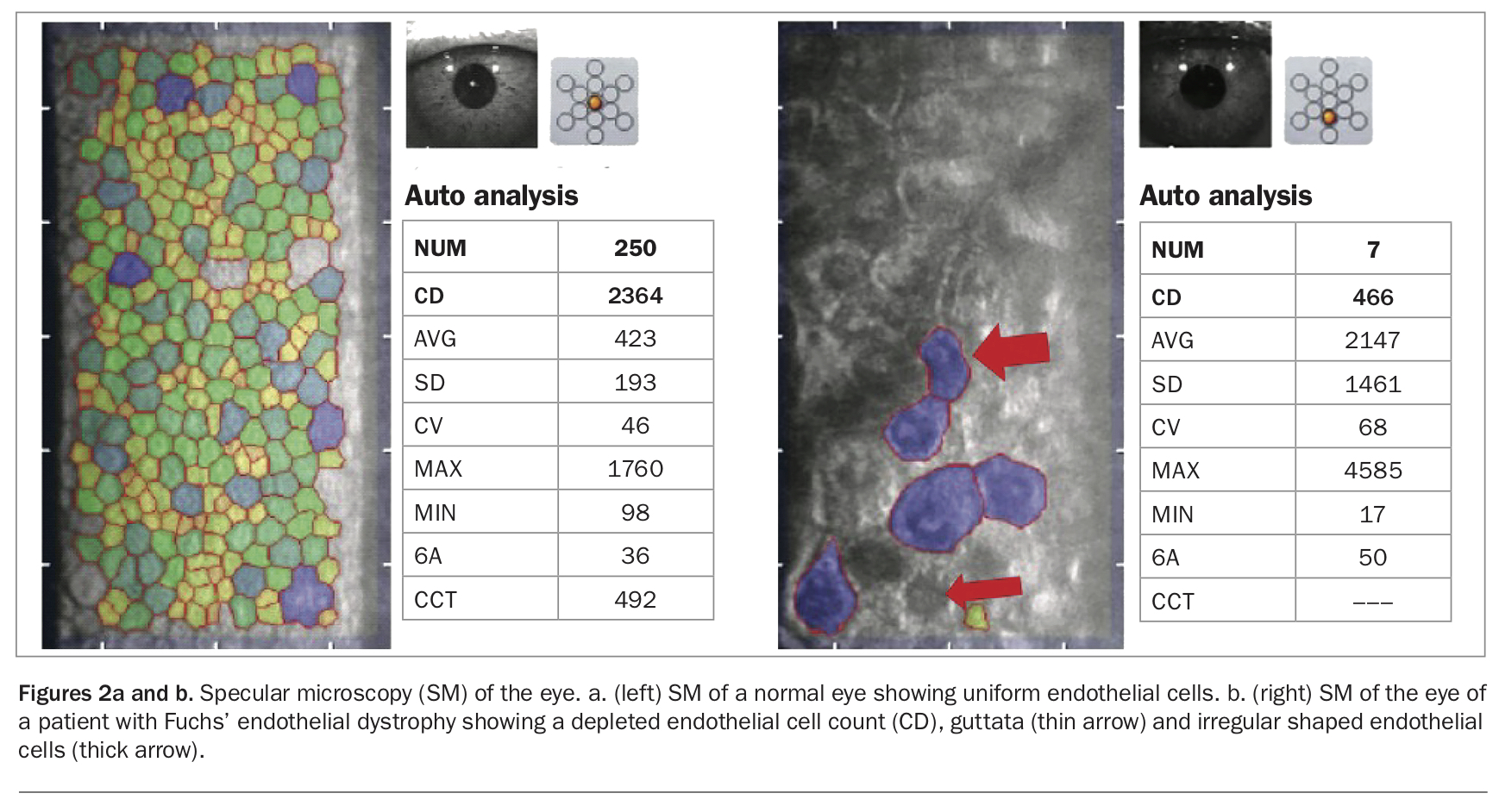
Imaging of the corneal endothelium with a specialised specular or confocal microscope is possible and aids in diagnosis and monitoring of the disease. These instruments can image the endothelial cells directly, count their number, assess their volume and give a measure of how uniform they are relative to each other (Figures 2a and b). Measuring the thickness of the cornea with pachymetry or a topographer is useful in assessing for corneal oedema and monitoring progress of the disease.
{kind=link}
Treatment
Medical
Most patients with FED do not require treatment. Most will not require corneal transplantation.
In patients who are starting to become symptomatic, topical hypertonic saline can be used in drop or ointment form. Hypertonic saline dehydrates the cornea and can help improve the patient’s vision temporarily. Hypertonic saline ointment used at night before bed can help to prevent the cornea from swelling overnight and hence reduce blurred vision on waking. A hair dryer held at arm’s length can be used to dry out the cornea.
Surgical
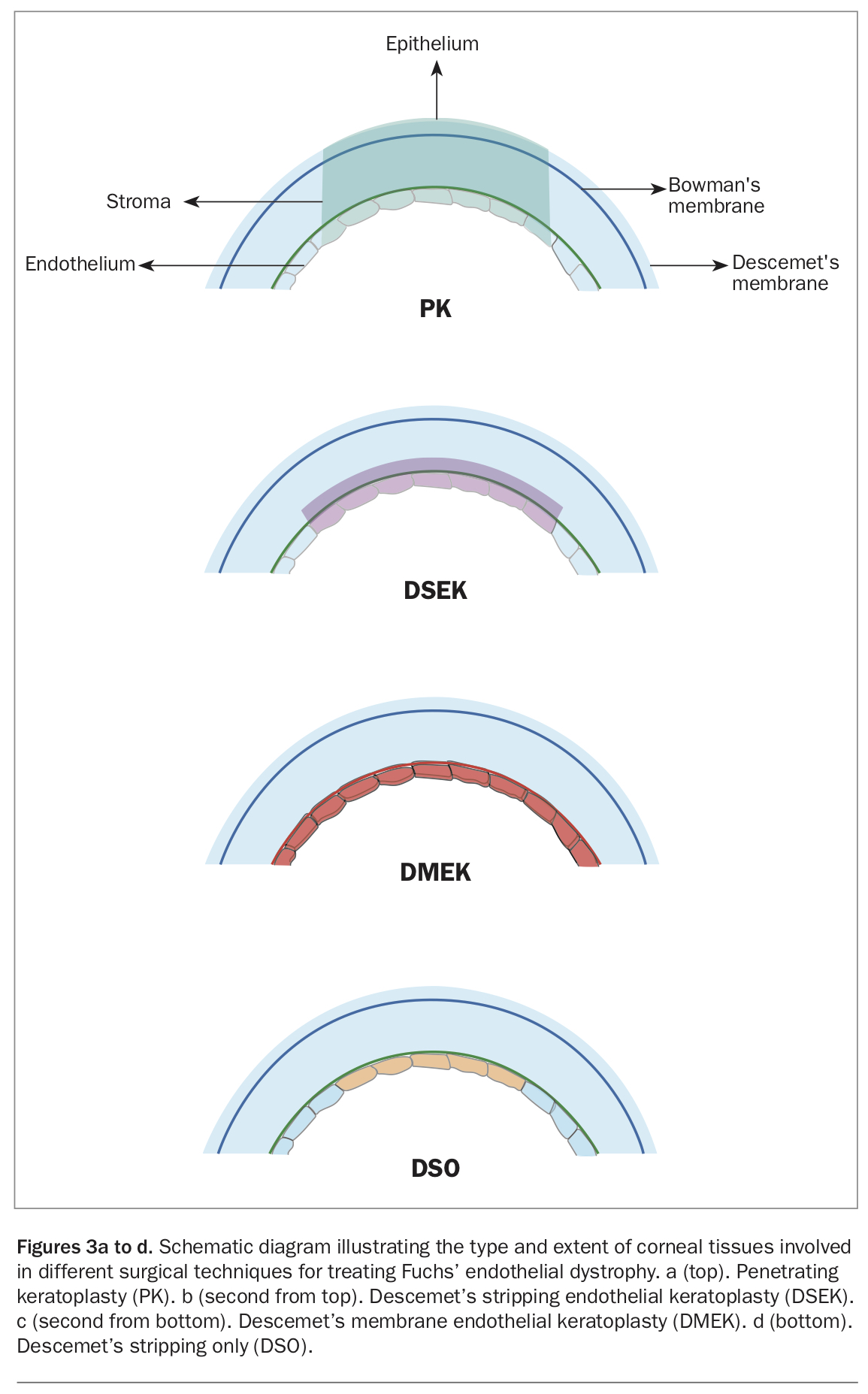
The surgical treatment for FED has evolved significantly over the years (Figures 3a to d). Previously, only a full thickness corneal transplant (penetrating keratoplasty [PK]) was possible to treat the disease. PK involves replacing a central full thickness button of the diseased cornea with a donor cornea, which is secured in place with 16 sutures that remain in the eye for at least 12 months. The recovery period is prolonged. PK still rarely has a place in treating patients with coexisting abnormal anterior segment anatomy.
{kind=link}
Modern surgical techniques for corneal transplantation replace only the diseased layers of tissue, with quicker recovery and better long-term outcomes. In the case of FED, only a very thin layer of the endothelium and Descemet’s membrane are removed and replaced. Descemet’s stripping endothelial keratoplasty (DSEK) involves stripping the host’s Descemet’s membrane and diseased endothelium and replacing it with a button of cadaveric donor tissue which has a small amount of corneal stroma together with Descemet’s membrane and the endothelium. Descemet’s membrane endothelial keratoplasty (DMEK) is a newer technique in which a super-thin scroll of only Descemet’s membrane and the endothelial cells is harvested and placed into the eye. DMEK is a technically more challenging procedure but confers several advantages over DSEK. These include being an anatomically correct replacement of the abnormal tissue, affording the possibility of better postoperative vision;3 being sutureless and performed through a very small incision; and having a lower rejection rate (2.6% vs 7.9% for DSEK4).
At the completion of both surgical procedures, a bubble of air is placed in the anterior chamber and the patient must position supine for around 48 hours postoperatively (with short breaks allowed in that time). This is to support the graft while it comes out of hibernation and starts functioning; it is the pumping action that then creates a fluid gradient which holds the graft in position. The patient is started on topical corticosteroids, often at a low dose lifelong, to prevent transplant rejection.
A new procedure called Descemet’s stripping only (DSO) or Descemet’s stripping without endothelial keratoplasty (DWEK) can be used in a small subset of patients with FED in whom only the central cornea is involved with an adequate reservoir of peripheral endothelial cells.3 In this procedure, only the central 4 mm of diseased Descemet’s membrane and endothelium are removed. They are not replaced with a transplant. The patient is prescribed postoperative rho-kinase inhibitor drops that aid in the migration of the peripheral endothelium to cover the central stripped area. This procedure eliminates the risks associated with endothelial grafts, such as detachment and rejection, and minimises the need for postoperative corticosteroid drops. It also decreases the burden on eye banks to provide tissue for corneal transplants. Should the cornea fail to clear after DSO then an endothelial transplant can still be performed.
FED and cataract surgery
An important time in the of management of a patient with FED is when planning cataract surgery. Any patient who undergoes cataract surgery will lose some endothelial cells due to the iatrogenic trauma caused by intraocular surgery. The paradigm has shifted somewhat over the years in terms of when to perform cataract surgery in a patient with FED. In the past, the mentality was to wait as long as possible before embarking on cataract surgery, with the fear that the cataract surgery would induce endothelial failure and necessitate a corneal transplant. However, as surgical techniques have evolved there is now an argument for intervening before the cataract becomes too dense, hence reducing the risk of intraoperative endothelial cell loss.
Patients with mild FED who still have adequate endothelial cell counts and are not yet symptomatic of the FED may be able to recover after cataract surgery, with particular care and specific surgical steps employed to protect their endothelium intraoperatively.
In patients who already have endothelial failure, are symptomatic of their FED or have very low endothelial cell counts then a combined procedure with cataract extraction and a corneal graft or DSO is indicated. Patients with only mild or intermediate disease may tolerate cataract surgery alone; however, they must be informed of the risk of needing a corneal procedure should their cornea not recover in the immediate or late postoperative period. The prognosis after a successful corneal graft or DSO is excellent, with many patients able to attain very good postoperative vision.5,6
Conclusion
FED is the most prevalent corneal dystrophy. It is often asymptomatic, but in more advanced stages can cause significant morbidity for patients. It is important to assess all patients undergoing cataract surgery for signs of FED. As knowledge about endothelial cell function and surgical techniques evolves, patients with FED are able to have excellent outcomes. Future directions for treatment of FED will likely involve stem cell treatment to replenish the lost endothelial cells, and many groups worldwide are actively seeking this solution. MT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.