COPD exacerbations: a pragmatic approach to prevention, diagnosis and management

Prevention, timely diagnosis and evidence-based management of exacerbations of chronic obstructive pulmonary disease (COPD) are crucial in primary care, to maintain the wellbeing of people living with COPD.
- Exacerbations of COPD can be infective (bacterial or viral) or noninfective.
- Early diagnosis and treatment of exacerbations is crucial to prevent hospital admission and delay decline in lung function.
- Principles of management are to reverse bronchoconstriction (with bronchodilators) and inflammation (with corticosteroids), reduce dyspnoea (through airway clearance, controlled oxygen therapy and ventilatory assistance) and treat or remove triggers (with antibiotic therapy).
- Prevention of exacerbations is important, encompassing both pharmacological and nonpharmacological treatment in a stepwise approach.
Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease that is a leading cause of death globally. Smoking is the most important modifiable contributing risk factor, and smoking cessation can slow decline in lung function.1,2 COPD exacerbations are defined as an acute worsening of respiratory symptoms that require a change in management. This management can be through self-management by the patient using their COPD action plan, GP care or, for more severe exacerbations, emergency department and hospital care. Prevention, timely diagnosis and effective management of exacerbations of COPD are of the utmost importance in primary care, to maximise the wellbeing of people living with COPD.
This article discusses the steps in diagnosis and the primary care management of patients with an exacerbation of COPD. It also outlines the recommended components of a strategy to prevent further COPD exacerbations.
Epidemiology of COPD exacerbations
Exacerbations of COPD are the major cause of morbidity and mortality in patients with COPD and contribute significantly to healthcare costs in Australia. In 2018, 7113 people (3783 men and 3330 women) died from COPD, making it the fifth leading cause of death.3 In 2015-16, COPD cost the Australian health system an estimated $977 million: $536 million for hospital care, $189 million for nonhospital medical services and $252 million for pharmaceuticals.3 An 18-fold variation in hospitalisation rates for COPD is seen across jurisdictions nationally, emphasising the need to achieve better equity of healthcare access for all Australians with COPD.4
Causes of COPD exacerbations
A range of factors can trigger COPD exacerbations, most commonly bacterial or viral infections and ambient pollution.5 Nearly half of COPD exacerbations are caused by bacterial infection.6 Respiratory viral infections may become more serious, with bacterial coinfections worsening the exacerbation. The most frequent bacterial causes of COPD exacerbations are Haemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis and Pseudomonas aeruginosa.
Conventional culture-based methods have confirmed the role of bacteria in the progression of lung disease. Further, investigations into the lung microbiome, which includes bacterial, fungal and viral elements, have found that complex microbial communities interact with the host immune system to influence clinical outcomes.7,8 Exacerbations and respiratory infections are significant clinical features in progression of COPD.9 The composition of the lung microbiome changes with smoking and stage of COPD severity, during exacerbations and with treatment of COPD during stability and acute episodes.10
Air pollutants, including fine particle matter, ozone, nitrogen dioxide and sulfur dioxide, have been associated with increased exacerbations and increasing mortality.11 Extremes of temperature, both hot and cold, have also been implicated.12 Other causes of acute respiratory distress, including heart failure, pulmonary embolism and pneumothorax, should also be considered in the differential diagnosis of COPD exacerbations.
Pathology and pathophysiology
Respiratory infections and inhaled irritants increase inflammation (especially infiltration by inflammatory cells) and excess respiratory secretions in the airway lumen. These pathological features in the airway during an exacerbation lead to the pathophysiological changes of worsened airflow obstruction, dynamic hyperinflation and sputum production. The end result is a cascade of increasing symptoms, fatigue and respiratory failure, particularly in more severe exacerbations.
Diagnosis of COPD exacerbations
A COPD exacerbation should be suspected in patients with an acute change in breathlessness, with or without a change in sputum production or colour or fever. Early diagnosis and treatment of exacerbations is crucial as it can prevent hospital admission and delay decline in lung function.13,14
In a mild exacerbation, physical examination at rest may have unremarkable results; however, exertional dyspnoea or wheeze may be unmasked after walking a short distance. In moderate to severe exacerbations, observation may show an increased respiratory rate, hypoxia, tachycardia and fever. On chest auscultation, a wheeze or crackles may be present. The patient should be thoroughly examined, and other potential causes of acute breathlessness should be considered, including congestive cardiac failure, cardiac arrhythmia and, less commonly, pulmonary embolism.15 Further diagnostic testing with an ECG, basic blood tests and chest x-ray is often warranted to guide further treatment.
Patients with a severe exacerbation presenting with significant hypoxia, respiratory distress or altered mental status require additional supports and should be referred to the local emergency department for review.16
Management of COPD exacerbations
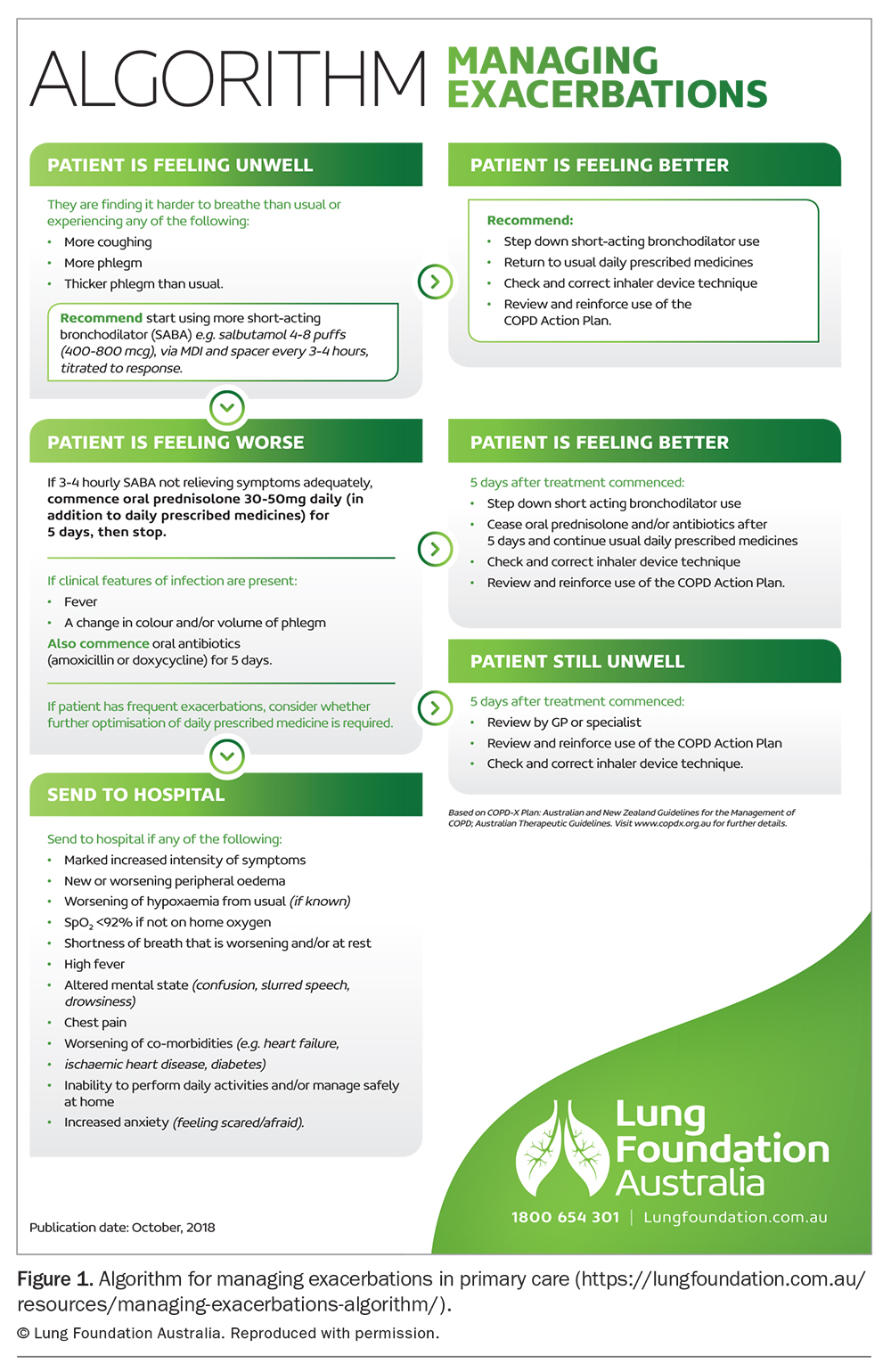
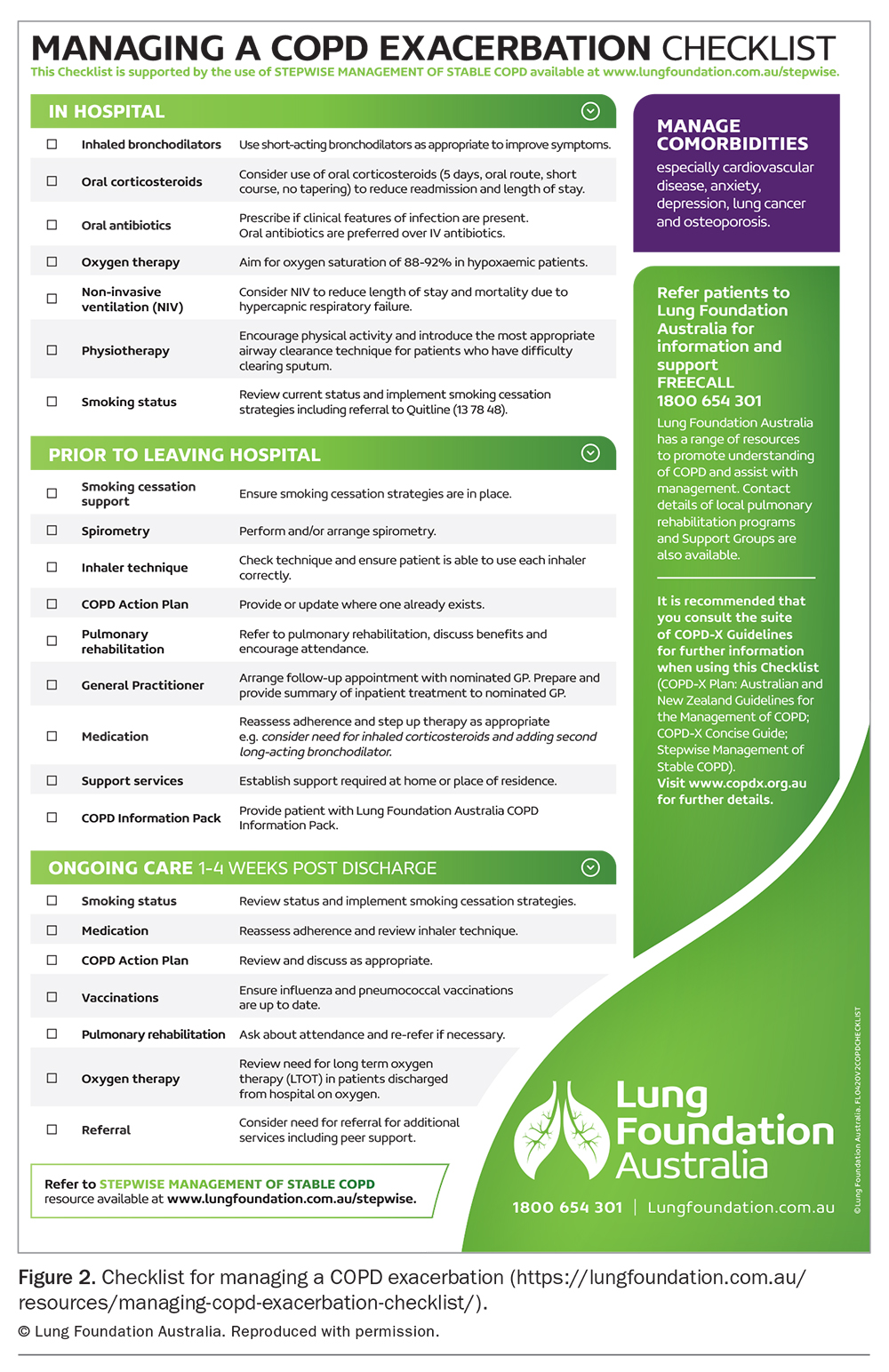
Early identification and treatment of a COPD exacerbation are important, as each exacerbation can contribute to progressive loss of lung function and reduction in quality of life.17 Treatment usually begins with a patient self-management plan (https://lungfoundation.com.au/resources/copd-action-plan/) and may require medical review in primary care (Figure 1) or hospitalisation (Figure 2).
{kind=link}
{kind=link}
Principles of management of a COPD exacerbation are to:
- reverse bronchoconstriction (with bronchodilators)
- reverse inflammation (with corticosteroids)
- reduce dyspnoea (through airway clearance, controlled oxygen therapy and ventilatory assistance) and
- treat or eliminate triggers (with antibiotic therapy).
Bronchodilators
The initiation of a regular short-acting beta-agonist (e.g. salbutamol) is recommended for all patients with a COPD exacerbation as it provides immediate relief of dyspnoea, although high-quality supporting evidence is limited.2 A long-acting bronchodilator in the form of a long-acting muscarinic antagonist (LAMA) can be either continued during the exacerbation or temporarily replaced by a short-acting muscarinic antagonist (ipratropium).
Bronchodilators can be delivered via either a metered-dose inhaler with spacer or a nebuliser. A Cochrane review found no significant difference in outcomes of patients in a nonintensive care setting between these two methods of delivery.18 Thus, the method of delivery should be determined by infectious risk, cost and the patient’s ability to co-ordinate an inhaler with spacer. The dose and frequency can be titrated to symptom severity.
Corticosteroids
Systemic corticosteroids (e.g. prednisolone) suppress airway inflammation to improve airflow, reduce the risk of treatment failure by over half compared with placebo, shorten the duration of hospitalisation and lower the rate of relapse at one month.19,20 Oral administration is usually preferred, as there is no significant difference in outcome compared with parenteral administration.21 A five-day course of prednisolone is recommended (e.g. 30 to 50 mg daily, not tapered), with a Cochrane meta-analysis showing no difference in treatment efficacy compared with longer courses, which are associated with an increased risk of sepsis and corticosteroid-related complications.22 Evidence is also emerging supporting individualised treatment according to blood eosinophilia count, as eosinophilic inflammation is more likely to be corticosteroid-responsive.23
Antibiotics
Infective exacerbations of COPD should be suspected in patients presenting with increased sputum production and a change in sputum colour, with or without fever. Therapeutic guidelines recommend treatment with oral amoxicillin or doxycycline for five days for patients whose clinical presentation suggests a bacterial exercerbation.24
Noninfective and viral exacerbations of COPD are common and can be challenging to distinguish from bacterial infection. Inflammatory markers, including
C-reactive protein, can be measured to guide antibiotic therapy.25 PCR testing of swabs for respiratory viruses including SARS-CoV-2 can be considered, as viral coinfection is detected in 25% of infective exacerbations.25 Sputum culture is not routinely recommended for exacerbations because persistent colonisation of the lower airways in many patients means that positive culture results do not always indicate active infection.1
Airway clearance
Airway clearance techniques (ACTs) may be considered for patients with an exacerbation or with daily sputum production.2 ACTs help optimise sputum clearance to reduce coughing, slow decline in lung function and reduce the frequency of exacerbations. ACTs that utilise positive expiratory pressure resistance may be of greater benefit than other therapies.26 Referral to a chest physiotherapist is recommended for patient education and training in ACTs.
Respiratory support
In people with COPD, the oxygen saturation target should be in the range 88 to 92%. Overoxygenation increases mortality and the risk of hypercapnia.27 If an acute exacerbation leads to hypercapnic respiratory failure (PaCO2 greater than 45 mmHg and pH less than 7.35 on arterial blood gas assessment) then hospital admission is required for noninvasive ventilation, as this reduces mortality.28
Care after an exacerbation
Following the patient’s discharge from hospital or acute management in primary care, COPD management should be reassessed, including the level of physical activity, spirometry and referral for pulmonary rehabilitation (Figure 2). Pulmonary rehabilitation reduces breathlessness, improves exercise capacity and wellbeing and reduces exacerbations.29 All medicines should be reviewed, as well as inhaler technique (useful video resources are available at www.lungfoundation.com.au). Pneuomococcal, influenza and COVID-19 vaccination status should be checked, smoking cessation encouraged and the COPD written action plan updated. Any chest x-ray abnormalities should be reviewed for resolution, with repeat chest x-ray in four to six weeks.2
Prevention of exacerbations
Preventing further exacerbations is crucial as exacerbations contribute to disease progression and mortality. Exacerbations are a strong predictor of future exacerbations.30 Prevention of exacerbations encompasses both pharmacological and nonpharmacological components.
Smoking cessation is essential. Recommended strategies include combination long and short-acting nicotine replacement therapy, medications (e.g. varenicline) and Quitline referrals for counselling.
Long-acting inhaled medicines should be optimised using a stepwise approach, along with regular patient education on inhaler technique to ensure appropriate delivery of medication.2 Vaccinations should be kept up to date according to Australian Immunisation Handbook recommendations, to reduce the chance and severity of infective exacerbations.31
All patients with dyspnoea on exertion, especially after hospitalisation for an exacerbation, should be offered referral to pulmonary rehabilitation (https://lungfoundation.com.au/patients-carers/support-services/lung-disease-and-exercise/pulmonary-rehabilitation/). This has been shown to reduce patient symptoms and hospitalisations, as well as to improve mental health.17
Areas of uncertainty
The current definition of a COPD exacerbation is subjective, defined as the worsening of respiratory symptoms requiring a change in management.17 Diagnosis can be difficult, with many comorbidities both mimicking and causing exacerbations. These include asthma, pneumonia, pulmonary embolism and cardiovascular events. Predictive factors for short-term hospital readmission have been proposed.32,33 Risk factors include comorbidities, frailty, low lung function, socioeconomic disadvantage and hypercapnic respiratory failure.34 Emerging evidence suggests that, in the future, artificial intelligence may be able to assist with accurate diagnosis, phenotype characterisation and prognosis prediction through access to databases of electronic medical records on patients with COPD.35
Conclusion
A pragmatic, collaborative approach to diagnosis and treatment of COPD exacerbations can enhance the partnership between clinicians in primary care and tertiary care, to achieve better lives for people with COPD. By effectively managing exacerbations and, importantly, implementing systematic approaches to preventing exacerbations, our multidisciplinary care will keep people with COPD as well as possible in the community. MT
COMPETING INTERESTS: Associate Professor Dabscheck and Professor Yang are Co-Chairs of the Lung Foundation Australia COPD-X Guidelines Committee. Dr Wagner, Ms Shaw and Dr Kung: None.
Acknowledgments: The authors gratefully acknowledge all of the contributors to the Lung Foundation Australia COPD-X Guidelines and Concise Guide, and Lung Foundation Australia for permission to reproduce the figures.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.