Smoking, alcohol and weight – primary care in the preconception, pregnancy and postnatal periods

Addressing smoking, alcohol consumption and weight during preconception, pregnancy and postnatal periods can significantly optimise health outcomes for women and children. GPs can be guided by best-practice recommendations to undertake evidence-based assessment, provide advice and arrange referrals to support women to improve these health behaviours.
According to the WHO, proactively addressing smoking, alcohol and weight before conception and in pregnancy is one of the most important ways healthcare providers can optimise health outcomes for women and babies.1,2 Support provided by healthcare providers during the preconception, antenatal and postnatal periods is effective in reducing risks of harm from smoking, alcohol consumption and weight and improving outcomes for current and future pregnancies.3-5 Pregnant women regard healthcare providers, including GPs, as a trusted information source and welcome their support. Over two-thirds (69%) of pregnant women who smoke want help to quit; over 90% of women indicate they want to be asked about alcohol use in pregnancy, advised of its harms, and supported to abstain; and 80% of women want support regarding their weight gain, nutrition and physical activity.6-8 Despite women wanting a high level of care, healthcare providers report multiple barriers to providing evidence-based care, including that they do not know what to ask, how to ask, what to advise and where to refer.9
Prevalence of risk factors
Smoking
In Australia, 10 to 14% of women of childbearing age (15 to 44 years) smoke tobacco.10 Although some women will spontaneously quit upon finding out they are pregnant, up to 60% continue to smoke, resulting in about 10% of women smoking during pregnancy.10,11 Of women who do stop smoking before or during pregnancy, 50 to 70% resume smoking within six months postpartum.12
Alcohol
Over half (55%) of women in Australia consume alcohol during pregnancy, often before they know they are pregnant, which is unsurprising given that 76 to 81% of all 18- to 39-year-old women in Australia report consuming alcohol.10 About 15% of Australian women consume alcohol after they know they are pregnant.10 After pregnancy, 58% of Australian women who are breastfeeding report drinking alcohol.13
Weight
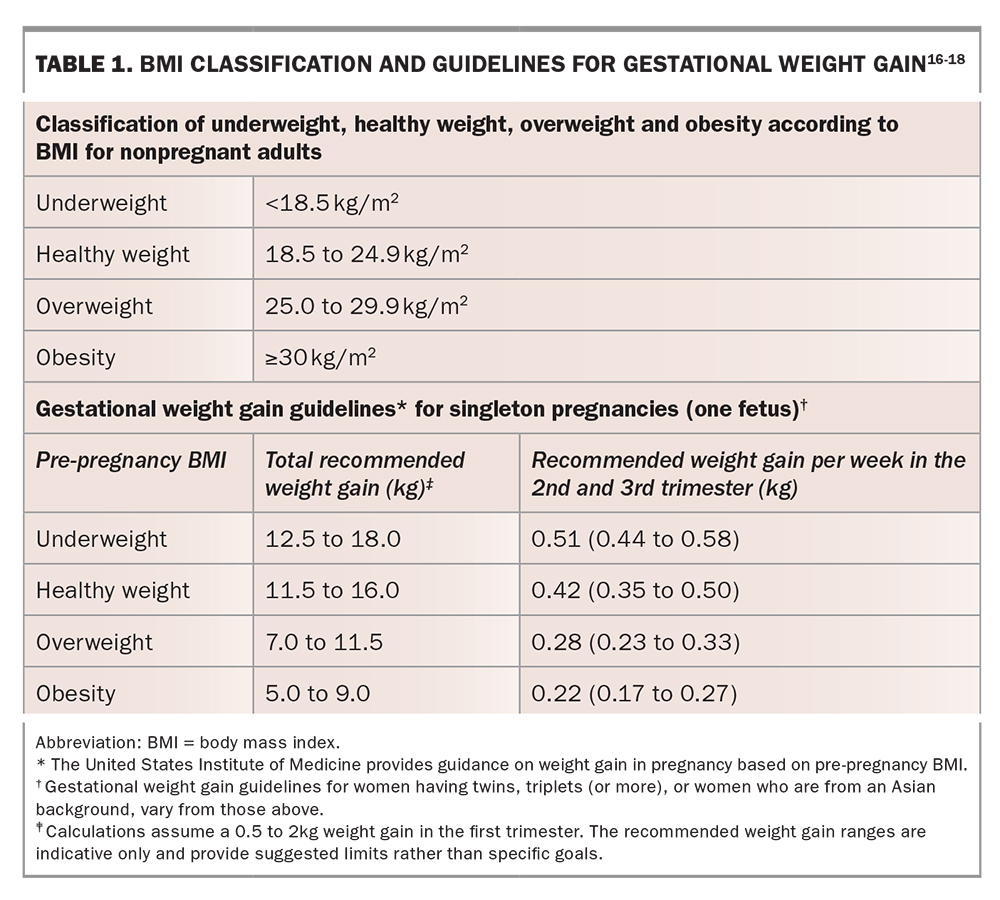
Over half (51%) of Australian women report having a body mass index (BMI) outside the healthy weight range at the start of their pregnancy and over 60% gain more weight than recommended during their pregnancy (Table 1).14-18 Postpartum weight retention is also common: most women retain between one and 5.5 kg at six to 12 months postpartum.19 Women who gain more weight than recommended during pregnancy retain 3 kg and 4.7 kg more weight at three and 15 years postpartum, respectively, than women who gain within the recommended amount, increasing long-term health risks from overweight and obesity.20
{kind=link}
For Aboriginal women, historical trauma and factors such as systemic racism, socioeconomic disadvantage and barriers to accessing health care have contributed to higher rates of smoking, high-risk alcohol consumption and weight gain in pregnancy.21-24
Impacts on the pregnancy and child
Smoking
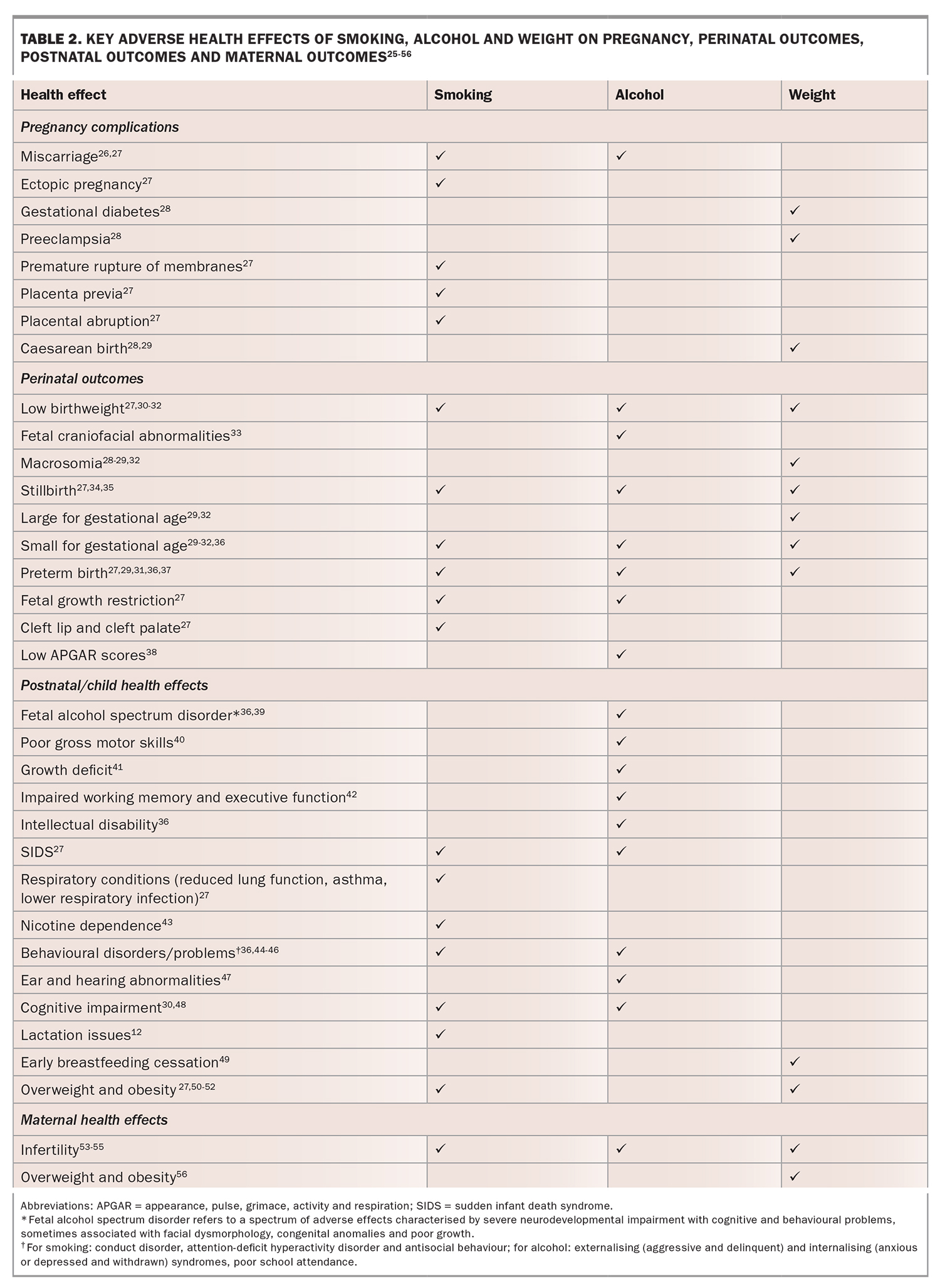
Smoking during pregnancy is associated with a wide range of pregnancy complications and adverse outcomes for the woman and her baby. There is a 71% increase in risk of infant mortality due to smoking, and impacts extend to childhood and adulthood (Table 2).25-56 Cigarette smoke contains over 7000 hazardous chemicals including nicotine, carbon monoxide, tar, benzene and heavy metals such as lead and cadmium. Many of these cross the placenta and enter the fetal circulation.30 Nicotine causes placental vasoconstriction, impacting placental blood flow, and carbon monoxide binds to haemoglobin causing fetal hypoxia.30 The resulting deprivation of nutrients and oxygen directly impacts fetal growth and the development of organs including the brain, lungs and adrenal glands. As a teratogen, nicotine can also affect the development of neurotransmitter systems and cause developmental abnormalities in the cerebral cortex, the autonomic nervous system and brainstem nuclei crucial to respiratory control.30 Quitting smoking before conception or during early pregnancy significantly reduces the risk of complications and adverse outcomes; however, quitting at any time during pregnancy can also result in reductions in risk and provide health benefits for both the woman and baby.57 Preventing relapse in the postnatal period is also crucial to reduce infant exposure to second-hand smoke and improve breastfeeding outcomes.12
{kind=link}
Alcohol
Alcohol is also a teratogen and can disrupt the development of the embryo and fetus.58 Alcohol freely passes across the placenta, resulting in similar blood-alcohol levels in the woman and unborn child.58 Alcohol consumption at any stage during pregnancy may be associated with adverse child outcomes, including birth defects (first trimester exposure), developmental delay and fetal alcohol spectrum disorder (FASD), and contributes to pregnancy complications and poor obstetric outcomes related to impaired placental blood flow and intrauterine growth restriction (Table 2).26,31,35,59-61 The risk of harm to the fetus is associated with the amount (quantity, frequency) and timing of alcohol consumption during pregnancy and is influenced by maternal factors including body composition, liver function and genetics.62
The 2020 NHMRC Guidelines to Reduce Health Risks from Drinking Alcohol state that ‘To prevent harm from alcohol to their unborn child, women who are pregnant or planning a pregnancy should not drink alcohol’, and that ‘For women who are breastfeeding, not drinking alcohol is safest for their baby’.62 These guidelines recognise that no safe level of alcohol consumption in pregnancy has been identified.
Weight
Optimising weight before, during and after pregnancy can have immediate and long-term health benefits for women and their children (Table 2). The greatest health improvements may come from preventing or managing unhealthy weight and improving diet and physical activity before conception, with benefits persisting across the pregnancy and postnatal periods.53
The mechanism by which maternal weight and related health behaviours influence child health and long-term risk of chronic disease is explained by the developmental origins of health and disease concept.63 There is strong evidence that a woman’s body composition, metabolic health, and diet quality and quantity (over and undernutrition) cause changes to the child’s physiology and metabolism via epigenetic and other mechanisms (developmental programming) and consequently influence their child’s health trajectory across the life course.64 For example, high maternal adiposity or high gestational weight gain in utero is associated with adverse fetal development.65 Although the exact mechanisms are still being determined, it is thought that adverse effects may be mediated through elevated maternal glucose and insulin levels, which drive fetal growth and adiposity and lead to increased birthweight and overweight or obesity during childhood.63 The extent to which the effects are due to the intrauterine environment, genetic factors and a shared postnatal environment is still to be determined.66
Optimising health behaviours in primary care
GPs in Australia provide antenatal care to almost 90% of women in early pregnancy and to 28% of women throughout pregnancy.67,68 Additionally, 85 to 92% of all Australian women of childbearing age (15 to 44 years) report seeing a GP during the past 12 months, of whom 4 to 7% seek care to reduce or quit smoking, 1 to 2% to reduce their alcohol intake, and 7 to 15% to reach a healthy weight.69 Between 6 and 17% of women of childbearing age specifically seek GP care for preconception family planning counselling.69 A large proportion of women (88%) then see their GP again within three to four months after the birth.68
Given these opportunities, GPs play a crucial role in supporting women to address health risk factors prior to conception, during pregnancy and postnatally. In surveys of Australian GPs, less than 20% reported routinely providing antenatal care that addresses smoking, only a third (32%) reported providing advice on alcohol consumption and 50% reported providing advice on weight gain.9,70,71 In some cases, the proportion of GPs who provide such care during preconception and postnatal periods is even lower.72
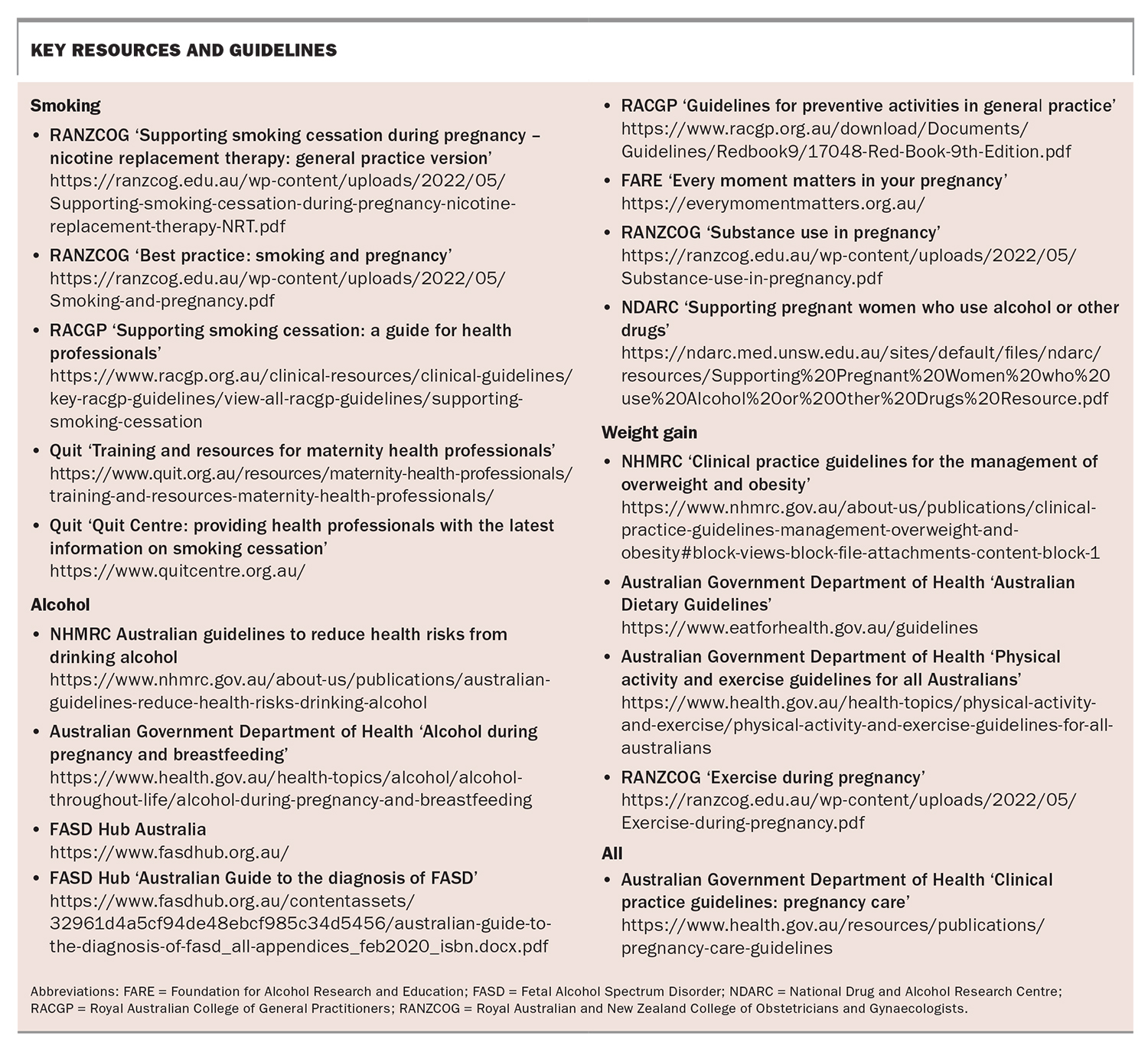
The Royal Australian College of General Practitioners guidelines and other antenatal guidelines recommend three elements of care to support women to address these risk factors: assessment of risk using a validated tool or objective measure; discussion and advice on risk and behaviour change; and referral to specialist risk-reduction services if required.23,73-75 Systematic review evidence shows that the delivery of such care is more likely to lead to changes in health behaviour if it involves collaborative conversations that invite the patient’s views, tailored discussions based on question-answer sequences and joint decision-making when planning actions to support behaviour change, than provision of advice alone.76 Recommendations for assessing and managing health risk factors in primary care are summarised in Table 3 & 3b and useful resources are listed in the Box.
{kind=link}
{kind=link}
{kind=link}
Smoking
Women who smoke are more likely to quit smoking when pregnant or planning a pregnancy than at any other time.12 Brief interventions with pregnant women significantly reduce smoking in late pregnancy and rates of low birthweight and preterm birth.77 Smoking status should be assessed for all women during preconception, pregnancy and postnatal visits. Due to the stigma attached to smoking, in particular during pregnancy, some women may not accurately disclose their smoking status, and identification of smokers may be improved using multiple response questions and exhaled breath carbon monoxide assessment.78,79 Smoking should be addressed in a supportive, nonjudgemental manner and include a discussion about the benefits of stopping smoking completely and effective ways to quit and continue to abstain from smoking.80
Behavioural support to quit smoking should be offered to all women who smoke. Behavioural support strategies include provision of pregnancy-specific self-help materials, barrier identification and problem solving, goal setting and facilitating use of social support.80,81 Referral to the Quitline is also recommended.79,82 Nicotine replacement therapy (NRT) should be considered if women are unable to achieve abstinence using nonpharmacological interventions alone.79,82 The risks and benefits of using NRT should be discussed, and oral NRT formulations offered as first-line pharmacotherapy for pregnant women to minimise exposure of the fetus to nicotine.79 If oral formulations are not tolerated or provide an insufficient dose to supress cravings, pregnant women can use NRT patches, provided they are removed at night-time to give the fetus a break from continuous nicotine exposure.82
Smoking should be addressed at every antenatal appointment with smokers and recent quitters.79,82 Rates of relapse to smoking after birth are high (50 to 70%) so it is vital that ongoing cessation support is provided at all postnatal visits for women who have quit during or before pregnancy.12 For women who are breastfeeding and are unable to achieve abstinence using nonpharmacological interventions alone, NRT should be discussed. Minimal amounts of nicotine are excreted into breast milk and absorption of nicotine through the infant gut is minimal. All forms of NRT can be used while breastfeeding (patch or oral). Infant exposure may be further reduced by breastfeeding immediately before using intermittent NRT formulations.82,83
Alcohol
Systematic reviews show that brief behavioural support delivered by healthcare providers can effectively support women to abstain from alcohol consumption during pregnancy and pregnancy planning.5,84 In line with this evidence, international and national clinical guidelines recommend that during preconception and pregnancy, clinicians provide all women with: an assessment of alcohol consumption using a validated tool; advice not to consume alcohol during pregnancy and discussion of the risks; and referral to specialist services, such as telephone-based coaching services, Aboriginal Community Controlled Health Services, or local Drug and Alcohol Clinical Services.17,85,86
The Alcohol Use Disorders Identification Test – Consumption (AUDIT-C) tool is one tool recommended for assessing alcohol intake and can be used for women during preconception, pregnancy and postnatal periods.87 AUDIT-C identifies whether a woman is consuming alcohol and provides a total score that categorises the risk of harm. For pregnant women, the following cut-off points have been established to reflect the risk of harm to the unborn child: no risk (total AUDIT-C score = 0); low risk (total AUDIT-C score of 1 to 2); medium risk (total AUDIT-C score of 3 to 4); and high risk (total AUDIT-C score of 5 or higher).88 It is recommended that referral for counselling and to clinical drug and alcohol services is offered to women drinking at medium or high risk levels, with engagement of addiction specialists for women at high risk or when alcohol dependency is known or suspected.17 Alcohol withdrawal can be harmful for women and their babies and requires inpatient supervision by experts.89
Weight
Routine measurement of weight and other clinical indicators of adiposity is recommended at clinical visits for all non-pregnant women of childbearing age for monitoring and early identification of women at risk of an unhealthy weight.90 Measured weight and height is recommended because of inaccuracies of self-reporting.91 Regular assessment of weight also provides a record of pre-pregnancy weight and BMI, enabling weight tracking from conception and the provision of accurate recommendations on gestational weight gain (Table 1).91
For pregnant women, routine measurement of weight at each antenatal visit enables early detection of weight gain at a rate that is below or above recommendations and maximises the potential impact of behavioural support and referral.92 Following pregnancy, there are no set recommendations for how quickly women should return to a healthy weight and BMI; however, it is recommended that women lose additional pregnancy weight so it is not carried into subsequent pregnancies and later life.
It is recommended that GPs discuss the benefits of a healthy weight for life stage with all women, explore the context of the behaviours that contribute to an unhealthy weight, and support women to plan their dietary and physical activity behaviour change.16,17 Referral to allied health professionals, including dietitians, is recommended for women before, during and after pregnancy if additional weight management and behavioural support is needed.16,17 Intensive weight loss interventions, including very low energy diets, weight loss medications or bariatric surgery, may be appropriate for nonpregnant women depending on their individual circumstances but are not appropriate during pregnancy.16
Further considerations
In this article, we refer to pregnant ‘women’ to reflect research evidence; however, we acknowledge that pregnancy care is also provided to transgender and gender diverse people. Engaging with partners and families of pregnant women to support changes to health behaviours is important, as is consideration of the partner’s health during the preconception period. These issues could not be covered within the scope of this article; however, they should be taken into account when providing care to women. Care provision to pregnant women who use e-cigarettes also requires consideration. As evidence and best practice recommendations become available in this emerging space, specific guidance to general practice will need to be provided.
Conclusion
GPs play an important role in proactively providing care for women during the preconception, antenatal and postnatal periods. Provision of best practice assessment and care addressing smoking, alcohol and weight can reduce risks and optimise health outcomes for women and their babies. MT
COMPETING INTERESTS: Dr Kingsland has received salary support from the Australian Prevention Partnership Centre and the Hunter New England Local Health District; financial and travel support from the NHMRC and the Hunter New England Local Health District; and has been a member of the Population Health Program Executive Committee, Hunter Medical Research Institute. Dr Hollis has received salary support from the Hunter New England Local Health District, Hunter Medical Research Institute, and Australian Government Department of Education and Training; travel support from Hunter Medical Research Institute, Hunter New England Local Health District and Australian and New Zealand Obesity Society; and has been a member of Hunter Medical Research Institute. Dr Daly has received salary support from the Hunter New England Local Health District. Professor Elliott has received funding from government and competitive sources relating to research into alcohol use in pregnancy and fetal alcohol spectrum disorder (FASD), including for the FASD Hub, FASD Register and FASD Clinic; and salary support from a Medical Research Futures Fund Next Generation Fellowship; and is Chair of the National FASD Advisory Group and a Board Member of the National Organisation for FASD.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.