Conducting a CPAP review appointment – timing, tips and troubleshooting

Obstructive sleep apnoea (OSA) is a common chronic disease and continuous positive airway pressure (CPAP) is the gold standard treatment for most symptomatic patients. However, nearly half of patients starting CPAP will have side effects in the first few weeks of therapy. Early troubleshooting and motivational support increases treatment adherence and hence long-term benefits of CPAP therapy.
- Continuous positive airway pressure (CPAP) is an evidence-based treatment for obstructive sleep apnoea (OSA).
- To have significant treatment benefits, CPAP usage should be four hours or more per night.
- Poor experience with CPAP in the first two months predicts subtherapeutic long-term usage.
- People of disadvantaged backgrounds and current smokers are at high risk of nonadherence with CPAP.
- Daily mask cleaning can reduce side effects, such as poor mask seal, dry mouth and dry eyes.
- Sleep specialist referral is indicated for patients who have not responded after two months on CPAP therapy.
If you think you are seeing more obstructive sleep apnoea (OSA) in your clinic than ever before, you are not wrong. OSA is a common chronic disease, occurring in more than 10% of men in Australia aged 45 to 64 years.1 The prevalence has increased dramatically in Western countries, with a 14% increase in incident cases from 1988–94 to 2007–10.2
The system under Medicare of investigating patients with suspected OSA and starting treatment has changed radically since 2018. A guide to arranging diagnostic sleep studies and choosing appropriate treatment(s) is covered in the Medicine Today article ‘Obstructive sleep apnoea: navigating the system’, published in the December 2021 issue of the journal.3
The gold standard treatment for most patients with moderate or severe symptomatic OSA is continuous positive airway pressure (CPAP) treatment. Given the management of OSA is increasingly becoming the domain of primary care, this article aims to develop the skills necessary to conduct a timely CPAP review appointment, identify patients at risk for CPAP nonadherence early and apply CPAP troubleshooting strategies.
Consequences of untreated OSA
Untreated OSA is associated with excessive daytime sleepiness, resulting in reduced workplace performance, increased motor vehicle crash risk and poor mental health.4 Severe OSA is associated with increased cardiovascular disease, including systemic hypertension, pulmonary hypertension, coronary artery disease, cardiac arrhythmias, heart failure and stroke.5 OSA is estimated in Australia to cost $2.6 billion annually through associations with cardiovascular disease, malignancy, lost productivity, absenteeism and mortality.1
Importance of adherence to CPAP treatment
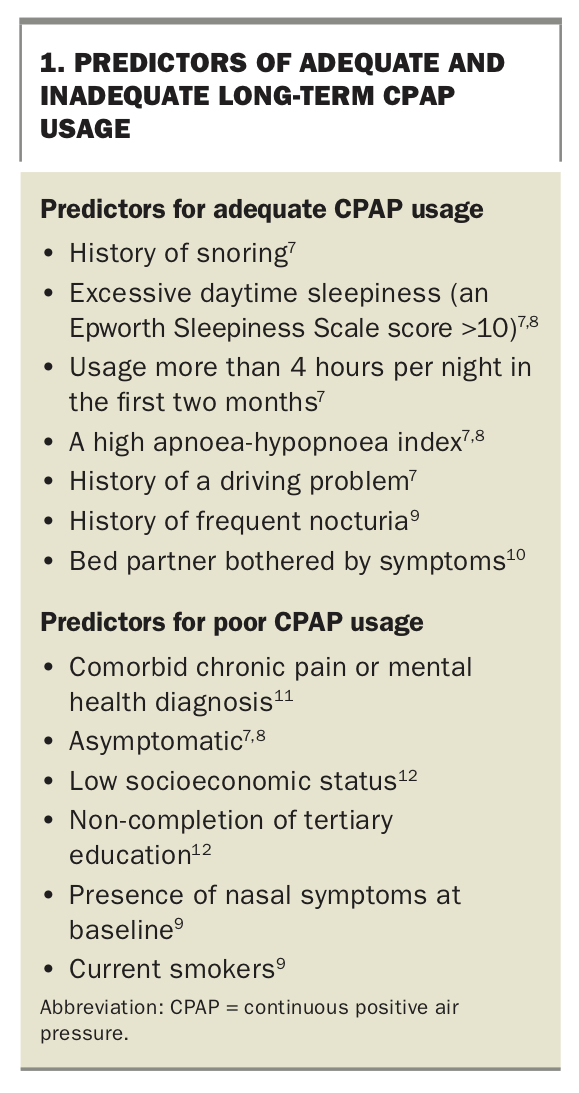
Fortunately for those with symptomatic OSA, CPAP is a highly evidence-based treatment.4 As with many chronic diseases however, adherence to treatment is the key to long-term benefit. Only around 40% of patients achieve four hours or more per night on their CPAP machine, although this does range from as low as 20% without assistance to as high as 80% with structured support.5 Those with severe OSA need to use CPAP for more than six hours per night to normalise their respiration.6 Patients who use CPAP for less than four hours per night are unlikely to achieve the neurocognitive improvements associated with adequate CPAP use.5 Predictors of CPAP usage adequacy are listed in Box 1.7-12
{kind=link}
Interestingly, age, gender and nadir oxygen saturation, which might be intuitively expected to impact CPAP usage, do not feature as independent predictors of adherence. Psychological factors do, however, play a significant role. These factors include:
- poor coping self-efficacy and confidence in CPAP use
- high perception of, and focus on, difficulties with treatment
- low expectation of benefit in daily functioning, health and wellbeing with CPAP use
- low perceived disease severity (functional impact of sleepiness) – people with this factor would be those ‘dragged in’ by their bed-partner but who do not think anything is wrong.
Improvements from CPAP
Improvements that can be expected after starting and adhering to CPAP include:
- normalisation of the apnoea-hypopnoea index (AHI), resulting in normalisation of nocturnal oxygen saturation13
- less daytime sleepiness
- improved neurocognitive performance
- improved cognition in those with mild cognitive impairment and severe OSA14
- improved driving performance15
- improved overall quality of life and reduced anxiety and depression symptoms.16
Assessing whether CPAP therapy can modify cardiovascular outcomes is more complicated. Two recent large studies showed patients with OSA and a history of a cardiovascular event, there was no significant reduction in death from cardiovascular disease with CPAP therapy.16,17 However, the patients enrolled in these studies had subtherapeutic CPAP usage (about three hours per night). Many surrogates of cardiovascular disease have been shown to improve with CPAP, including blood pressure control, left ventricular ejection fraction, nocturnal arrhythmias and urinary catecholamines.16 It is unlikely that a study with sham CPAP will be undertaken in symptomatic OSA patients to clarify this further.
CPAP equipment and care
Positive airway device options
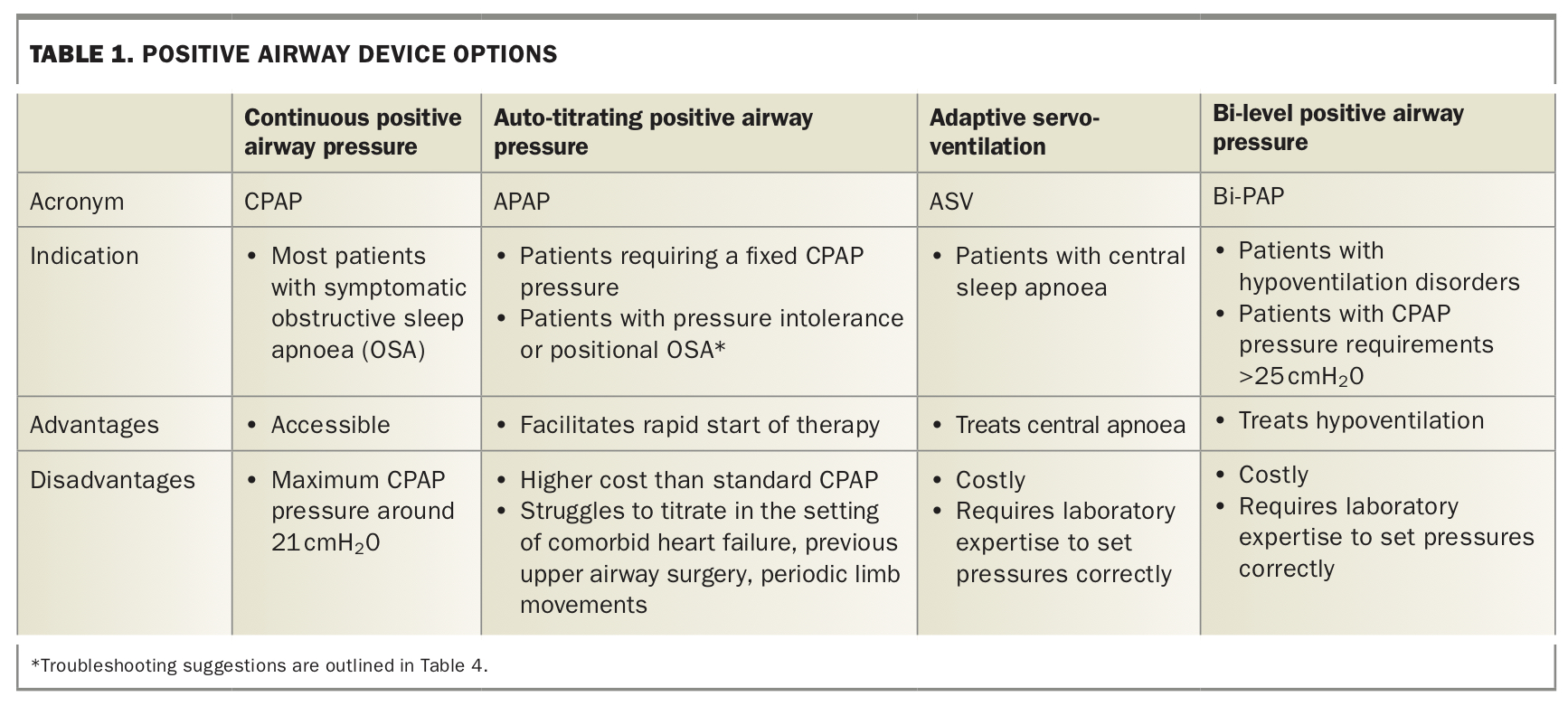
The CPAP machine is a small bedside pump connected to the upper airway via a mask attached to the patient’s face, splinting the airway open. Auto-titrating positive airway pressure (APAP) is a form of CPAP in which the device contains sensors to increase and decrease the pressure to maintain a patent airway. Most patients do not need the more expensive APAP devices in the long term, as evidence does not show APAP improves adherence or outcomes. Bi-level positive airway pressure (also known as Bilevel, VPAP, BiPAP®, BPAP) machines alternate between inspiratory and expiratory pressure (IPAP, EPAP); these machines are indicated for hypoventilation disorders or where the pressure required to treat OSA is above the upper limit of a standard CPAP machine (usually >25 cmH2O). Adaptive servo-ventilation (ASV) ventilators have proprietary algorithms that track a patient’s breathing pattern and then deliver a targeted ventilation to normalise respiration, using clinician-set inspiratory and expiratory pressure ranges. The indications for, and advantages and disadvantages of, the various positive airway device options are summarised in Table 1.
{kind=link}
Types of masks
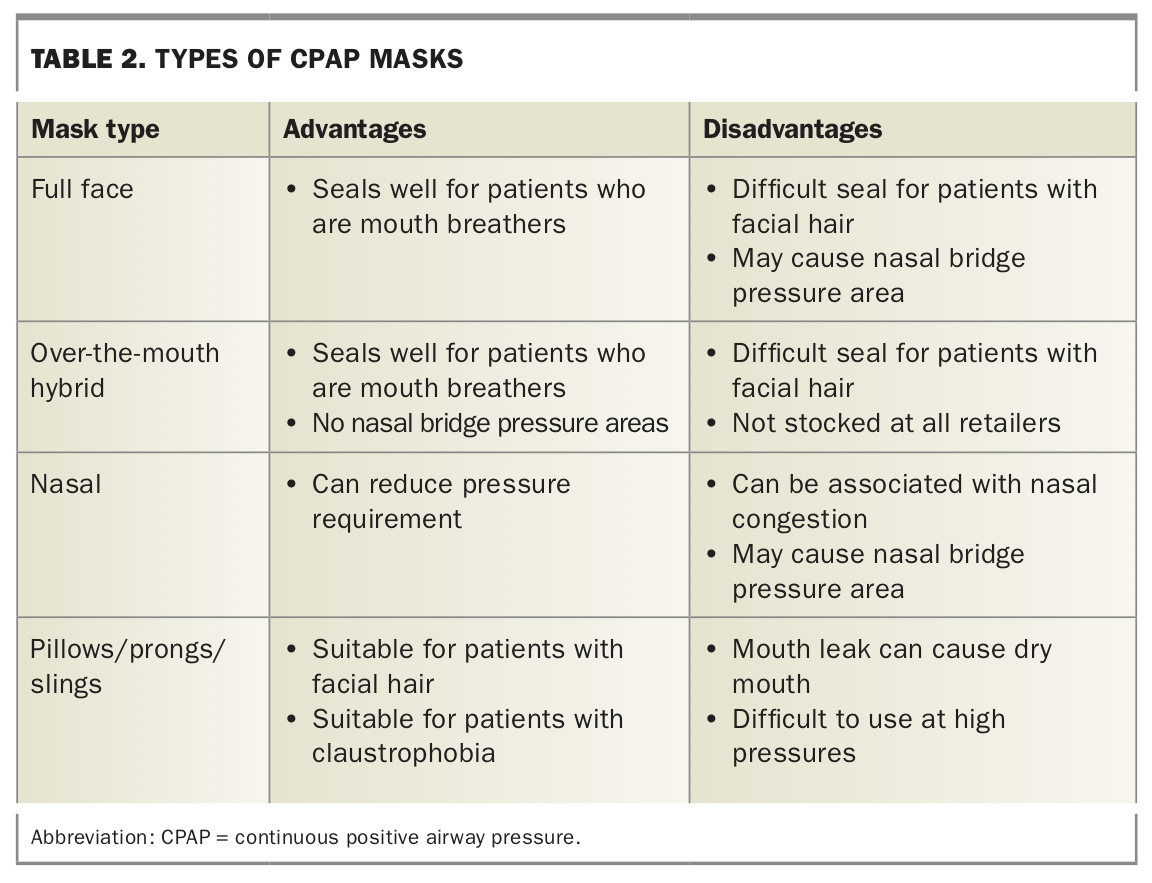
There are four main options for masks: full-face (oronasal) masks, over-the-mouth hybrid masks (which sit under the nose), nasal masks and nasal pillows/prongs/slings. The advantages and disadvantages of these different mask types are listed in Table 2.
{kind=link}
Routine mask care
A clean mask seals better and reduces the likelihood of leaks, side effects and discomfort. Regular mask cleaning will also improve the longevity of the equipment. Patients should expect to replace headgear and mask cushions about every 12 months, and the whole mask about every three years. Some tips for mask cleaning include:
- mask cushion
– wash daily with warm soapy water and place to dry
– do not leave out in direct sun
– do not bleach - mask headgear
– wash weekly with laundry detergent and hang to dry in the shade
– hand washing is best
– if washing in a machine, put in a pillow case or ‘delicates’ bag - mask frame
– wash weekly with warm soapy water and place to dry.
The CPAP review appointment
Follow up at two, six and 12 months after diagnosis of OSA is suggested to discuss symptoms, as well as CPAP usage and side effects. Daytime sleepiness can be recorded using the Epworth Sleepiness Scale (ESS; https://epworthsleepinessscale.com/about-the-ess/), a free, validated, self-report tool to quantify excessive daytime sleepiness. The ESS is a summation of eight items, with a score above 10 considered higher than normal daytime sleepiness, and a score 16 and above indicative of severe excessive daytime sleepiness.18
The main items to cover in a CPAP review appointment include the following.
- Review of symptoms:
– aim for an ESS score of 10 or less (normal)
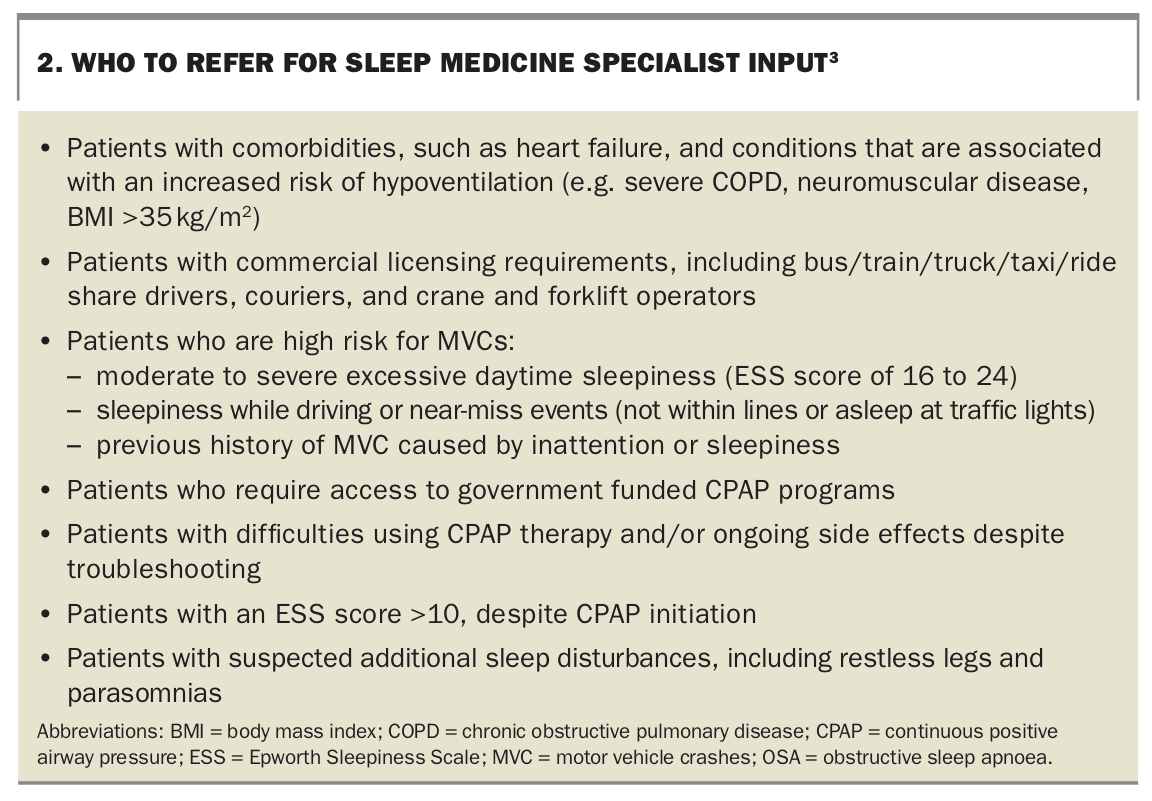
– refer patients not achieving the above symptomatic response to a sleep medicine specialist for review, as outlined in Box 2.3 - Review of driving safety:
– aim for no inattention with driving and no microsleep episodes. - Review of a download of the patient’s CPAP machine (obtain this from their CPAP provider):
– check usage – aim for usage of more than four hours per night
– review efficacy – aim for machine-derived ‘AHI’ of less than five events per hour
– review mask seal – aim for mask leak of less than 25 L per minute. - Discussion of side effects, as summarised later in this article.
{kind=link}
When to arrange a repeat CPAP titration study
There are only a few indications for repeat CPAP titration studies for patients established on therapy; routine annual re-titration is not recommended. Indications for repeating a CPAP titration study include:
- significant weight change (greater than 10 kg up or down)
- return of symptoms
- unresolved side effects
- significant change in comorbidities, e.g. heart failure or increased opiate dosage
- other associated problems, including restlessness, awakenings, restless legs and/or insomnia.
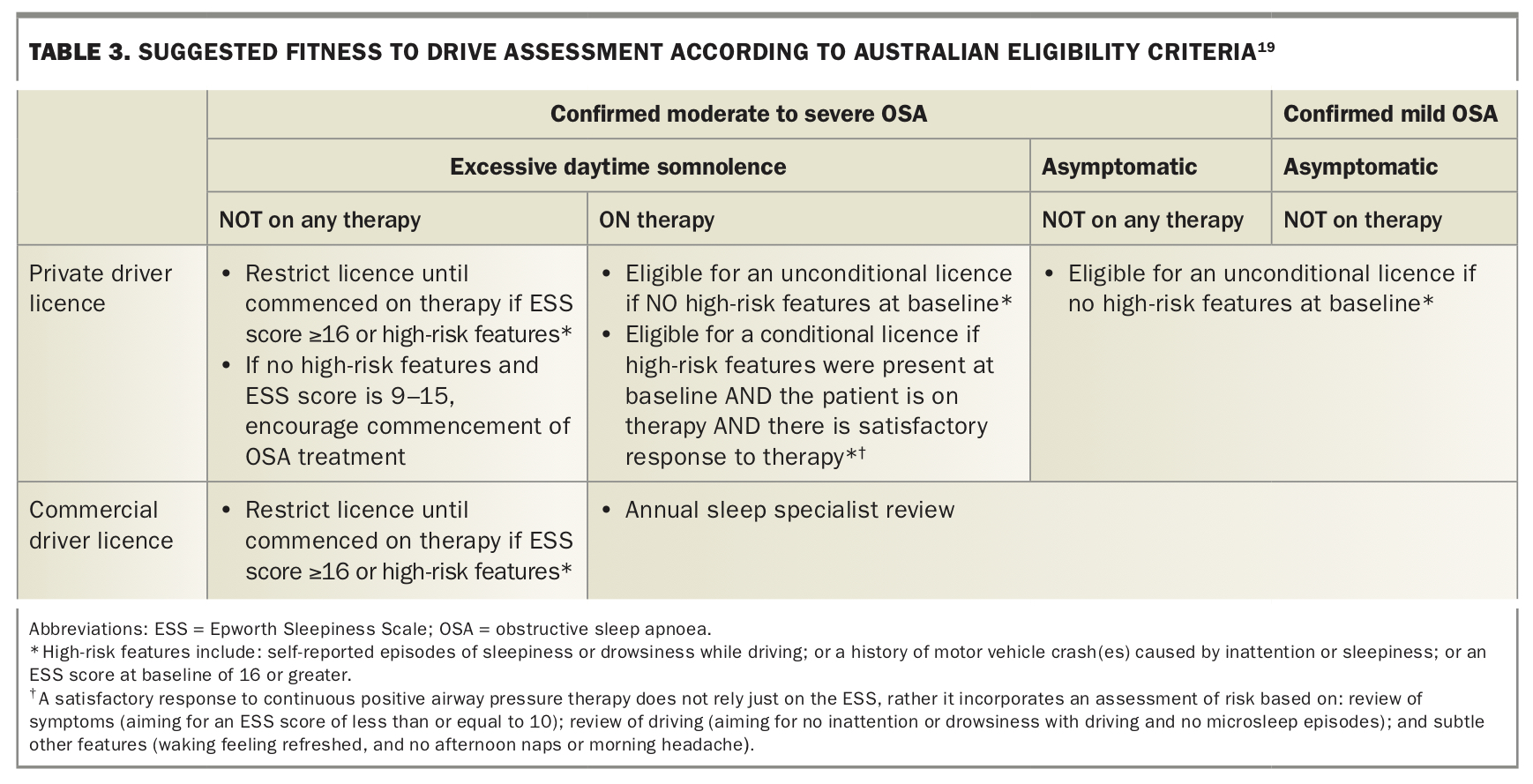
Assessing fitness to drive
Fitness to drive is an important safety and medicolegal consideration with OSA. The current Australian guidelines for assessing fitness to drive outline the conditions under which a patient with OSA can be considered safe and fit to hold a driver licence.19 Table 3 summarises the eligibility criteria for private and commercial driver licences according to OSA severity and whether the patient is undergoing treatment.19 Sleep physicians recommend that patients with confirmed moderate to severe OSA require adherence of more than four hours per night of CPAP and symptomatic response to be fit to drive.
{kind=link}
Patients with OSA should be made aware of their legal obligation to notify their local transport licensing authority and insurance provider of their diagnosis. Driving restrictions should be customised to consider the degree of sleepiness risk and the nature of the driving tasks. For example, restrictions while awaiting therapy may include limiting driving duration to 30 minutes at a time and limiting driving to daytime only.
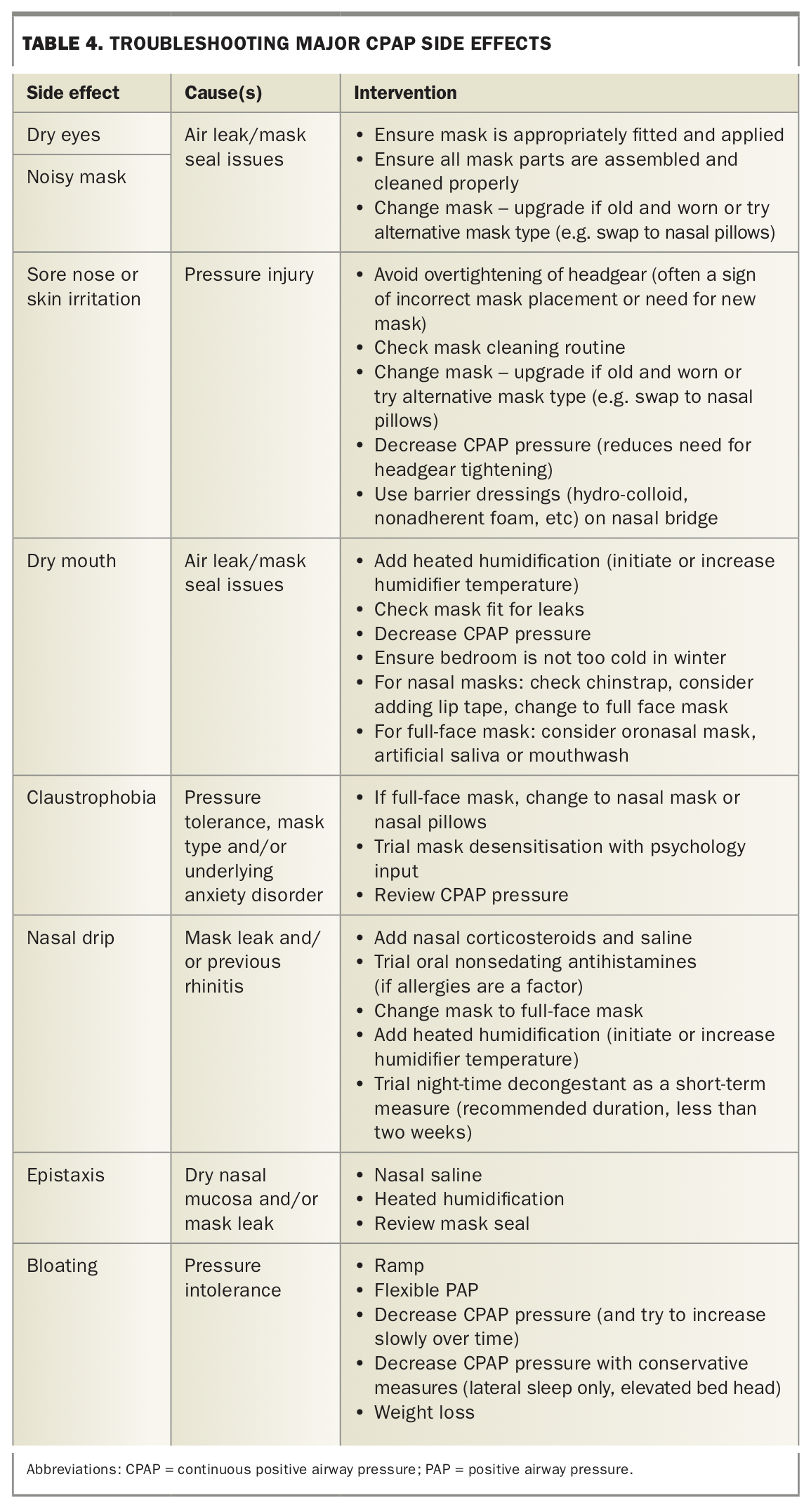
Troubleshooting the major side effects of CPAP
About half of people starting CPAP will have at least one side effect. Troubleshooting these side effects early in the first two to three months of CPAP use increases the probability of long-term adequate adherence. Three common device-specific comfort features can be customised to improve adherence and comfort for patients: ramp, proprietary flexible pressure settings and humidification.
Ramp
In the ramp option, the pressure starts at a pre-set level (usually a low level of CPAP, such as 4 cmH2O) and then slowly increases to the treatment pressure (CPAP) over the set ramp time. This setting is usually adjusted up or down by CPAP providers if the patients feel pressure onset is too fast/strong initially or insufficient.
Proprietary flexible pressure settings
These proprietary expiratory pressure relief settings, known as A-Flex, C-Flex and EPR, depending on the brand, allow for the pressure to be adjusted by the machine by about ±1 to 3 cmH2O to facilitate greater flow in exhalation.
Humidification
Heated humidity increases the moisture to reduce the discomfort of oronasal mucosal dryness. Humidity can be altered up (usually needed in winter) or down (usually in summer, especially in tropical areas). Overall, studies indicate increased compliance with humidifiers. However, there are increased cleaning demands with a humidifier, including the issue of water condensing in the tubing and mask. This can be avoided by keeping the CPAP unit on the ground by the bedside, purchasing tubing with inbuilt heating elements and purchasing a tubing cover.
Motivational techniques to improve CPAP adherence
Several evidence-based motivational interviewing techniques can be used to help patients use CPAP. These include the following:
- consider the primary motivators for each patient separately – often it is not longer-term health outcomes, but rather improved energy, reduced irritability and improved capacity to engage in social relationships that motivates patients
- focus on the primary motivator(s) for change with CPAP education, in addition to answering technical questions
- pay attention to ‘change talk’ (statements indicating a willingness to try to engage with treatment) and reflect these back to the patient during the consultation
- ‘roll with resistance’ – if patients express concerns about CPAP use, acknowledge this and explore concerns openly and nonjudgementally
- develop a clear plan for managing any concerns or barriers to use, e.g. discomfort, noise and/or cost; suggested strategies for managing side effects of CPAP are listed in Table 4
- foster self-confidence by supporting the patient to maintain a problem-solving and open attitude to treatment
- encourage patients to call their CPAP stockist or sleep laboratory early for help with problem solving any issues that arise, rather than discontinuing treatment prematurely
- at follow up, reflect on the benefits that the patient has obtained through treatment, particularly in reference to their original motivators for change
- at follow up, reinforce machine maintenance (such as air filter and mask cleaning) to reduce side effects
- at follow up, reinforce any attempts to problem solve or seek support on any difficulties arising with the treatment.
{kind=link}
Breaking news - product recall
In 2021, the Therapeutic Goods Administration (TGA) announced that Philips Australia and New Zealand had to issue an urgent product defect correction for sleep and respiratory devices, because of issues with sound abatement foam used inside certain CPAP and Bilevel PAP devices. Concerns were raised that the foam may degrade and be ingested or inhaled by the users.
This is an evolving situation, and the most up-to-date information can be found at the Philips website for Sleep and Respiratory Care (https://www.philips.com.au/healthcare/e/sleep/communications/src-update). Patients with Philips Respironics branded CPAP machines should be advised to:
- register their device with the manufacturer via this website https://www.philipssrcupdate.expertinquiry.com/?ulang=en or by phoning 1800 009 579 (toll-free)
- go to their local CPAP provider to obtain an inline bacterial filter
- continue using therapy unless OSA is mild and symptoms pre-treatment were mild. The benefits of continuing CPAP therapy for most patients outweigh the risks raised by the product defect.
By registering a device of concern, patients should gain assistance from Philips to have their machines corrected under the repair/replacement program. The TGA notes that 20% of machines have been corrected in Australia since the notification in early 2021.
Conclusion
Early troubleshooting and motivational support increases the probability that patients with OSA will gain the benefits of CPAP therapy. These benefits include less daytime sleepiness and workplace absenteeism, fewer motor vehicle crashes and improved quality of life.
Patients will frequently turn to their GP for first-line assistance with CPAP issues, so awareness of common side effects and potential strategies to work through these will improve therapy adherence. Mask cleaning is the key to a good mask seal, which reduces side effects such as dry mouth and dry eyes. If somnolence is not improving after two months of CPAP, specialist input can help with reviewing pressure requirements, mask review and additional support.
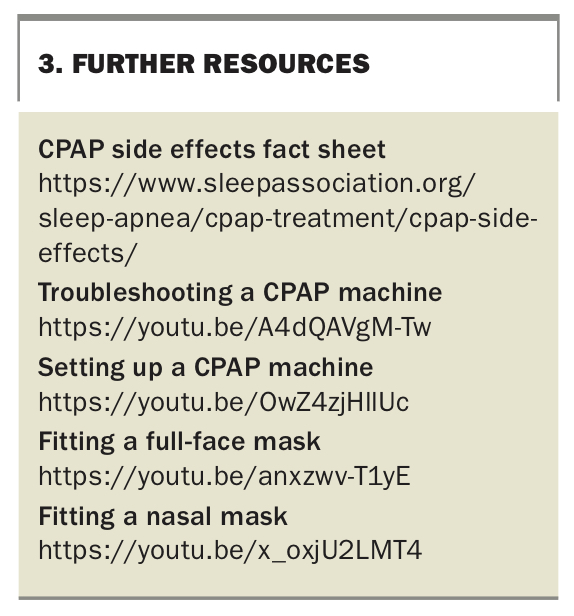
Further resources that may be useful are listed in Box 3. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.