Obstructive sleep apnoea – navigating the system

Dr Ellender is a Respiratory and Sleep Physician at the Princess Alexandra Hospital, Metro South Hospital and Health Service, Brisbane; and Senior Lecturer at the Faculty of Medicine, Princess Alexandra Southside Clinical Unit, University of Queensland, Brisbane.
Dr Jones is a General Practitioner at Eastbound Medical Clinic, Bentleigh East, Melbourne, Vic.
Dr Hukins is a Respiratory and Sleep Physician at the Princess Alexandra Hospital, Metro South Hospital and Health Service, Brisbane; and Associate Professor at the Faculty of Medicine, Princess Alexandra Southside Clinical Unit, University of Queensland, Brisbane, Qld.
Sleep apnoea

Obstructive sleep apnoea (OSA) is becoming increasingly prevalent in our communities. GPs are well placed to recognise, investigate and manage many patients with uncomplicated OSA. Navigating the system to help patients access diagnostic sleep studies and appropriate treatment can be difficult. This article aims to demystify the system and help facilitate timely treatment.
- Obstructive sleep apnoea (OSA) is a common chronic disease and is increasing in prevalence.
- A focused history is important to evaluate for the likelihood of OSA and to identify patients at risk of the consequences of untreated OSA.
- A sleep study is needed to confirm the diagnosis and evaluate the severity of disease.
- Continuous positive airway pressure (CPAP) therapy is the gold standard for many symptomatic patients with moderate to severe OSA.
- Other treatment options are available for less severe disease or for those with difficulties in using CPAP.
All GPs will have seen patients dragged in by their bed partner with fatigue, loud snoring and excessive daytime sleepiness and suspected obstructive sleep apnoea (OSA) to be the likely diagnosis. OSA is a sleep disorder characterised by obstruction or collapse of the upper airway during sleep, resulting in oxygen desaturation and sleep fragmentation. It is the most common cause of excessive daytime sleepiness, unrefreshing sleep and snoring, and a cause of reduced workplace productivity.
OSA is increasing in prevalence in Australia due to increasing obesity.1 It is a very treatable disease, often with continuous positive airway pressure (CPAP) therapy. However, navigating the system from symptoms to treatment requires a customised approach to match the patient with the correct testing modality and treatment.
With the increase in prevalence of OSA, management of OSA is increasingly becoming the domain of primary care. This article aims to demystify the system and help facilitate timely treatment, to help our patients feel less sleepy, more productive and have lower motor vehicle accident risk. Patients without significant comorbidities and a history consistent with OSA are suitable for GP-referred sleep studies and can be initiated on therapy in the community with follow up at the primary care level. This article will cover the specific comorbidities and history to look for to stratify patients into those who can be managed in primary care and those who require in-laboratory studies and sleep physician review.
Consequences of untreated OSA
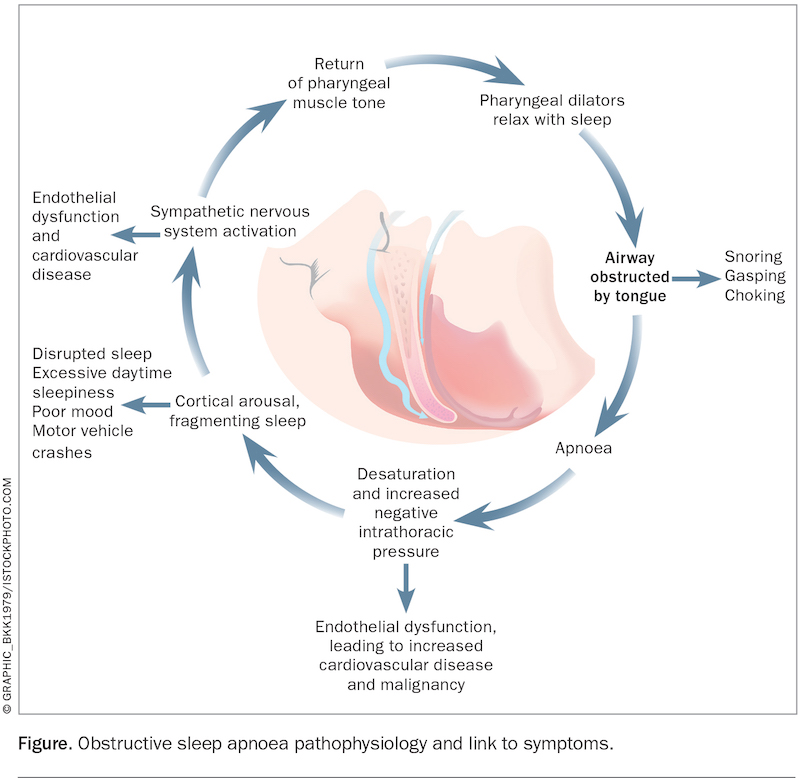
The pathophysiology of OSA is shown in the Figure. Untreated severe OSA is associated with a fourfold increase in all-cause mortality and increased cardiovascular disease, such as ischaemic stroke, myocardial infarction, hypertension and arrhythmia.2
{kind=link}
Severe OSA is also associated with a sevenfold increased risk for multiple vehicle crashes in a five-year period, independent of age and driving time.3,4 It is essential to ask about driving safety when taking a sleep history – falling asleep at the traffic lights, near misses or inattention due to sleepiness and previous sleepiness-related accidents are predictors of motor-vehicle accident risk.
Additionally, severe OSA is associated with a 25% increased relative risk for developing cancer, controlling for confounders.5
Epidemiology
Across all populations, at least 14% of men and 5% of women will have some of sort of OSA.6,7 OSA has been increasing in prevalence in recent years.8
Data from the Bettering the Evaluation and Care of Health (BEACH) program has shown that sleep disturbance is within the top 30 reasons for attendance in general practice.9
Risk factors
The common risk factors for OSA are age greater than 65 years, obesity, male sex and anatomical features such as retrognathia.3 Obese adults (body mass index [BMI] greater than 30 kg/m2) have as high as a 45% risk of OSA, compared with a 25% risk in those who are overweight (BMI 25 to 29.9 kg/m2).10 There is a strong association between OSA and other chronic diseases such as heart failure and end-stage kidney disease.
Presenting features and their assessment
The key presenting features of OSA are listed in Box 1. A history of excessive daytime sleepiness and nocturnal choking or gasping is the most predictive for a diagnosis of OSA. Although some patients will present with nocturnal symptoms of snoring, a history of nonrestorative sleep, morning headaches and need for an afternoon nap can also point to this diagnosis.
{kind=link}
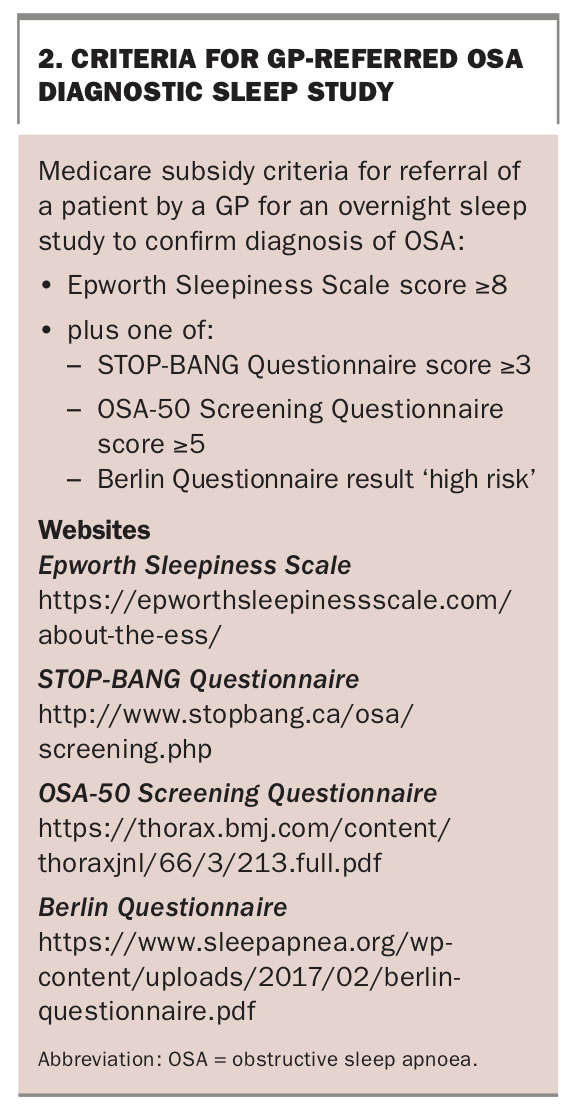
The most widely validated self-report tool to quantify excessive daytime sleepiness is the Epworth Sleepiness Scale.11 The scale is a summation of eight items, with a score above nine considered higher than normal daytime sleepiness and greater than 16 suggestive of severe excessive daytime sleepiness. The STOP-BANG, OSA-50 and Berlin questionnaires are validated screening tools for sleep apnoea.12-14 Significant results with these tools are a score of 3 or higher for the STOP-BANG questionnaire, a score of 5 or higher for the OSA-50 questionnaire and a ‘high risk’ result for the Berlin questionnaire.
An approach to the primary care investigation and treatment of a patient with OSA is shown in the Flowchart.
Investigating patients suspected to have OSA
In a patient with symptoms suggestive of OSA, a sleep study (polysomnogram) is needed to make a formal diagnosis. A sleep study involves measurement of electroencephalography (EEG) to confirm sleep stage, as well as measurement of chest and abdominal wall movement, nasal airflow and pressure, in addition to oxygen saturation, ECG and leg movements. Using data from the sleep study, OSA is categorised as mild, moderate or severe disease, based on the number of obstructive events per hour, known as the apnoea-hypopnoea index (AHI). An AHI of five to 14 events per hour indicates mild OSA, an AHI of 15 to 29 indicates moderate OSA and an AHI of greater than 29 indicates severe OSA.6
A Medicare subsidy is available for GP referral of patients for overnight sleep studies to confirm the diagnosis of OSA, providing certain criteria are met (Box 2).
{kind=link}
At-home sleep studies versus in-laboratory sleep studies
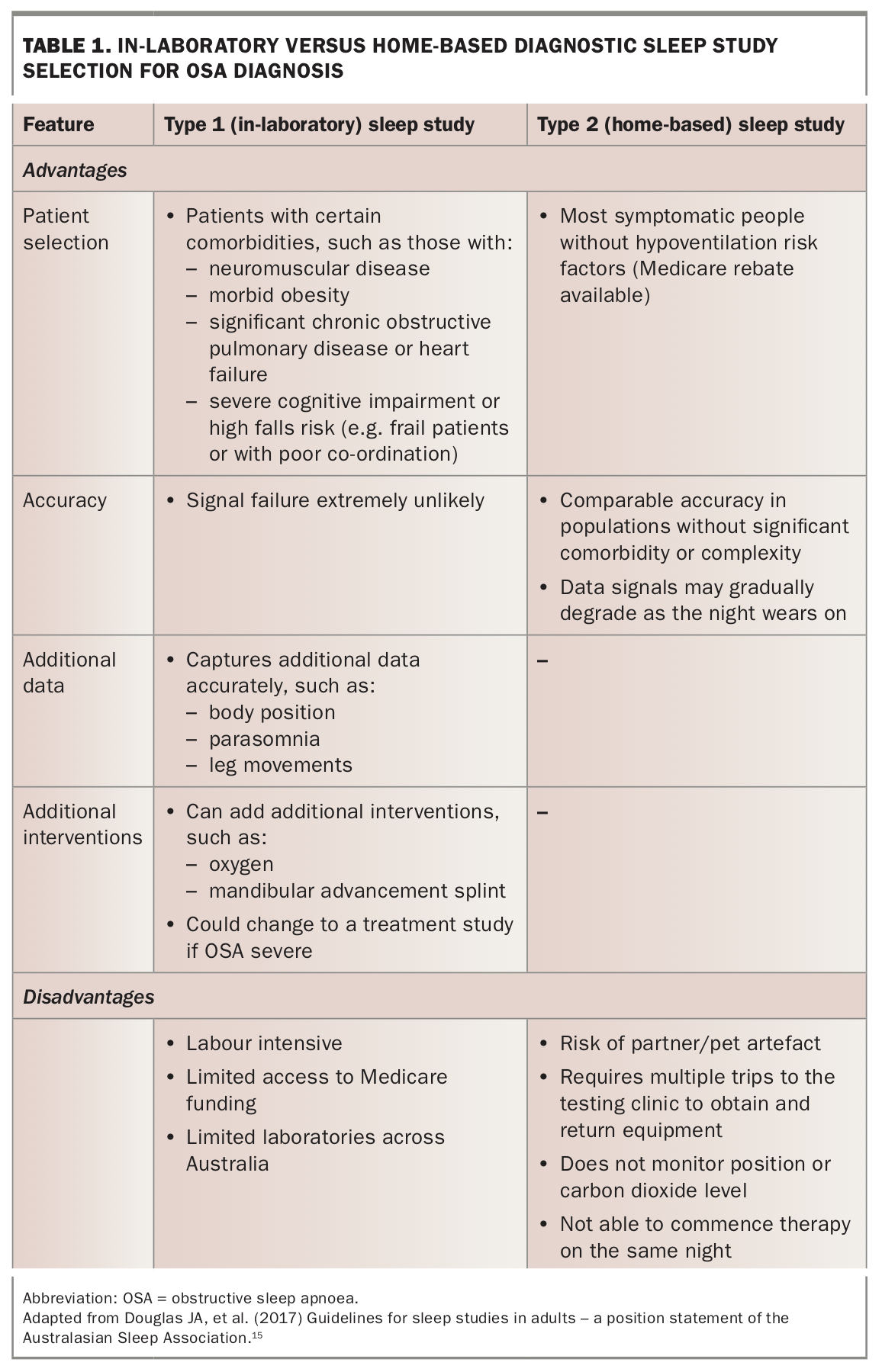
Most patients being investigated for OSA will be suitable for an unattended ‘type 2’ home-based sleep study (sometime also referred to as a ‘level 2 study’). Home-based studies can be used to confirm the diagnosis of OSA in patients with a highly suspicious history. However, because of the reduced data-set compared with laboratory testing, home sleep studies are not usually appropriate for investigating other sleep disorders, such as parasomnia, narcolepsy, nocturnal seizures or suspected hypoventilation disorders.
Attended in-laboratory diagnostic sleep studies (‘type 1 studies’) are needed where contraindications exist or for a second opinion, and require a sleep medicine practitioner or respiratory physician referral to be eligible for Medicare funding. Type 3 and 4 studies measure oxygen saturation and nasal airflow, without electroencephalography; these are not widely available, or Medicare subsidised. Table 1 summarises the indications, advantages and disadvantages of in-laboratory and home sleep studies.15
{kind=link}
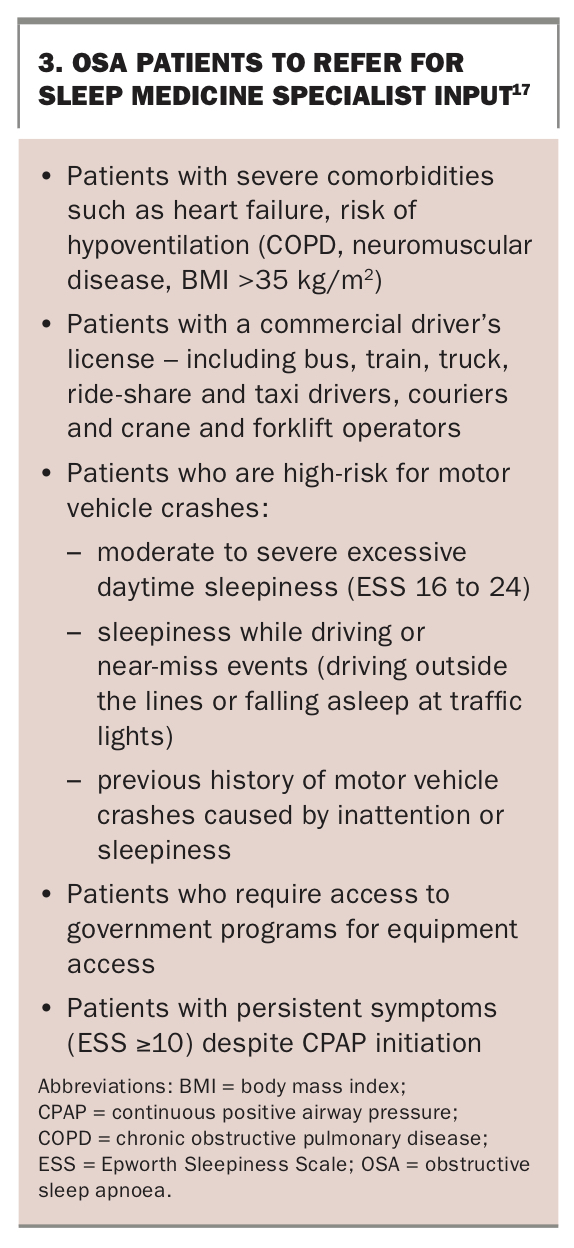
As shown in Box 2, in an adult with a suggestive history, who meets the Epworth Sleepiness Scale and other questionnaire criteria, GPs are the key healthcare providers for referring patients to get a Medicare subsidised ‘Type 2’ sleep study, providing there are no features that require a sleep physician review (Box 3). In-laboratory studies require a sleep physician review for the study to be Medicare subsidised. Box 3 summarises the patient groups who would benefit from input from a sleep medicine specialist.16
{kind=link}
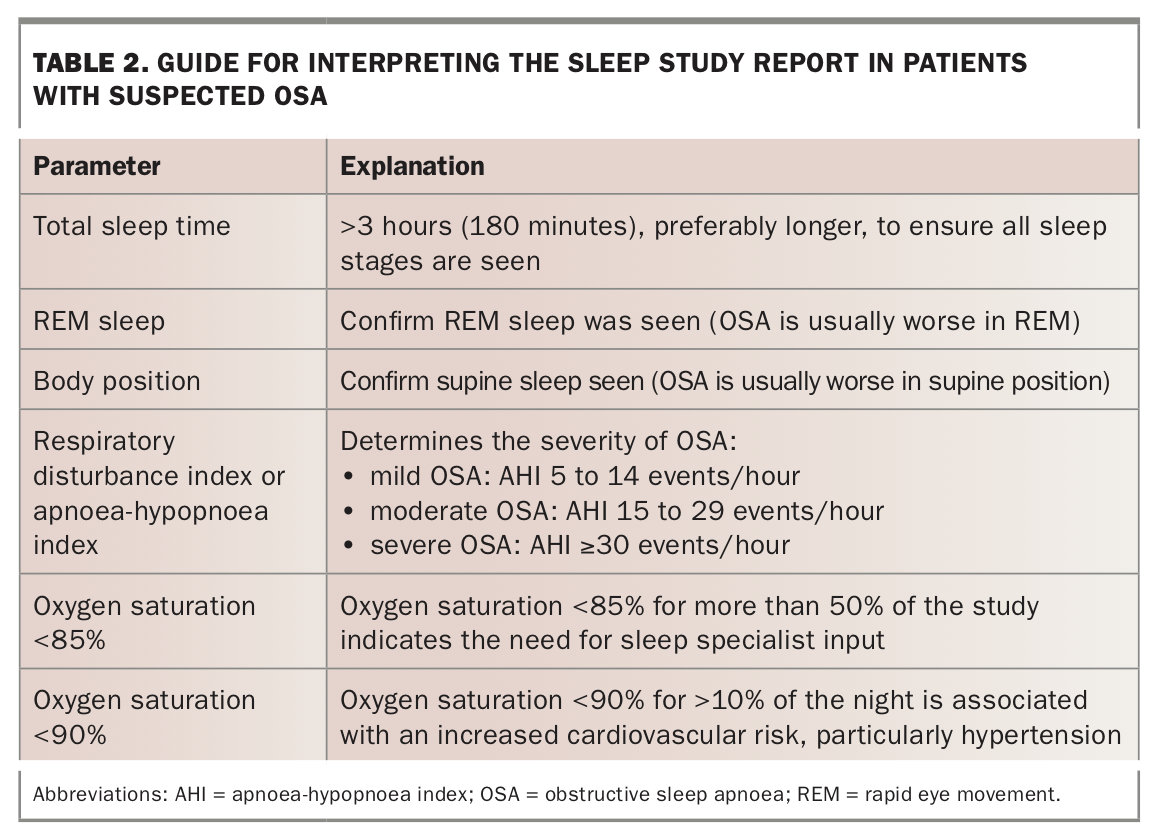
Key results from a sleep study
The key parameters to review in a sleep study report are summarised in Table 2. Building a relationship with local sleep study testing facilities is helpful for consistent results. To check which laboratories in your local area are accredited, see the National Association of Testing Authorities, Australia (NATA) website (www.nata.com.au/accredited-facility) and search by state using the keyword ‘sleep’.
{kind=link}
Treatment options for OSA
Unfortunately, OSA is a chronic disease that rarely resolves spontaneously. OSA treatment options include positive airway pressure (PAP), a mandibular advancement splint, surgery, positional therapy and weight loss.
CPAP
The gold standard treatment for OSA is CPAP. The CPAP machine is a small bedside pump connected to the patient’s upper airway via a mask attached to their face, splinting the airway open. Auto-titrating CPAP (APAP) is a form of CPAP delivered by a device that contains sensors to increase and decrease the pressure in order to maintain a patent airway. Most patients do not require auto-titrating CPAP machines; for more information see our follow-up article about CPAP therapy in a future issue of Medicine Today.
CPAP is indicated in symptomatic moderate to severe OSA, or mild OSA with an oxygen saturation (SpO2) less than 90% for greater than 10% of the night.
CPAP is a highly effective treatment for OSA. There is strong evidence that CPAP therapy for people with OSA improves the AHI and daytime sleepiness, reduces motor-vehicle accident risk, and increases quality of life.17 The number needed to treat to achieve a two-point reduction on the Epworth Sleepiness Scale is only four, with a cost to the healthcare system of only about $550 per person per year.1,18 Another advantage of CPAP therapy is that the CPAP machine can be rented to test for symptom improvement before purchase.
Disadvantages of CPAP therapy include side effects and the cost of the device and mask replacement. Side effects such as nasal congestion and dry mouth are common, and adherence to CPAP therapy of greater than four hours per night is required to obtain ongoing benefits.
Mandibular advancement splints
Mandibular advancement splints advance the lower jaw while the wearer sleeps. They are custom-made by a specialist dentist. The Australasian Sleep Association list of accredited sleep dental services can be found online in the Sleep Services Directory by selecting OSA – Dental Treatment and your location (www.sleep.org.au/public/resources/sleep-directory).
Mandibular advancement splints are indicated in mild to moderate OSA in the absence of significant oxygen desaturation and in patients who are intolerant of CPAP therapy.19
The advantages of mandibular advancement splints are that they are more portable than CPAP machines and they are associated with fewer nasal side effects than CPAP therapy. Their disadvantages include their cost, the potential long-term changes to the wearer’s bite and the requirement for adequate dentition. Mandibular advancement splints generally cost between $1200 and $2500 and full payment before use is usually required.
Surgery
Surgery as a treatment for OSA remains largely a last resort, and is only indicated in patients with mild symptomatic OSA where reversible risk factors (e.g. obesity) have been optimised, or for other OSA patients who cannot tolerate alternative therapies, following a sleep specialist opinion.16 The procedure involves debulking of the uvulae, palate and tongue with radiofrequency tissue ablation (known as a modified uvulopalatopharyngoplasty and coblation channelling of the tongue).
The advantage of surgery is that there is no ongoing requirement for device use; disadvantages include the risks of surgery and the limited longevity of efficacy as people age and gain weight.
Positional therapy
Positional therapy can be used for sleep apnoea where upper airway obstruction is present only in the supine position. Several forms of positional therapy are available, including vibro-tactile electronic devices, tennis balls sewn into a nightshirt and pillows with straps to prevent supine sleep. These are available for purchase through local CPAP retailers.
Positional therapy is indicated in mild to moderate OSA where there are infrequent events in the lateral position (e.g. lateral AHI less than 15 events per hour).
The advantage of positional therapy is that it has fewer side effects than other treatments; a disadvantage is that long-term adherence is poor.
Weight loss
Weight loss of more than 10% body weight can improve the severity of OSA; however, even surgical weight loss has been shown to result in persistent OSA in most patients.20 Thus, weight loss in isolation is not likely to be sufficient treatment for patients with moderate or severe OSA.
PAP treatment
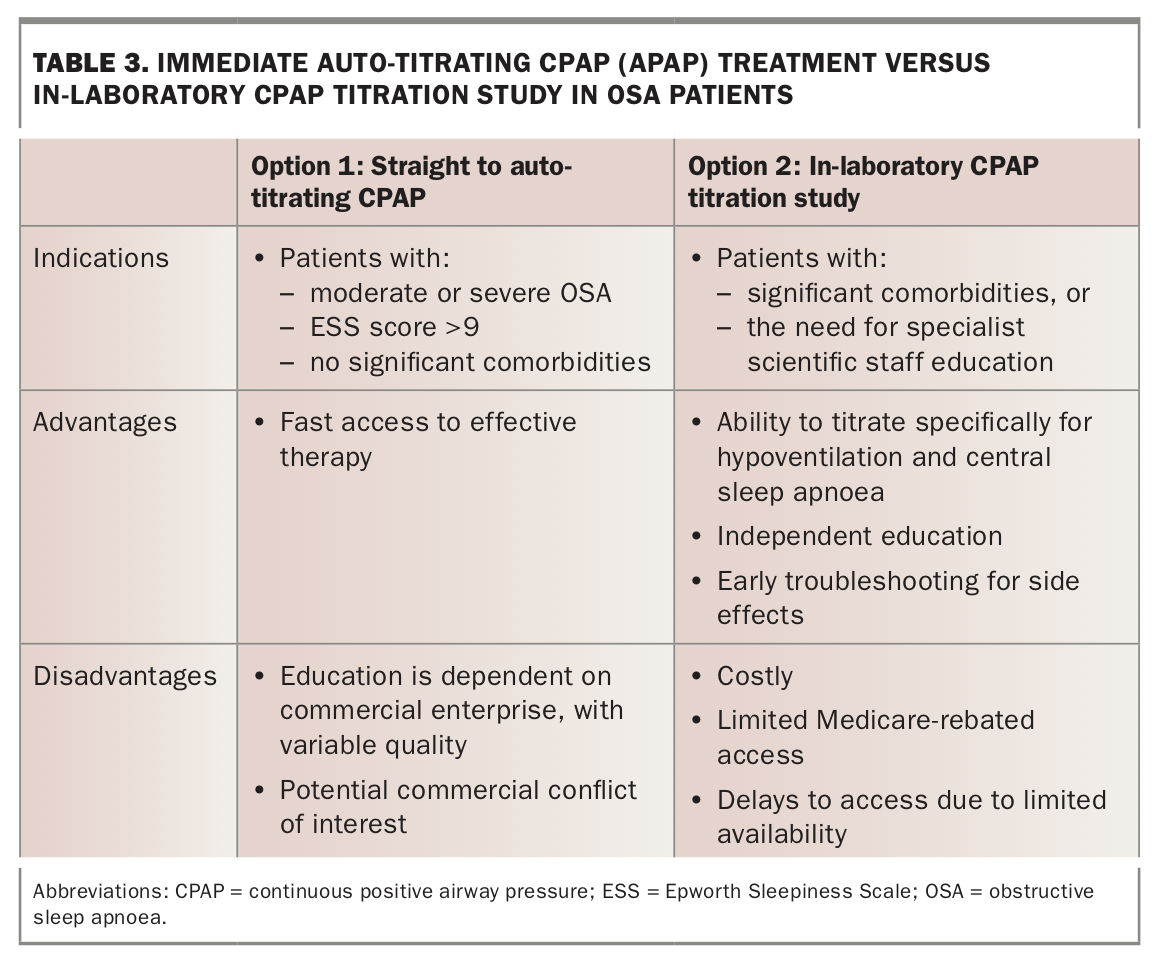
Accessing CPAP treatment
Following confirmation of the diagnosis of OSA, some patients can commence APAP treatment immediately and others will require in-laboratory CPAP titration (Table 3). This can be done by GPs in primary care, via local CPAP retailers and without a sleep physician consultation if the patient is able to self-fund therapy. See Table 3 for a guide to which patients are suitable for auto-titrating CPAP and which patients require in-laboratory CPAP titration studies.
{kind=link}
Patients are generally encouraged to rent an APAP machine for at least three nights and then rent a fixed pressure CPAP machine for two months prior to purchase of a CPAP machine to ensure tolerability. In most capital cities, rental of an APAP or CPAP machine costs about $100 to $200 each month. Masks cost about $120 to $300 and usually require replacement of head straps and silicon seals every 12 months.
After renting an APAP device, patients can either self-fund a CPAP machine, with settings titrated from the APAP findings, or can be referred to a local public sleep disorders unit to obtain a government-funded machine.
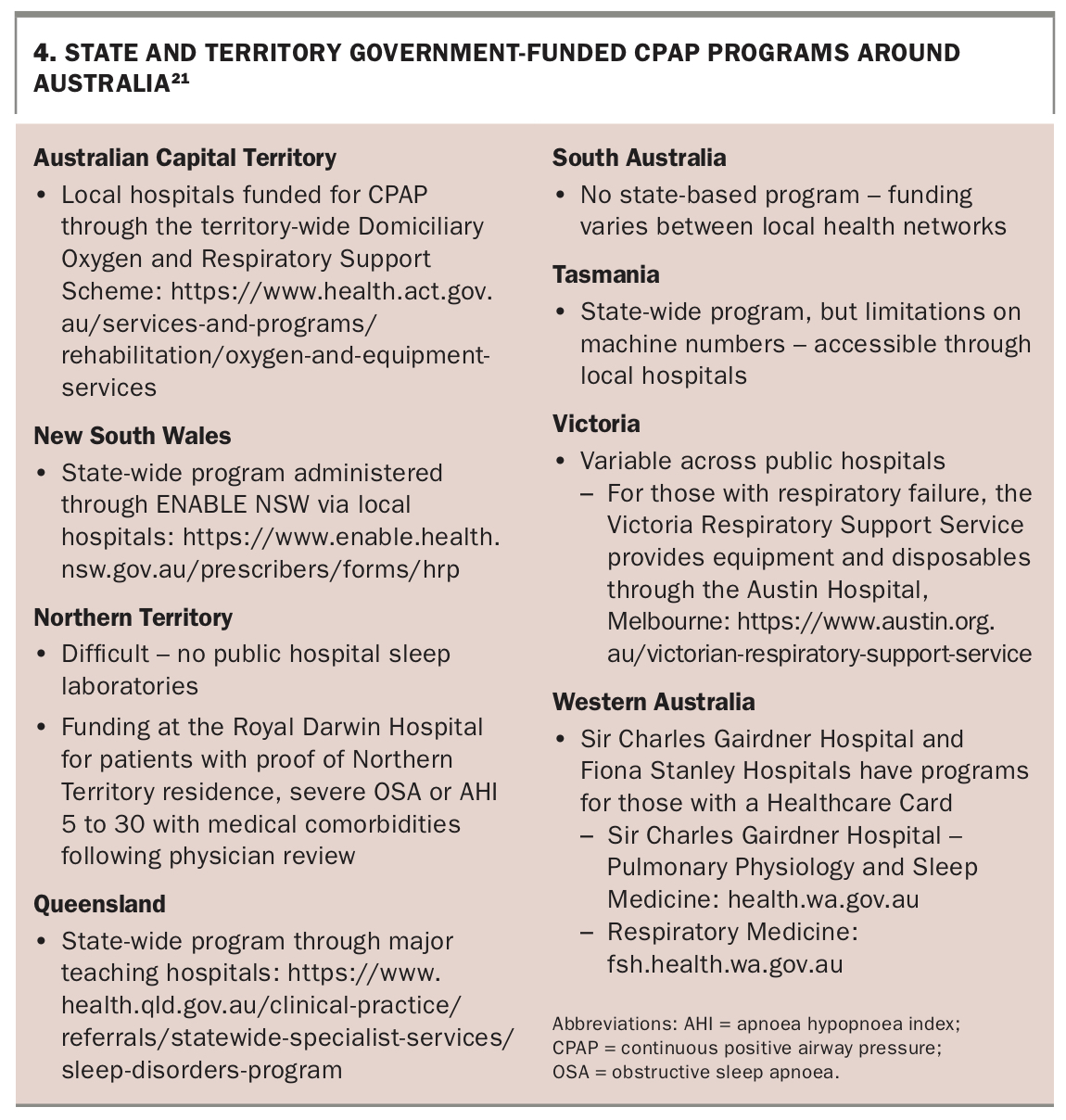
CPAP machines range in cost from around $750 to $2000, depending on the store and the type of device purchased. As a rough guide, however, most patients self-funding the machine should set aside $1500 in total for rental, mask and machine purchase. A machine will last eight to 15 years if cleaned regularly. Masks generally need replacing every three years if they are cleaned each morning. Funding is available in some states and territories for patients unable to self-fund CPAP equipment (Box 4).21
{kind=link}
Rebates
Private health insurance ‘extras’ will often reimburse around $500 of the initial cost of the equipment, depending on the policy; a supporting letter from a clinician may be required.
For those with financial hardship and no concession card, an application can be made to release superannuation for purchasing medical equipment. Forms can be found on the Australian Tax Office website (www.ato.gov.au; search for ‘Compassionate release of superannuation’).
Most electricity providers will provide a rebate and priority for restoring power in the event of supply issues. Concession or pension cardholders are eligible for an additional annual subsidy to Centrelink payments if an Essential Medical Equipment Payment Services Australia form is completed.
Government CPAP programs
Despite the strong data in support of CPAP, devices are not accessible through Medicare or Federal funding. There are several state-based programs for accessing government-funded CPAP machines for people with pension or concession cards. These programs generally require a referral to a designated centre and a rental period on CPAP to confirm adherence to treatment. Patients have to purchase their own masks.
Conclusion
OSA is a chronic disease with increasing prevalence in the community and can be effectively treated at relatively low cost. Its management is becoming the domain of primary care because of its increased prevalence. Navigating the system to initiate effective treatment for patients starts with a thorough history, recognition of indications for specialist referral, and knowledge of local services. High quality local sleep studies can expedite investigation and can be arranged by GPs where there are no red flags for specialist care. The conducting of a CPAP review appointment will be covered in our article on CPAP therapy in a future issue of Medicine Today. MT