COVID-19 manifestations in the skin
Skin changes are seen in up to 20% of patients with COVID-19 and vary widely in presentation. The most common include maculopapular eruptions, ‘COVID toes’, urticaria and most concerningly vaso-occlusive rashes, such as livedo reticularis and retiform purpura. Some of these skin signs are indicators of disease progression or severity.
- Skin changes are common in patients with COVID-19, seen in up to 20% of patients.
- Maculopapular eruptions and acral chilblain-like lesions are the most common skin changes seen in patients with COVID-19.
- Many skin changes have prognostic value and associations with severity of disease.
- Most skin changes do not need any specific treatment and resolve spontaneously over time.
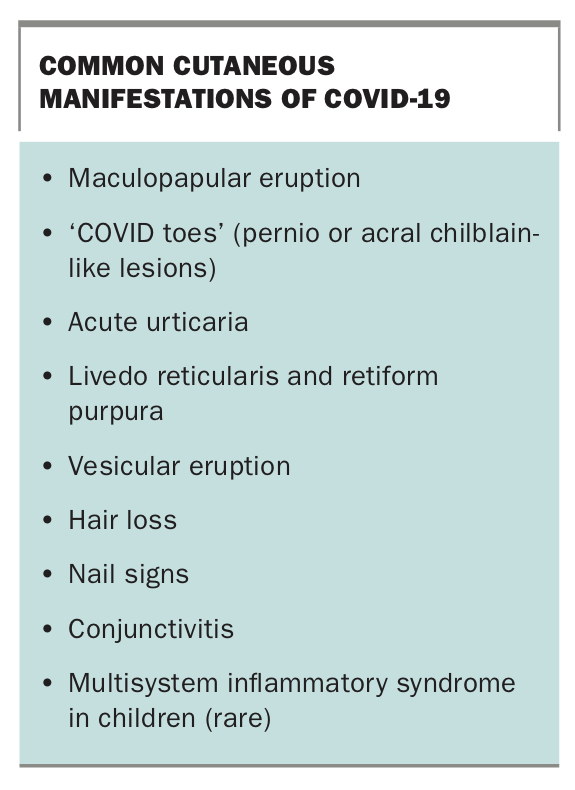
The global pandemic of coronavirus disease 2019 (COVID-19) has now lasted more than two years, and more than 400 million cases of COVID-19 have been reported worldwide.1 At the beginning of the pandemic, many different and unexpected skin changes were observed in association with COVID-19. It is now clear that skin changes occur in up to 20% of patients with COVID-19.2,3 We know which skin signs are more common and which are related to disease severity. The range of possible dermatological changes is broad, including maculopapular eruptions, ‘COVID toes’, urticaria, nail and hair changes and vaso-occlusive rashes (Box).
{kind=link}
This article reviews the most common skin changes associated with COVID-19, their course, relation with disease severity and management.
Incidence of COVID-19 skin manifestations
The online COVID-19 Dermatology Registry collates data about dermatological manifestations of COVID-19 on behalf of the American Academy of Dermatology and the International League of Dermatologic Societies. Any healthcare professional internationally is invited to contribute to the registry (www.aad.org/member/practice/coronavirus/registry).
The skin manifestations of COVID-19 most commonly reported to the Registry are:3,4
- maculopapular eruptions (22% of reported dermatological cases)
- chilblain-like or pernio-like acral lesions (18%)
- urticaria (16%)
- macular erythema (13%)
- papulosquamous eruptions (9%)
- retiform purpura (6%).
In addition, COVID-19 has been associated with erythema multiforme, conjunctivitis, oral mucosal ulceration, petechiae, chronic urticaria and gangrene.2,3 A multisystem inflammatory syndrome that includes skin changes has also been noted in children with COVID-19.2,3
Pathophysiology of COVID-19 skin changes
The dermatological signs of COVID-19 are believed to be due not to direct damage caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) itself, but rather to the elevated immune response to the virus. Overactivation of the complement system leads to microvascular damage, which is already increased in older people and may explain their higher rates of severe disease and mortality.4 The vaso-occlusive (clotting) consequences of COVID-19 have been recognised to affect many organ systems and are thought to be also responsible for some of the skin changes.4 Male-pattern baldness has been linked with increased risk of hospitalisation and severe disease.5 This may be due to an increased level of the hormone dihydrotestosterone, which upregulates ACE2 receptors, the receptors that allow entry of SARS-CoV-2 into the cell.5
Common skin changes associated with COVID-19
Maculopapular eruptions
A maculopapular eruption is believed to be the most common skin sign associated with COVID-19 (Figures 1a and b). The rash is mostly truncal, comprising widespread small erythematous macules and papules. This type of eruption can occur at any time from the onset of illness to weeks later. Maculopapular eruptions have been associated with more severe COVID-19, with up to 2% mortality in patients with this rash.4
{kind=link}
COVID toes
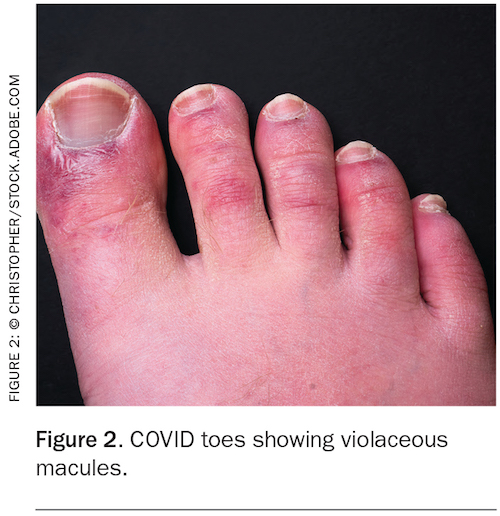
‘COVID toes’, or pernio or acral chilblain- like lesions (CLL) in the absence of cold exposure, are also very common and make up about 18% of reported dermatological manifestations of COVID-19.3,4 COVID toes present as erythematous or violaceous itchy and painful macules over the hands or feet, with occasional vesicles or pustules (Figure 2).
{kind=link}
COVID toes occur later in the course of COVID-19 and are an indicator of mild disease.4,6 The condition is most common in children and in patients with a lower body mass index and is more often documented in European and US populations than in Asian populations.4,6 The pathophysiology is believed to involve a combination of vasospasm and a type I interferon immune response.4,6
Interestingly, patient presentations with CLL have increased significantly in the general population during the COVID-19 pandemic despite many of these patients having a negative PCR result for SARS-CoV-2. It is hypothesised that CLL may be a late sign of COVID-19, when SARS-CoV-2 can no longer be detected by nasal PCR tests. Alternatively, SARS-CoV-2 may cause isolated cutaneous effects, supported by the isolation of viral fragments from skin biopsy specimens of asymptomatic patients with a negative nasal PCR result.6
No specific management has been recommended for COVID toes, although some clinicians report a response to topical corticosteroids.3
Acute urticaria
Acute urticaria has been seen in COVID-19 patients, consisting of itchy erythematous raised oedematous wheals that resolve quickly (Figure 3). These wheals sometimes occur at the onset of fever and other symptoms, resolving within hours but reappearing in a different distribution. Urticarial eruptions have been noted to resolve completely in COVID-19 patients usually within 24 hours to 10 days.3,4 They are more common in middle-aged women and have been associated with mild or moderate disease.4
{kind=link}
Acute urticaria does not require specific treatment unless it bothers the patient. The itch can be treated with a trial of nonsedating antihistamines or menthol cream.
Livedo reticularis and retiform purpura
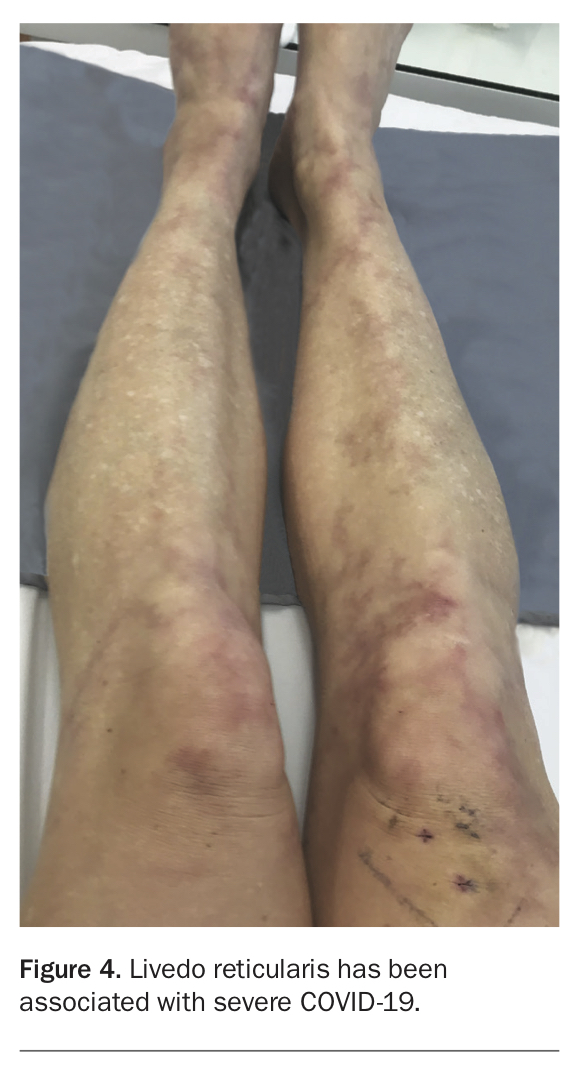
Livedo reticularis is a net-like purpuric eruption that is often described as bruise-like (Figure 4). Retiform purpura consists of stellate purpuric patches or plaques that can show necrosis or ulceration. Livedo reticularis and retiform purpura are believed to be due to thrombo-occlusion of blood vessels and complement-mediated microvascular damage.4
{kind=link}
These skin signs have been associated with severe COVID-19, more commonly in older patients.4,7 They are also associated with higher rates of intensive care admission and mortality.4 In a case series of 11 patients with retiform purpura, all were hospitalised and nine had acute respiratory distress syndrome requiring intensive care admission.8
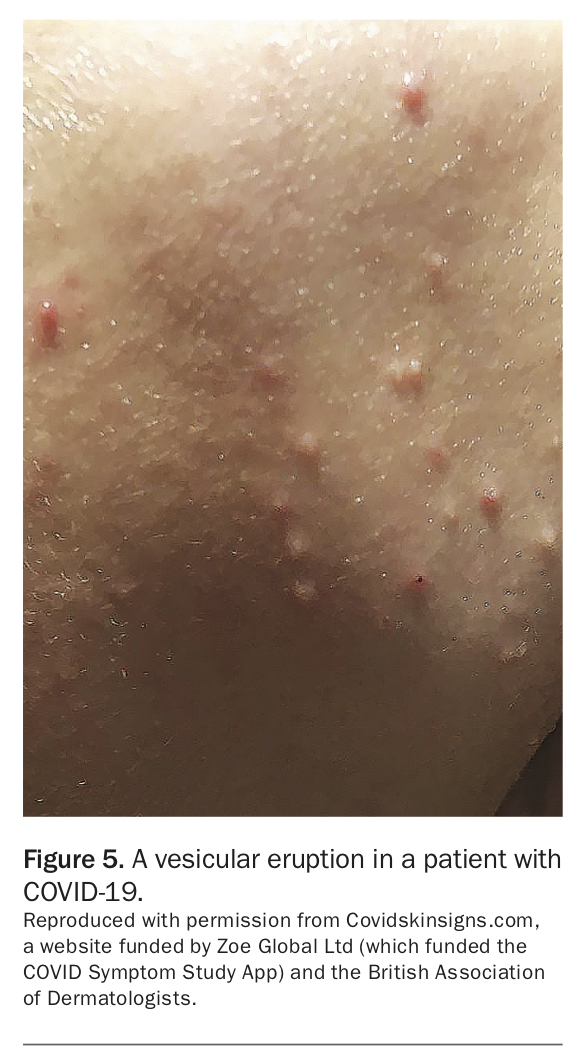
Vesicular eruption
A vesicular eruption has been seen in patients with COVID-19, consisting of small fluid-filled blisters most often on the trunk or hands (Figure 5). It occurs early in the disease course and has been associated with medium-severity COVID-19.4 Middle-aged patients are more likely to be affected. The vesicular eruption commonly lasts about 10 days.4
{kind=link}
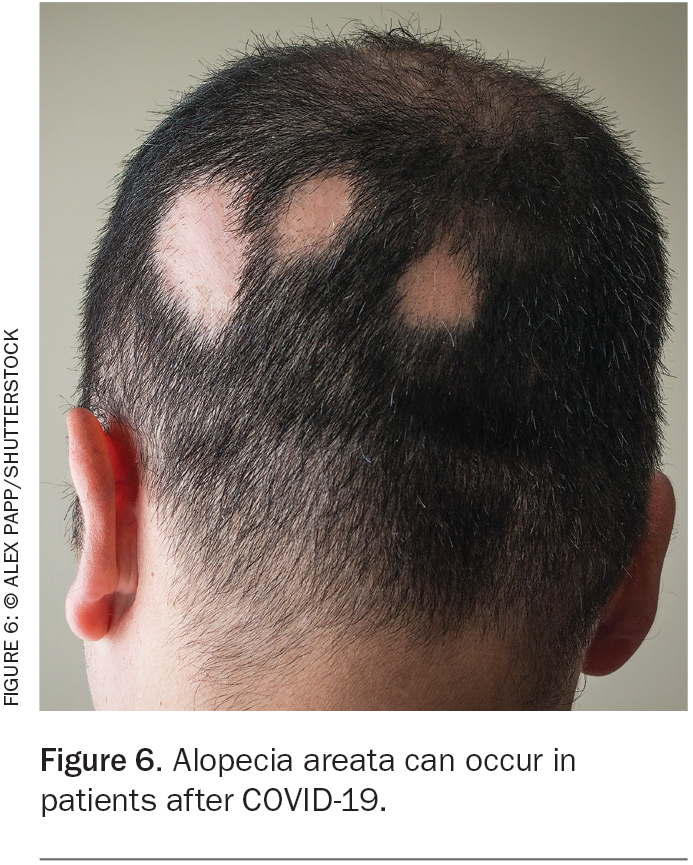
Hair and nail changes
Hair loss (telogen effluvium and alopecia areata) can occur in many illnesses, including COVID-19, as a sign of a significant stressor on the body (Figure 6). Hair loss is usually a late sign or arises after COVID-19 illness has resolved.9 Most hair loss resolves over time with minimal intervention. Ensuring patients’ iron levels are optimised by correcting any deficiency assists with this process.
{kind=link}
A range of nail signs have been seen in COVID-19 patients, including transverse ridges and red-violet lines (the red half-moon sign), distal onycholysis (nail plate separation) and an orange discolouration of the nail plate.2,9 These signs usually appear late in the disease course or in the recovery stage and can persist for weeks to months.9
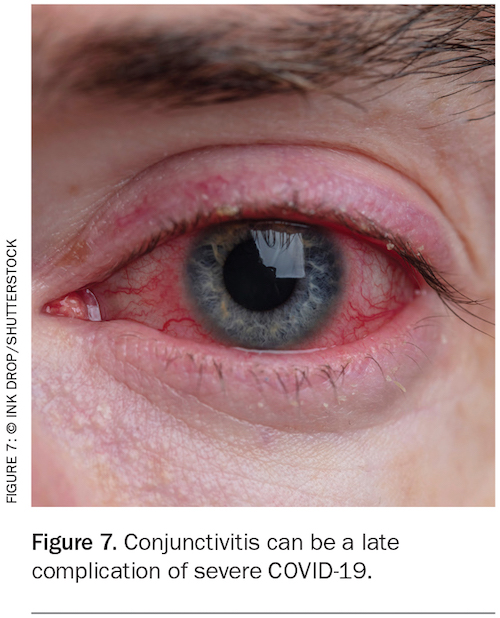
Conjunctivitis
Conjunctivitis has been seen in COVID-19 patients, most commonly later in disease progression and in patients with severe disease (Figure 7).
{kind=link}
Multisystem inflammatory syndrome in children
A multisystem inflammatory syndrome in children (MIS-C) has also been associated with COVID-19, with a constellation of signs that include erythema and oedema of the hands and feet, oral mucositis, conjunctivitis and a polymorphic erythematous eruption.3,10 This immune system ‘overdrive’ triggers inflammation of the heart and blood vessels similar to atypical Kawasaki disease, resulting in blood clots and symptoms of shock. Also termed paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS), this is a rare complication that typically occurs two to six weeks after a child has had COVID-19.10 Screening for vascular complications should be considered for patients who present with other signs of this syndrome.
Cutaneous changes after COVID-19 vaccination
Some cutaneous changes have been associated with COVID-19 vaccines, the most common being injection-site reactions, angioedema and urticaria.11 Maculopapular and morbilliform eruptions and pityriasis rosea have also been seen after vaccination. For some patients with dermatological conditions such as psoriasis or atopic dermatitis, flare ups have been reported after vaccination.11
Conclusion
Some dermatological signs of COVID-19 appear early in the disease, such as urticaria, maculopapular eruptions and vesicular eruptions. Testing for COVID-19 should be considered in patients with these rashes, if not already performed, to capture all positive cases. Other dermatological signs occur later in the disease course, such as COVID toes and conjunctivitis.
Vaso-occlusive skin signs such as livedo reticularis and retiform purpura and MIS-C are signs of more severe disease and can lead to severe complications. Patients with these skin signs require careful monitoring, referral and follow up. Most skin manifestations resolve within days to weeks and can be managed with simple measures, such as corticosteroid creams or antihistamines. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.