Patella instability: diagnosis and management

Patella instability is an important diagnosis in young active individuals with a history of acute knee injury. In high-risk individuals, instability can become chronic and, if left untreated, increase risk of secondary cartilage defects and early onset osteoarthritis.
The presentation of patella instability can range from sudden acute debilitating dislocation requiring urgent reduction to more minor episodes of subluxation. Both males and females can suffer from patella instability but it is more common in females, with many suffering their first dislocation as a teenager. In the general population, patella dislocations occur at a rate of 5.8 per 100,000; female athletes aged 10 to 17 years have the highest risk, with a reported rate of 33 per 100,000.1
The mechanism of injury is often a noncontact twisting injury where the knee is in a slightly flexed position with an externally rotated foot. Acute patella dislocation can also occur with direct trauma such as a knee-to-knee collision to the medial patella, although this is a less common mechanism of injury.
After an acute patella dislocation, pain, swelling and feelings of instability can incapacitate individuals for up to six to eight weeks. In the longer term, instability events can become chronic, occurring more frequently, significantly limiting an individual in activities of daily living and, if left untreated, increasing risk for developing secondary cartilage defects and early onset osteoarthritis. Concerningly, these day-to-day limitations can result in an otherwise healthy individual essentially becoming a young person with ‘old knees’.
Anatomy
The cause of patella instability is a multifactorial problem that relates to the distribution of forces through the patellofemoral joint during normal daily activities. The primary function of the patella is to increase the lever arm of the quadriceps, the main antigravity muscle of the body, increasing its knee extension strength. Movements that involve loaded flexion and extension of the knee place considerable strain on the patellofemoral joint, with activities such as jogging and deep squats resulting in joint reaction forces of up to seven times an individual’s bodyweight going through the knee.2,3
Appropriate distribution of these large forces is necessary to maintain a normal functioning patellofemoral joint. Important contributors to normal patella biomechanics include lower limb alignment, gait pattern, bony morphology of the patella and femur and a balance between the soft tissue constraints and the surrounding musculature. At 30-degrees of knee flexion, the patella fully engages into the trochlea groove on the femur, where it relies predominantly on these bony constraints to centralise it under increasing amounts of load.
Anatomical variants that reduce the bony constraints of the patellofemoral joint predispose individuals to episodes of patella instability. These variants include a high riding patella (patella alta), a flat trochlea groove (trochlea dysplasia), lateral patella tilt and a deficient lateral femoral condyle. These deficiencies in bony constraints cause the patellofemoral joint to become more reliant on soft tissues to distribute the joint reaction forces and maintain normal biomechanics. Individuals at a high risk of initial patella dislocation and subsequent redislocation may suffer from two or three of these anatomical variants. The more variants they suffer from, the greater the risk of chronic instability.
Important soft tissue constraints include the medial patellofemoral ligament (MPFL), which attaches proximally on the medial border of the patella and inserts near the medial epicondyle of the femur, which acts primarily as a lateral restraint at 0- to 30-degrees of knee flexion. The MPFL works in conjunction with the vastus medialis obliquus to guide the patella medially to maintain centralised tracking; however, the forces from vastus lateralis and the iliotibial band (ITB) are often stronger and will have a tendency to sublux the patella into the lateral position (Figures 1a and b).
{kind=link}
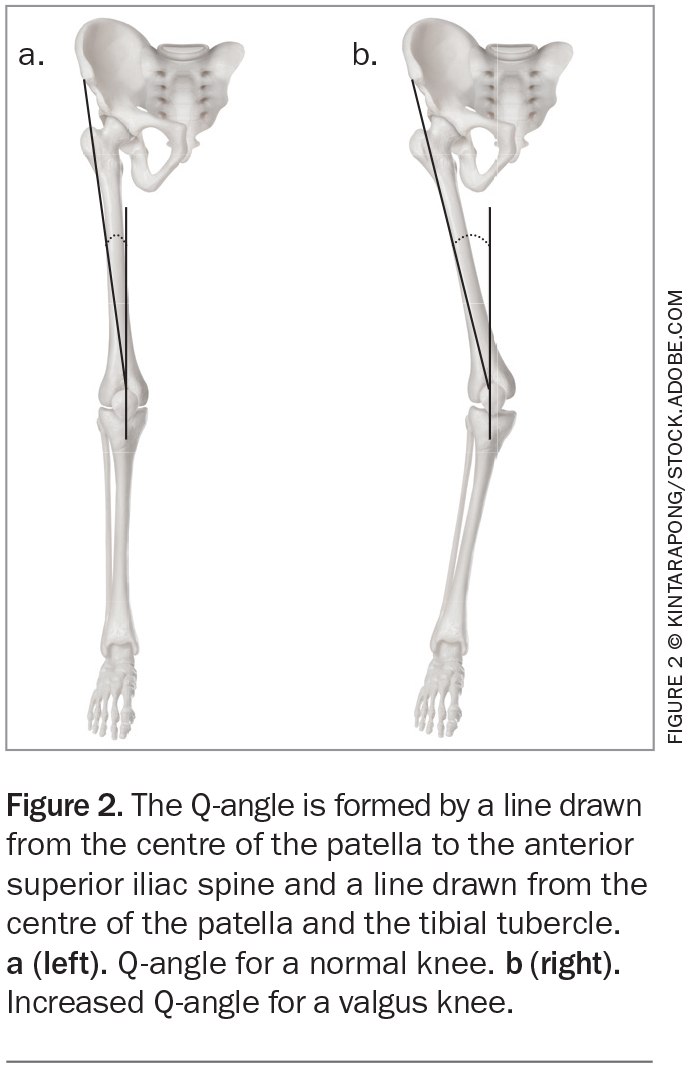
Lower limb alignment can also affect the distribution of forces throughout the knee. The Q-angle, which is an indicator of the combined forces that the quadriceps and patella tendon exert on the patella, can be useful (Figures 2a and b). The trio of valgus knee alignment, femoral anteversion and foot pronation, which is termed ‘miserable malalignment syndrome’, often results in an increased Q-angle which will allow the quadriceps to translate the patella laterally throughout the knee range of motion and increase an individual’s risk for patella instability.
{kind=link}
Diagnosis of patella instability
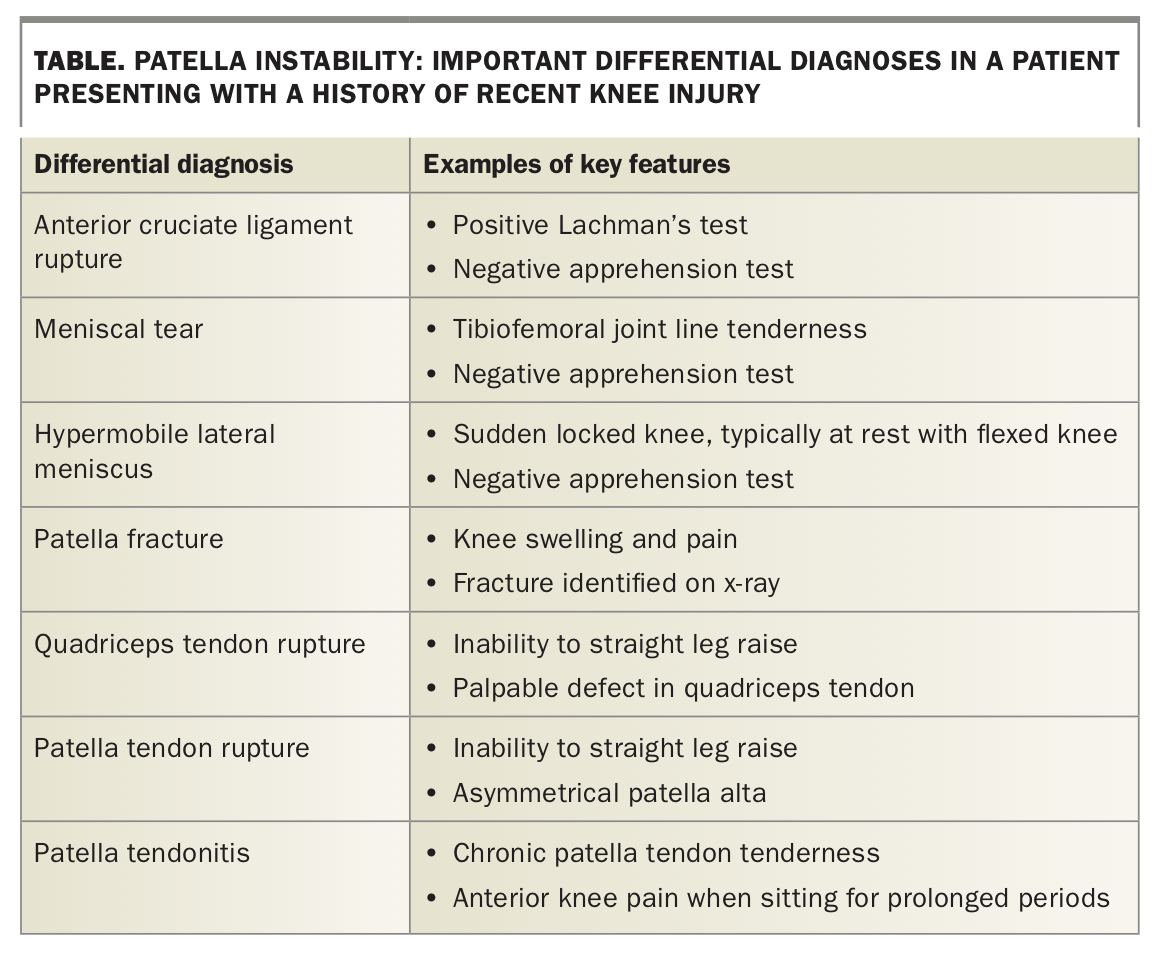
As patients can present at any time in the course of their patella instability, establishing an accurate and timely diagnosis can be difficult. Important differential diagnoses that should be considered in a patient with a recent knee injury are listed in the Table.
{kind=link}
History
Patient assessment should begin with a careful history detailing the patient’s symptoms and the age of onset. It is important to differentiate symptoms that originated with a traumatic episode from an onset that was more insidious, as this will assist in determining the cause of the pain.
Important points that will affect management include the mechanism of injury (contact or noncontact, high-energy or low-energy), whether a reduction in the emergency department was required, recurrent episodes, symptoms of locking or catching that could represent an osteochondral loose body (Figure 3) or meniscal tear, and problems with other joints. The most important predictor of future patella instability is previous episodes of instability.
{kind=link}
Examination
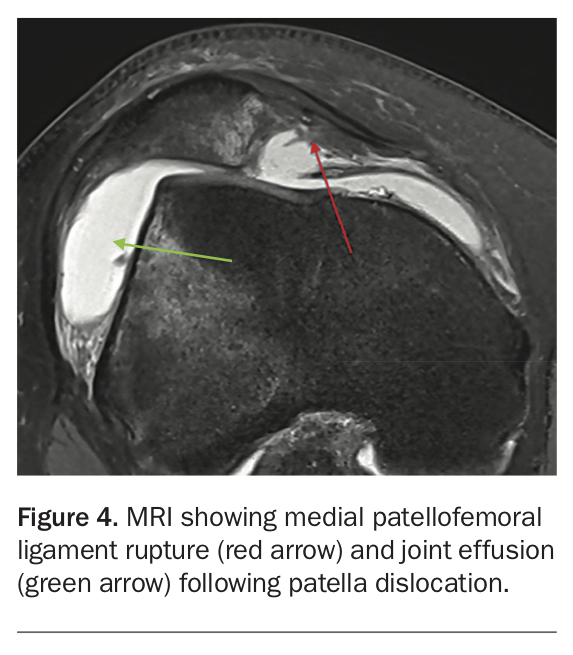
Patients with an acute traumatic episode of patella instability or dislocation present differently to those with a recurrent dislocation. In the acute setting, examination will be difficult; the patient will have a significant joint swelling related to MPFL rupture (Figure 4) or medial patella avulsion. Patients may present with the patella dislocated, in which case they often have their knee in a fixed flexed position with a large bony deformity on the lateral aspect of the knee (Figure 5). The priority at this point is to reduce the patella and immobilise the knee (see below), allowing further examinations to be performed in the subacute setting when symptoms allow.
{kind=link}
{kind=link}
A patient who presents with a described episode of patella instability but has no effusion is likely to have had a recurrent episode. At this stage, it is possible to perform an examination for predisposing factors. Important signs to look for in a patient with suspected chronic patella instability include wasting of the vastus medialis obliquus, high riding patella, Q-angle greater than 20 degrees, and tight quadriceps and iliotibial band.
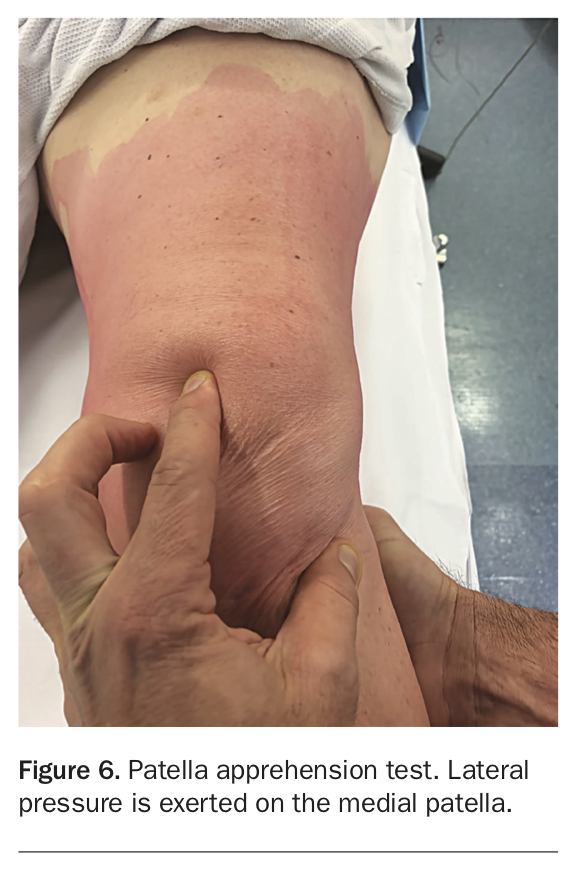
Patients should be tested for patella apprehension (Figure 6). To perform the test, the patella is translated laterally with the knee in slight flexion. A positive result occurs when the patient demonstrates apprehension during this movement. This test is typically positive after prior dislocation events and has a high specificity for patella instability.
{kind=link}
Assessment of J-tracking, which involves actively bringing the knee from flexion to full extension, is useful. As the knee nears full extension and the patella disengages the trochlea, a sharp lateral deviation of the patella indicates a positive test, which can be a sign of trochlea dysplasia or patella alta.
To complete the examination, the patient should be assessed for valgus lower limb alignment, malrotation and signs of ligamentous laxity using Wynne-Davies criteria (for further details of these criteria, see https://www.researchgate.net/ publication/235440516_Sports_hip_injuries_assessment_and_ management).4
Investigations
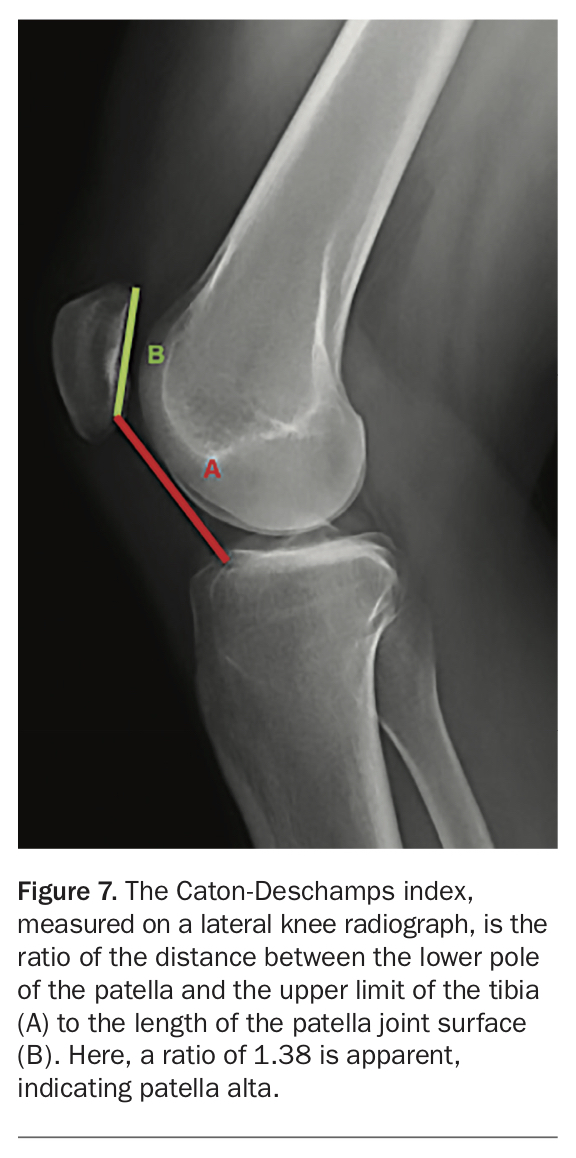
Standard AP and lateral radiographs provide important information into any joint injury and are necessary to exclude an underlying fracture, which can commonly occur where the medial patella facet is avulsed. Additional imaging can be used to identify anatomical variants that predispose patients to patella instability. True lateral radiographs where the knee is positioned in 30-degrees of flexion can be used to assess for bony variance of patella alta and trochlea dysplasia. A variety of radiographic measures can define patella alta, the most commonly used being the Caton-Deschamps index shown in Figure 7: a ratio between 0.6 and 1.3 is normal, with a ratio greater than 1.3 indicating patella alta. Lateral radiographs on the anterior femoral cortex can present with crossover, double contour or supratrochlear spurs that indicate trochlea dysplasia. Skyline views can also be useful for assessing trochlea depth and patella position. Long leg alignment radiographs can also be used to assess for valgus malalignment.
{kind=link}
In the acute setting of a patella dislocation, a patient may not tolerate the positioning necessary for the specific radiographs described above due to pain and swelling.
MRI is useful for assessing soft tissues, particularly the integrity of the cartilage and the presence of any osteochondral defects. MRI will identify MPFL injuries (Figure 4) and any other articular pathology which may include a meniscal tear or ACL rupture. MRI has been used to calculate patella translation using TT-TG distance (tibial tuberosity-trochlea groove) for surgical planning; however, a recent study has suggested that MRI may underestimate the values when compared with CT.5 CT scans may be required to assess complex rotational lower limb deformities.
Management of patella instability
Nonoperative management
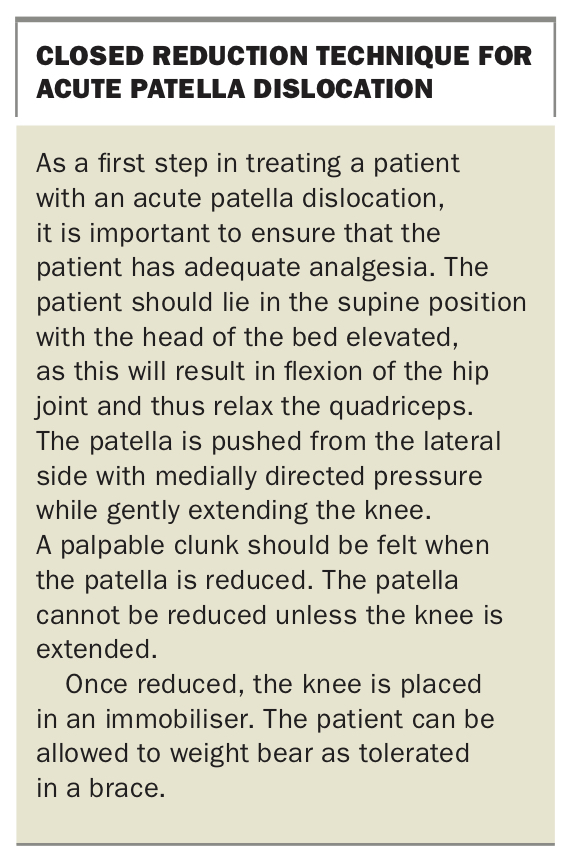
The closed reduction technique used to treat acute patella dislocation is described in the Box.
{kind=link}
In the absence of any loose bodies or other pathology, nonoperative management is the mainstay of treatment for the acute episode of patella dislocation. This includes use of anti-inflammatories and immobilisation for comfort, usually for two to three weeks, in a brace that keeps the lower limb in extension. Once pain and swelling improve the patient should begin rehabilitation under the guidance of a physiotherapist. Rehabilitation programs are individualised to address patient-specific muscular imbalances. Programs include controlled range of motion exercises and vastus medialis obliquus strengthening, often in conjunction with activity modification and hip abductor and core strengthening to improve overall lower limb positioning.
Patients who have dislocated their patella for the first time and do not have significant osteochondral injuries can be managed by their GP with rehabilitation to reduce the risk of further episodes. Patients suffering two or three episodes require specialist advice.
Operative management
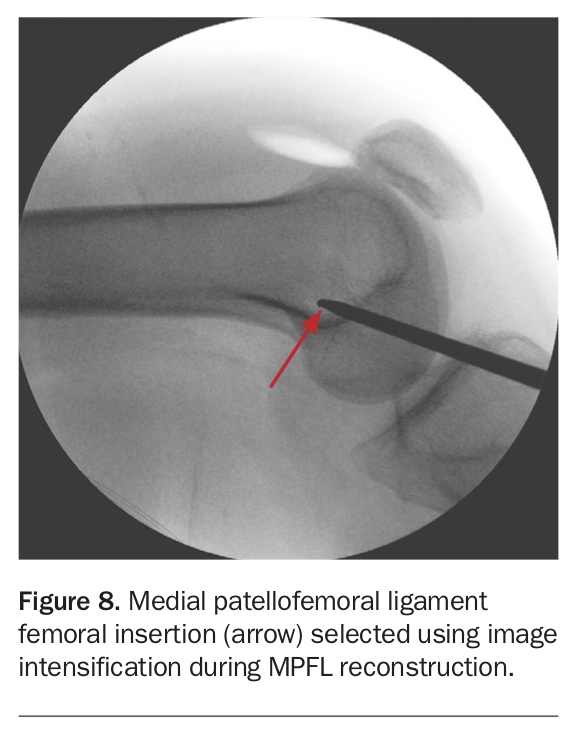
Patellofemoral reconstruction is typically indicated after two or three dislocations. The current gold standard for all patients is MPFL reconstruction, typically using a hamstring tendon (Figure 8). Occasionally a bony procedure may also be indicated, such as a distalisation of the tibial tubercle if severe patella alta exists. Reshaping the trochlear (trochleoplasty) and/or derotational osteotomies, is usually reserved for revision cases. MPFL reconstructions are typically short stay procedures and full recovery takes four to six months. Redislocation rates are approximately 3 to 5% and usually occur in individuals with multiple anatomical risk factors.
{kind=link}
Uncommonly, patients may require arthroscopic fixation or removal of chondral and osteochondral fragments from the joint.
Conclusion
Patella dislocation most commonly affects young active individuals and can lead to chronic instability in high-risk individuals. Plain radiographs are indicated for patients who have dislocated their patella for the first time to exclude fractures and can prognosticate on redislocation risk based on patellofemoral morphology. MRI may be indicated in initial dislocations or to exclude other intra-articular pathologies such as meniscal tears or ACL ruptures. A patient who has dislocated the patella for the first time without significant osteochondral injuries can be managed with anti-inflammatories, immobilisation and physiotherapy with a gradual return to activity. Individuals with osteochondral injuries or recurrent dislocation should be referred to a specialist and may require surgical management. MT
References
235440516_Sports_hip_injuries_assessment_and_management (accessed June 2020).