Mycoplasma genitalium. The state of play

Mycoplasma genitalium has emerged as the causative agent of sexually transmitted syndromes including urethritis in men, cervicitis and pelvic inflammatory disease in women; however, testing should be limited to specific clinical scenarios. Treatment challenges include widespread macrolide resistance and the emergence of multidrug-resistant strains. Treatment failure is not uncommon and resistance-guided therapy currently offers the highest probability of cure.
Mycoplasma genitalium infection is a bacterial sexually transmitted infection (STI). M. genitalium belongs to the bacterial class Mollicutes, distinguished by their tiny genome and absent cell wall (Figure). M. genitalium is an extremely slow-growing and fastidious organism to culture;1 therefore, studies showing its association with genital syndromes really only began to accumulate after the development of the first diagnostic polymerase chain reaction (PCR) test in the early 1990s. Since the isolation of M. genitalium from the urethras of two men with nongonococcal urethritis in the early 1980s, evidence has shown its association with other clinical syndromes, including cervicitis, pelvic inflammatory disease and poor pregnancy outcomes in women.1,2
{kind=link}
Genital syndromes associated with M. genitalium
M. genitalium is a well-established cause of nongonococcal urethritis (pooled odds ratio [OR], 5.5 [95% confidence interval (CI), 4.3-7.0]) and chronic persistent nongonococcal urethritis in men.1,3,4 With fewer studies performed in women and smaller sample sizes, the association of M. genitalium with female genital syndromes has been harder to establish. However, M. genitalium has been shown to be significantly associated with cervicitis (OR, 1.66 [95% CI, 1.35-2.04]) and pelvic inflammatory disease (PID; OR, 2.14 [95% CI, 1.31-3.49]). This meta-analysis also suggested M. genitalium is associated with tubal factor infertility and poor pregnancy outcomes (preterm delivery and spontaneous abortion), although data supporting these associations were more limited, particularly in pregnant women.2
M. genitalium has been detected in the rectum in men who have sex with men (MSM), with significantly higher rates in those living with HIV infection.5 Although there have been case series describing M. genitalium-associated proctitis, data are conflicting as to whether M. genitalium is significantly more common in men with proctitis compared with asymptomatic controls; therefore, its role as a causative agent in proctitis remains somewhat controversial and unclear.6-9
Prevalence
Population-based studies in the US, UK and Europe have reported a prevalence of M. genitalium infection in the general population in both men and women of 1 to 3.3%.10 M. genitalium infection is more common in higher-risk populations such as sexual health clinic attendees and MSM, in whom estimates of prevalence in the order of 7% and 9.5% were reported, respectively.8,11,12
Antimicrobial resistance
M. genitalium has no cell wall and, therefore, antibiotics such as penicillins or other beta-lactams, which target the cell wall, are ineffective. Antimicrobials that inhibit protein synthesis or DNA replication are required to treat this infection. The main currently available options with demonstrated efficacy include macrolides, streptogramins and later-generation fluoroquinolones.13
Although doxycycline appeared promising from early in-vitro studies, used alone it cures about 30% of infections.14,15 However, a recent study in Melbourne showed the use of doxycycline for one week before subsequent treatment with a macrolide or fluoroquinolone significantly lowered bacterial load and improved overall likelihood of cure.13
Azithromycin was very potent in early susceptibility testing;14 however, it now cures only 50% of infections globally, due to the rapid development of macrolide resistance. Australian studies have shown that macrolide resistance mutations are currently detected in 50% of M. genitalium strains from heterosexuals and in more than 80% of strains from MSM.8,15 Macrolide resistance is caused by single nucleotide polymorphisms in the 23s rRNA gene, which also arise de novo in 10% of macrolide-susceptible infections after treatment with a 1g single dose of azithromycin.13,16 The number of de-novo mutations is reduced to 3.8% when an extended azithromycin regimen is used.16,17
Moxifloxacin is under similar pressure from emerging resistance, with a meta-analysis reporting a decline in cure rates from 100% in studies before 2010 to 89% in studies after 2010.18 Moxifloxacin resistance is caused by mutations affecting the quinolone resistance-determining regions, predominantly in the parC gene.19 These mutations were detected in 20% of infections at Melbourne Sexual Health Centre in 2016-2018.19
Testing for M. genitalium infection
To screen or not to screen?
Although the prevalence of M. genitalium is similar to that of chlamydia, when it comes to screening, the situation for M. genitalium is significantly more complex and therefore screening is not currently recommended.20,21 First, most infections remain asymptomatic and there are limited data regarding the natural history of M. genitalium and long-term sequelae of asymptomatic infection.22
Furthermore, increasing antimicrobial resistance is resulting in the need to treat patients with costly antimicrobials that have uncommon but potentially serious adverse effects. These complexities generate considerable uncertainty regarding the potential cost benefit of screening, as the risk of adverse outcomes of treatment may exceed the risk from the infection itself. Until drug regimens that are more efficacious with fewer and less serious side effects become available, the benefit of testing and treating asymptomatic infection does not appear to outweigh risk on an individual or population level.
When to test
Testing for M. genitalium is currently recommended and supported by evidence in the following groups or clinical scenarios:
- men with nongonococcal urethritis
- women with cervicitis or PID
- sexual contacts of people with M. genitalium infection
- test of cure (TOC) two to three weeks after completion of antimicrobial treatment for M. genitalium infection.
Routine testing is not currently recommended for MSM with proctitis, although it may be indicated in those with persistent symptoms who first test negative to other known pathogens. Although M. genitalium can co-exist with other STIs, the presence of another infection is not in itself an indication to screen for M. genitalium.
How to test
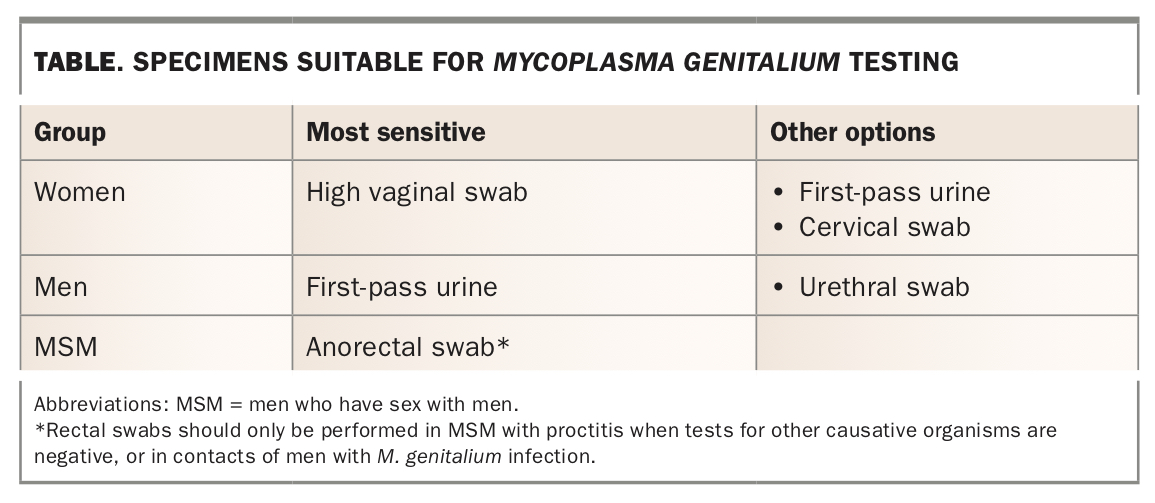
Nucleic acid amplification testing (NAAT) and PCR testing are now available in laboratories throughout Australia and are TGA approved. Some assays provide simultaneous reporting of macrolide resistance markers, which enables selection of antibiotics based on evidence of macrolide resistance. Suitable specimens for testing in different patient groups are listed in the Table.
{kind=link}
Management of M. genitalium infection
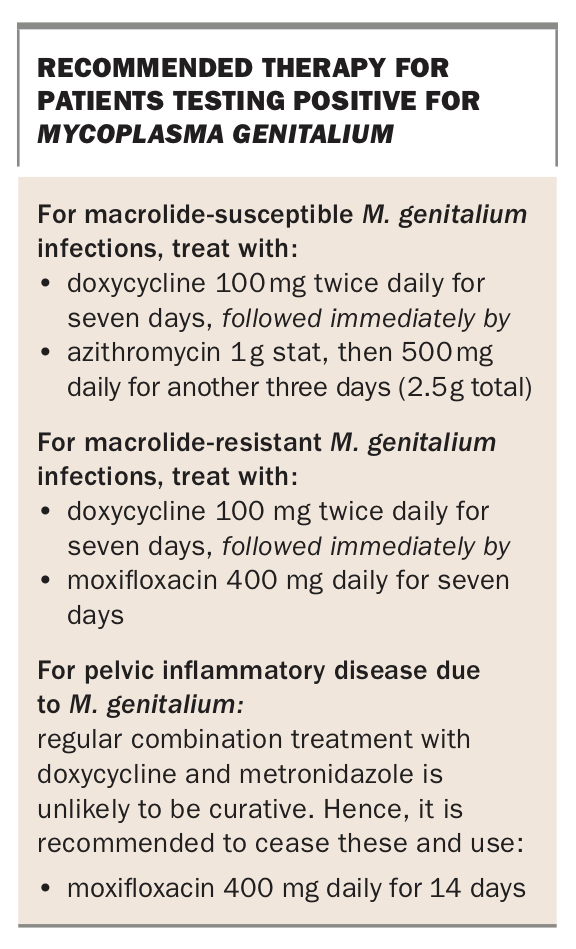
To avoid selection of macrolide resistance, syndromic management of nongonococcal urethritis and cervicitis should be with doxycycline 100 mg twice daily for seven days rather than single-dose azithromycin. Similarly, the use of single-dose azithromycin for treatment of PID is no longer recommended. These changes are reflected in both the Australian STI management guidelines and Centers for Disease Control and Prevention STI guidelines.23,24 Patients presenting with these clinical syndromes should be tested for M. genitalium (ideally with macrolide resistance testing) at baseline and recalled for resistance-guided therapy if positive (Box).
{kind=link}
Moxifloxacin can be associated with significant side effects including diarrhoea, tendonitis, neurological complications and cardiac events. It is not recommended in pregnancy (Category B3). Patients should be counselled before use; and when contraindications exist, alternative options should be considered. Although moxifloxacin is not currently TGA approved for treatment of M. genitalium, it is the recommended first-line treatment in all macrolide-resistant infections.
Considerations before treatment
Clinicians should maintain a high index of suspicion for treatment failure, particularly in settings where assays for detection of macrolide resistance are not available. Patients should be advised to abstain from sex or adhere to strict condom use until a TOC is negative. This should be performed two to three weeks after completion of antimicrobial therapy and is advised, given the high rates of resistance and persisting infection. When the above treatment fails (positive TOC), other antimicrobial options are available; however, these need to be accessed with input from a sexual health physician.
Other antimicrobial options for treatment failures
Pristinamycin is a streptogramin antibiotic that is used primarily in the treatment of staphylococcal infections. It will cure 75% of macrolide-resistant M. genitalium infections.25 Although not used as first-line treatment, it can be used in combination with doxycycline when fluoroquinolones have failed (or are contraindicated), or as monotherapy when doxycycline is contraindicated (such as during pregnancy and breastfeeding; pregnancy Category D).
Pristinamycin is available through hospital pharmacies (or via a specialist sexual health centre) using the Special Access Scheme of the TGA. Global shortages have been experienced at the end of 2019 into early 2020. When it is available, the recommended treatment is pristinamycin 1 g three times daily in combination with doxycycline 100 mg twice daily for 10 days. The recommended dose as monotherapy (with no combination doxycycline) is pristinamycin 1 g four times daily for 10 days.21
Four case reports exist in which M. genitalium infection that had failed treatment with both azithromycin and a quinolone was cured with an extended course of minocycline.26,27 Minocycline is a tetracycline and is thought to be more effective than doxycycline, owing to lower mean inhibitory concentrations. However, data on minocycline are limited to published case reports as above, and treatment failures following its use have occurred in Melbourne (personal communication, C. Bradshaw).
A large Melbourne-based study achieved cure rates of 92.2% using sitafloxacin after seven days of doxycycline treatment of macrolide-resistant M. genitalium infection.13 Sitafloxacin has lower mean inhibitory concentrations than moxifloxacin and has been shown to cure strains harbouring quinolone resistance mutations.15 However, sitafloxacin is difficult to access and is currently only available through specialist centres.
How should we manage sexual partners?
Symptomatic or asymptomatic sexual contacts of people with M. genitalium infection, particularly those in a continuing relationship with a symptomatic person, should be offered testing, and treatment if the test result is positive. Studies in Melbourne showed that 48% of women, 42% of MSM and 31% of heterosexual males reporting sexual contact with an index case were also infected.28
Partners can be treated presumptively according to the resistance profile of the index case to expedite management. If antibiotic treatment has failed in the index case, it can be assumed the same treatment will fail in the partner. MSM who are contacts require urine and anorectal swabs. Throat swabs are unnecessary as pharyngeal infection is rare (1%).21
Conclusion
M. genitalium has emerged over the past 30 years as the causative agent of important and common sexually transmitted syndromes, particularly urethritis in men, cervicitis and PID in women. Macrolide resistance is widespread and multidrug-resistant strains are emerging.
Testing in patients should be limited to specific clinical situations and, when possible, assays enabling detection of macrolide resistance mutations should be used. Resistance-guided treatment currently offers the highest probability of cure and reduces further development of antimicrobial resistance. A TOC should be performed two to three weeks after completion of antimicrobial therapy. Sexual partners should be tested and treated whenever possible. If infection persists despite treatment with first- or second-line antimicrobial regimens, guidance should be sought from a sexual health physician for further management.
More research is needed into the natural history of asymptomatic infection before screening can be recommended. There is an imperative to develop novel and inventive treatment strategies, including combinations of existing drugs, to target this ever-evolving pathogen. MT