Chronic kidney disease: detection, prevention and early-stage management
Chronic kidney disease (CKD) is an increasing problem among our ageing population and is associated with significant cardiovascular morbidity and mortality. Targeted screening and optimal early management of patients in primary care can prevent the worst outcomes of CKD.
- Estimated glomerular filtration rate and albuminuria should both be used to predict risk of chronic kidney disease (CKD) progression and are both independently associated with an increased risk of cardiovascular disease and mortality.
- Recommended assessment before referral to a nephrologist includes measuring blood pressure (BP), biochemical and haematological testing, urinary albumin to creatinine ratio, urine microscopy for red cell morphology and casts, and urinary tract ultrasound.
- BP control in patients with CKD should be optimised according to cardiovascular risk while balancing the risks of more intensive BP treatment.
- Sodium-glucose cotransporter-2 inhibitors should be considered in high-risk patients with diabetic kidney disease and macroalbuminuria due to their renal and cardiovascular benefits.
- Patients with CKD commonly have hyperuricaemia but should only be prescribed urate-lowering therapy if they already have gout or urate calculi.
- Salt restriction and the Dietary Approach to Stop Hypertension diet are recommended in hypertensive patients. Persistent hyperkalaemia and hyperphosphataemia may warrant input from a nephrologist and dietitian.
- Parenteral or oral iron should be used to treat anaemia associated with CKD. Metabolic acidosis may be treated with oral sodium bicarbonate.
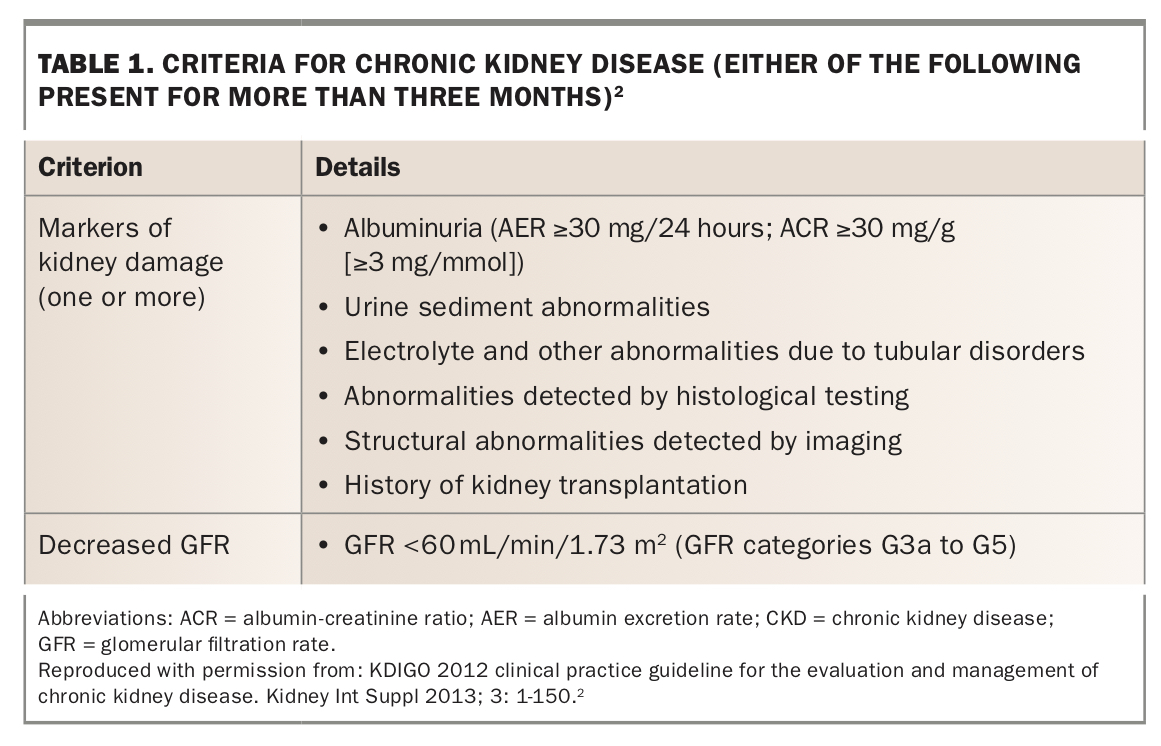
Chronic kidney disease (CKD) is a major public health problem associated with the increased incidences of diabetes and hypertension, and an ageing population.1 CKD is defined as abnormalities of kidney structure or function present for more than three months (Table 1).2 The Australian Institute of Health and Welfare reported that about 1.7 million adult Australians (10%) had CKD in 2011–12;3 however, only 6.1% self-reported a diagnosis of CKD in the Australian Bureau of Statistics 2017–18 National Health Survey.4 This reflects the asymptomatic nature of CKD, which is often detected late in the disease course when therapeutic interventions are less effective.
{kind=link}
Early detection, prevention and management of CKD are essential in reducing the health burden of kidney disease progression and associated cardiovascular disease (CVD). The incidence of end-stage kidney disease (ESKD) requiring dialysis or kidney transplantation in Australia is steadily increasing.5 The burden of ESKD is highest among people over 65 years of age, Aboriginal and Torres Strait Islander people, people living in remote and very remote areas, and the lowest socioeconomic group.6 The cumulative cost of treating ESKD is estimated to be $12.3 billion in 2020, up from $4.1 billion in 2012.7
Furthermore, both reduced estimated glomerular filtration rate (eGFR) and albuminuria are independent risk factors for CVD and death. The risk of cardiovascular and all-cause mortality is tripled by an eGFR of 15 mL/min/1.73m2 and doubled by a urinary albumin-creatinine ratio (uACR) of 30 mg/mmol.8 CKD is associated with increased cardiovascular risk beyond the management of ‘traditional’ modifiable risk factors.
This article reviews the investigation and management of the early stages of CKD. A comprehensive review of the management of ESKD including dialysis or nondialysis conservative care is beyond the scope of this review.
Detecting and evaluating CKD
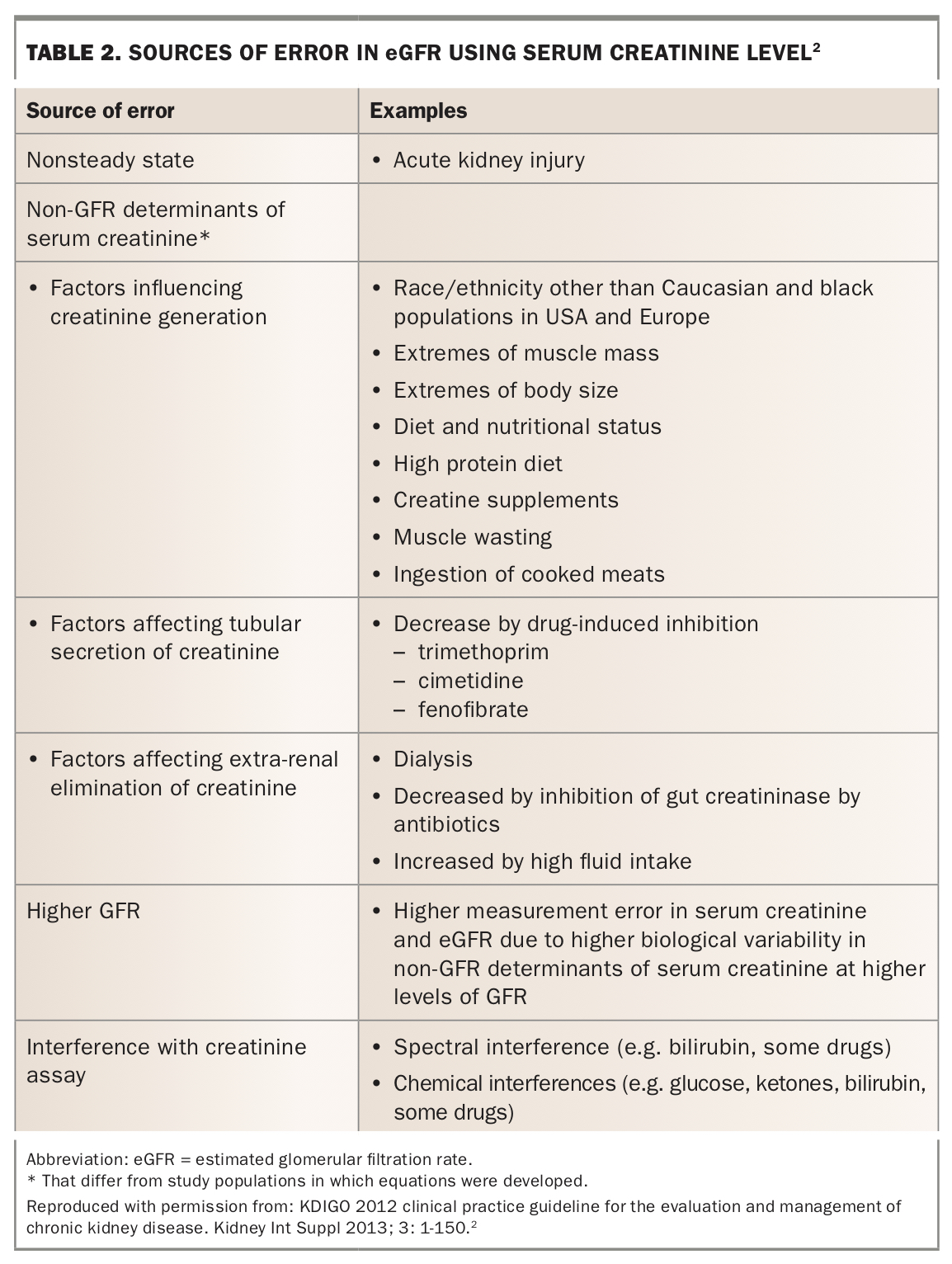
Screening for CKD should be targeted to individuals at increased risk of developing CKD, including those with diabetes, hypertension, established CVD (such as coronary heart disease, cerebrovascular disease or peripheral vascular disease), obesity, smoking history, previous history of acute kidney injury, family history of CKD or age greater than 60 years, or 30 years and over in the case of Aboriginal and Torres Strait Islander people.9 Detection of CKD is often based on eGFR using serum creatinine level and the CKD Epidemiology Collaboration formula, since CKD is often asymptomatic in its early stages.9,10 Although estimating kidney function using eGFR is more accurate than using serum creatinine level alone, sources of error in eGFR include nonsteady state conditions (such as acute kidney injury), non-GFR determinants of serum creatinine level, inaccuracies at higher GFR and factors that influence the creatinine assays (Table 2).2
{kind=link}
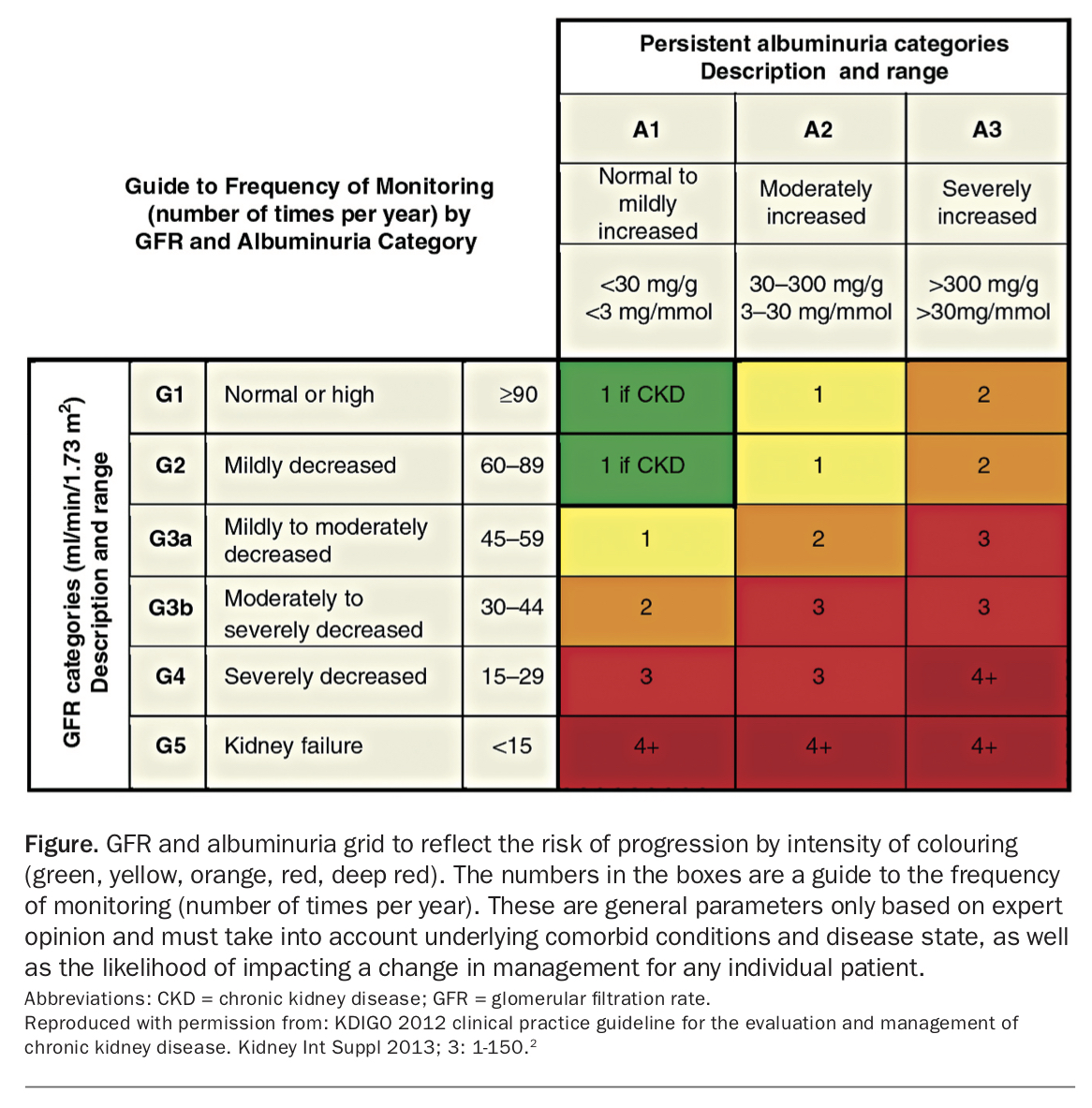
Albuminuria should also be used to detect CKD, as it independently increases the risk of progressive CKD and ESKD. Macroalbuminuria (uACR >30 mg/mmol) with an eGFR greater than 90 mL/min/1.73m2 triples the risk of progressive CKD, equivalent to the risk associated with an eGFR of 30 to 60 mL/min/1.73 m2 with no albuminuria.2 The Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group GFR and albuminuria grid reflects the risk of CKD progression based on colour intensity (Figure).2 The Kidney Health Australia Chronic kidney disease (CKD) management in primary care 2020 handbook has applied this grid to recommend clinical and laboratory assessments every 12 months for those at moderately increased risk, every three to six months for those at high risk and every one to three months for those at very high risk.9
{kind=link}
Once detected, an abnormal eGFR and/or uACR should be further evaluated by repeat electrolyte levels, spot uACR testing, urine microscopy, targeted history, examination including lying and standing blood pressure (BP), and medication review. Minor abnormalities often disappear after resolution of intercurrent illnesses, and thus represent reversible acute kidney injury rather than CKD.
Referral to specialist kidney care services
The KDIGO 2012 clinical practice guideline for the evaluation and management of CKD recommends referral to specialist kidney care services for the following situations:2
- acute kidney injury or an abrupt sustained fall in eGFR
- eGFR <30 mL/min/1.73m2
- consistent finding of significant albuminuria (uACR ≥30 mg/mmol or albumin excretion rate ≥300 mg/24 hours) or proteinuria (urine protein-creatinine ratio [uPCR] ≥50 mg/mmol or protein excretion rate ≥500 mg/24 hours)
- progression of CKD
– sustained decline in eGFR ≥25% from baseline
– sustained decline in eGFR >5 mL/min/1.73m2 per year - urinary red cell casts or persistent haematuria (RBC >20 per high power field) that is not readily explained
- CKD and hypertension refractory to treatment with four or more antihypertensive agents
- persistent abnormalities of serum potassium
- recurrent or extensive nephrolithiasis
- hereditary kidney disease.
Ultimately, these are guidelines that should be tailored to each patient. Early referral is associated with a 49% reduction in mortality compared with late referral.11 Validated clinical prediction tools such as the Kidney Failure Risk Equation (available online at https://kidneyfailurerisk.com), which calculates the two-year and five-year risk of ESKD based on four variables (age, sex, eGFR and uACR), can also be helpful in guiding decisions for referral.12
It is recommended that assessment before referral includes current and previous BP readings, current blood biochemical and haematological testing, uACR, urine microscopy for red cell morphology and casts, and a urinary tract ultrasound scan.9 The uACR measured using the first morning void is preferred as it reduces intraindividual variability compared with random urine samples and excludes orthostatic proteinuria.
The uACR is preferred to uPCR since uACR is more specific and sensitive for detecting glomerular disease. However, in multiple myeloma for example, the uACR can give misleadingly low readings and uPCR is preferred. Although urinalysis can be used to screen for proteinuria, it is insensitive, prone to false-positive results (e.g. concentrated urine or alkaline urine secondary to urinary tract infections) and is operator dependent. Detection of haematuria by urinalysis is sensitive but prone to false-positive results and should be confirmed with urine microscopy.2
Common clinical problems in CKD
BP control and increased CVD risk
Optimising BP control is the cornerstone in managing CKD and slowing its progression. It should involve addressing ‘traditional’ modifiable risk factors including salt restriction, smoking cessation, alcohol reduction and exercise. BP should be managed in the context of CVD risk. It is suggested that treatment should aim to lower BP towards:
- ≤140/90 mmHg for adults without CVD
- ≤130/80 mmHg for adults with diabetes, or with any level of albuminuria (uACR >2.5 mg/mmol for males; uACR >3.5 mg/mmol for females)13-16
- <120 mmHg in select patients with high cardiovascular risk who would tolerate more intensive BP control.17
When aiming for lower BP targets, patients should be monitored for adverse effects, including hypotension, syncope, electrolyte abnormalities and acute kidney injury. Antihypertensive agents such as ACE inhibitors or angiotensin receptor blockers (ARBs) are favoured in CKD due to their ‘renoprotective effects’ in lowering proteinuria. Patients should ideally be on maximal doses of these agents if there is marked proteinuria (uACR >85 to 100 mg/mmol, or more than 1 g protein excretion daily). However, at lower levels of albuminuria there is no additional benefit in maximising the dose of these agents, when BP is already controlled.18
A diuretic should be considered in the management of uncontrolled hypertension. Treatment-resistant hypertension, when three or more classes of antihypertensives including a diuretic are required, may warrant nephrologist input.19 In this case, there may be a role for a mineralocorticoid antagonist such as spironolactone. Treatment-resistant hypertension is more common in patients with CKD, among whom hyperaldosteronism may be under-recognised.19
Diabetic kidney disease
The increasing health burden of CKD is largely due to diabetic kidney disease, which is the leading cause of ESKD (38% of new cases) in Australia.5 ACE inhibitors or ARBs should form the cornerstone of management of diabetic kidney disease with microalbuminuria, as their use reduces the risk of ESKD by 23 to 28%.20,21 There is emerging evidence that cessation of ACE inhibitors or ARBs due to progression of CKD in patients with an eGFR less than 60 mL/min/1.73m2 is associated with an increased risk of death and cardiovascular events without any change in risk of ESKD.22 However, the combination of ACE inhibitors and ARBs should not be used in diabetic or nondiabetic kidney disease due to the higher risk of hyperkalaemia and acute kidney injury.23,24
More recently, sodium-glucose cotransporter 2 (SGLT-2) inhibitors (canagliflozin, dapagliflozin, empagliflozin and ertugliflozin) have become a useful addition to ACE inhibitors or ARBs in the management of patients with diabetic kidney disease with macroalbuminuria, who are at higher risk of CKD progression. SGLT-2 inhibitors have been shown to reduce the risk of ESKD, progression to macroalbuminuria and CVD.25-27 Adverse effects of SGLT-2 inhibitors include volume depletion, diabetic euglycaemic ketoacidosis, genital mycotic infection and lower-limb amputation.26,27 As with ACE inhibitors and ARBs, a modest (30% or less) initial drop in eGFR should not necessitate stopping SGLT-2 inhibitors, as it reduces the decline in eGFR in the long term.26,27 However, SGLT-2 inhibitors should be prescribed with caution in the context of the ‘triple whammy’ (ACE inhibitors/ARBs, diuretics and NSAIDs). Patients should be educated on a ‘sick day plan’ to withhold these medications during an intercurrent illness preventing adequate fluid intake, as well as before elective surgery.
Glucagon-like peptide-1 (GLP-1) agonists have also been shown to reduce the decline in eGFR, macroalbuminuria and cardiovascular events;28-31 however, studies powered for patient-level kidney endpoints such as reduction in ESKD have not yet been published. Use of weight-neutral or weight-losing diabetic therapies such as metformin, dipeptidyl peptidase-4 inhibitors (‘gliptins’) and injectable GLP-1 agonists is crucial to avoid exacerbating obesity; in contrast, sulfonylureas, glitazones and insulin promote weight gain and further insulin resistance.
Diet
Protein catabolism is prevalent in CKD and ESKD due to a chronic inflammatory state and metabolic acidosis.32 The prevalence of malnutrition in nondialysis-dependent CKD is as high as 41% and correlates with increased mortality.33 However, high protein intake increases the accumulation of uraemic toxins and may accelerate the progression of CKD. Therefore, a protein intake of 0.8 g/kg/day is recommended for adults with an eGFR <30 mL/min/1.73m2.2 For a 75 kg individual, this is equivalent to about 200 g of chicken breast, 300 g of salmon or 650 g of cooked lentils per day.34 CKD may be associated with hyperkalaemia and hyperphosphataemia, which if persistent may necessitate referral to a dietitian who can educate the patient regarding avoidance of foods high in potassium and phosphate. In particular, prevention of hyperkalaemia may facilitate continuation of ACE inhibitors or ARBs, which are renoprotective.
Dietary considerations for hypertensive patients include salt restriction. In adults, the recommended intake is less than 2 g/day of sodium (i.e. less than 90 mmol sodium, or less than 5 g of sodium chloride), unless contraindicated.2 Salt restriction can reduce systolic BP by up to 8 mmHg and diastolic BP by 3 mmHg.35 The Dietary Approach to Stop Hypertension (DASH) diet, which consists of four to five servings each of fruit and vegetables, two to three servings of low-fat dairy per day, and overall less than 25% fat, can further reduce systolic BP by up to 6 mmHg and diastolic BP by up to 3 mmHg depending on the degree of salt restriction.36 The potassium load associated with fruit may limit the use of this diet in patients with more advanced CKD.
Hyperuricaemia
Hyperuricaemia is associated with CKD, and recent evidence shows no added benefit in prescribing urate-lowering therapies in asymptomatic hyperuricaemia to slow the progression of CKD.37,38 Hyperuricaemia should therefore only be treated in patients with gout or urate calculi. Of note, patients with CKD may need to be cautiously initiated on lower doses of allopurinol but subsequently need higher maintenance doses of more than 300 mg daily to achieve target urate levels (less than 0.36 mmol/L; or less than 0.30 mmol/L for those with gouty tophi).
Other metabolic complications
Metabolic acidosis is a common complication of CKD and is associated with loss of bone and muscle mass and accelerated progression of CKD. Correction of metabolic acidosis in CKD with oral sodium bicarbonate may reduce its progression, lower serum potassium levels and improve nutrition without evidence of worsening hypertension, oedema or heart failure due to the additional sodium load.9,39,40
Anaemia and secondary hyperparathyroidism develop as eGFR declines below 60 mL/min/1.73m2 and become more prevalent with advanced CKD.41,42 Iron absorption is impaired in CKD due to chronic inflammation. Parenteral or oral iron supplementation can be used in the treatment of anaemia in CKD if the ferritin level is 500 mcg/L or less and transferrin saturation is 30% or lower, as maintaining high iron stores in CKD delays the need for erythropoiesis-stimulating agents or blood transfusions.43,44 The prescription of erythropoiesis-stimulating agents and management of secondary hyperparathyroidism with phosphate binders and vitamin D analogues requires specialist nephrology input and are beyond the scope of this review.
Conclusion
CKD is increasing in our community in the context of our ageing population and the increased incidence and prevalence of diabetes. There is a sound and growing evidence base for strategies allowing early detection of CKD and measures to delay progression to ESKD. Significant developments in the past few years, particularly in diabetic kidney disease, have been highlighted in this article. We anticipate that these developments will further reduce the burden of illness of people living with CKD. MT
References
1. Nugent RA, Fathima SF, Feigl AB, Chyung D. The burden of chronic kidney disease on developing nations: a 21st century challenge in global health. Nephron Clin Pract 2011; 118: c269-c277.
2. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013; 3: 1-150.
3. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease prevalence among Australian adults over time. Canberra: AIHW; 2018.
4. Australian Bureau of Statistics. National Health Survey: first results, 2017-2018. ABS cat. no. 4364.0.55.001. Available online at: https://abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4364.0.55.0012017-18?OpenDocument (accessed September 2020).
5. Australia and New Zealand Dialysis and Transplant Registry (ANZDATA). ANZDATA 42nd Annual Report 2019 (data to 2018). In: Chapter 1. Incidence of renal replacement therapy for end stage kidney disease. Adelaide: ANXDATA; 2019. Available online at: https://anzdata.org.au/report/anzdata-42nd-annual-report-2019 (accessed September 2020).
6. Australian Institute of Health and Welfare (AIHW). Incidence of end-stage kidney disease in Australia 1997-2013. AIHW Cat. no. PHE 211. Canberra: AIHW; 2016.
7. Kidney Health Australia (KHA). Pre-budget submission 2016-2017 Federal Budget. Charting a comprehensive approach to tackling kidney disease. Melbourne: KHA; 2017.
8. Consortium CKDP. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010; 375: 2073-2081.
9. Kidney Health Australia. Chronic kidney disease (CKD) management in primary care. 4th ed. Melbourne 2020.
10. Levey AS, Stevens LA, Schmid CH, et al; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med 2009; 150: 604-612.
11. Smart NA, Titus TT. Outcomes of early versus late nephrology referral in chronic kidney disease: a systematic review. Am J Med 2011; 124: 1073-1080. e1072.
12. Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of chronic kidney disease to kidney failure. JAMA 2011; 305: 1553-1559.
13. Go AS, Chertow GM, Fan D, McCulloch C, Hsu C. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 2004; 351: 1296-1305.
14. Sarnak MJ, Greene T, Wang X, et al. The effect of a lower target blood pressure on the progression of kidney disease: long-term follow-up of the modification of diet in renal disease study. Ann Intern Med 2005; 142: 342-351.
15. Agodoa LY, Appel L, Bakris GL, et al. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA 2001; 285: 2719-2728
16. Aggarwal R, Petrie B, Bala W, Chiu N. Mortality outcomes with intensive blood pressure targets in chronic kidney disease patients. Hypertension 2019; 73: 1275-1282.
17. SPRINT Research Group; Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015; 373: 2103-2116.
18. Cheung AK, Chang TI, Cushman WC, et al. Blood pressure in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2019; 95: 1027-1036.
19. Williams B, MacDonald TM, Morant S, et al; British Hypertension Society’s PATHWAY Studies Group. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet 2015; 386: 2059-2068.
20. Brenner BM, Cooper ME, De Zeeuw D, et al; for the RENAAL Study Investigators. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001; 345: 861-869.
21. Lewis EJ, Hunsicker LG, Clarke WR, et al; for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 2001; 345: 851-860.
22. Qiao Y, Shin J-I, Chen TK, et al. Association between renin-angiotensin system blockade discontinuation and all-cause mortality among persons with low estimated glomerular filtration rate. JAMA Intern Med 2020; 180: 718-726.
23. Fried LF, Emanuele N, Zhang JH, et al; for the VA NEPHRON-D Investigators. Combined angiotensin inhibition for the treatment of diabetic nephropathy. N Engl J Med 2013; 369: 1892-1903.
24. The ONTARGET Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008; 358: 1547-1559.
25. Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med 2016; 375: 323-334.
26. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017; 377: 644-657.
27. Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 2019; 380: 2295-2306.
28. Tuttle KR, Lakshmanan MC, Rayner B, et al. Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7): a multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol 2018; 6: 605-617.
29. Marso SP, Daniels GH, Brown-Frandsen K, et al; LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016; 375: 311-322.
30. Gerstein HC, Colhoun HM, Dagenais GR, et al; REWIND Investigators. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet 2019; 394: 121-130.
31. Marso SP, Bain SC, Consoli A, et al; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016; 375: 1834-1844.
32. Lim VS, Kopple JD. Protein metabolism in patients with chronic renal failure: role of uremia and dialysis. Kidney Int 2000; 58: 1-10.
33. Chan M, Kelly J and Tapsell L. Dietary modeling of foods for advanced CKD based on general healthy eating guidelines: what should be on the plate? Am J Kidney Dis 2017; 69: 436-450.
34. US Department of Agriculture Agricultural Research Service. FoodData Central. Available online at: https://fdc.nal.usda.gov (accessed September 2020).
35. Graudal NA, Hubeck‐Graudal T, Jurgens G. Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride. Cochrane Database Syst Rev 2017; (4): CD004022.
36. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med 2001; 344: 3-10.
37. Badve SV, Pascoe EM, Tiku A, et al. Effects of allopurinol on the progression of chronic kidney disease. N Engl J Med 2020; 382: 2504-2513.
38. Doria A, Galecki AT, Spino C, et al. Serum urate lowering with allopurinol and kidney function in type 1 diabetes. N Engl J Med 2020; 382: 2493-2503.
39. de Brito-Ashurst I, Varagunam M, Raftery MJ, et al. Bicarbonate supplementation slows progression of CKD and improves nutritional status. J Am Soc Nephrol 2009; 20: 2075-2084.
40. Di Iorio BR, Bellasi A, Raphael KL, et al. Treatment of metabolic acidosis with sodium bicarbonate delays progression of chronic kidney disease: the UBI Study. J Nephrol 2019; 32: 989-1001.
41. Hsu C-y, McCulloch CE, Curhan GC. Epidemiology of anemia associated with chronic renal insufficiency among adults in the United States: results from the Third National Health and Nutrition Examination Survey. J Am Soc Nephrol 2002; 13: 504-510.
42. Isakova T, Wahl P, Vargas GS, et al. Fibroblast growth factor 23 is elevated before parathyroid hormone and phosphate in chronic kidney disease. Kidney Int 2011; 79: 1370-1378.
43. McMurray JJ, Parfrey PS, Adamson JW, et al. Kidney disease: Improving global outcomes (KDIGO) anemia work group. KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl 2012; 2: 279-335.
44. Macdougall IC, Bock AH, Carrera F, et al. FIND-CKD: a randomized trial of intravenous ferric carboxymaltose versus oral iron in patients with chronic kidney disease and iron deficiency anaemia. Nephrol Dial Transplant 2014; 29: 2075-2084.