Noisy breathing in children. When to be concerned

Noisy breathing in children can be concerning for both parents and clinicians. The aetiology may not be easily apparent on office assessment. Having a systematic approach and understanding potential pathologies can help differentiate which children require referral.
- Most children breathe comfortably and quietly both awake and asleep. If present, airway noise can indicate the presence of either a static or dynamic obstruction.
- Assessment of noisy breathing in children begins with questions about the onset, severity and progression of the noise, associated features, history of previous intubation and the possibility of a foreign body.
- General inspection, listening to the sound and how it correlates with respiration, and examining the nose, oral cavity, neck and chest can help localise the region of pathology.
- The nasal cavity, oral cavity, larynx and trachea are potential sources of various airway noises and presentations. Correlating the site with age, acuity of onset and associated symptoms narrows the differential diagnosis.
- Consider referral to an ENT surgeon for anatomical assessment and potential intervention if there is persistent noisy breathing, especially if associated with parental anxiety, difficulty feeding, slow weight gain or increased work of breathing.
- Refer to the emergency department if there are prolonged apnoeas, dusky episodes or blue spells when the child is awake or asleep, or if there is concern about a foreign body, especially a button battery.
Few clinical presentations generate more anxiety than a child with noisy breathing. In infants particularly, this may raise concern about respiratory arrest and even sudden infant death syndrome (SIDS). The challenge for clinicians is that a range of pathologies present with airway noise and office examination may not yield an obvious diagnosis. In some children, noisy breathing is only present intermittently and not witnessed during review. Parental reports may be subjective and it can be difficult to distinguish between children who have self-limiting conditions and children who require referral and further intervention.
This article reviews the assessment of a child with noisy breathing, provides a systematic framework for differential diagnosis of common airway pathologies, and outlines when a child requires referral to an ear, nose and throat (ENT) surgeon or even the emergency department.
Assessing a child with noisy breathing
Key paediatric airway history questions
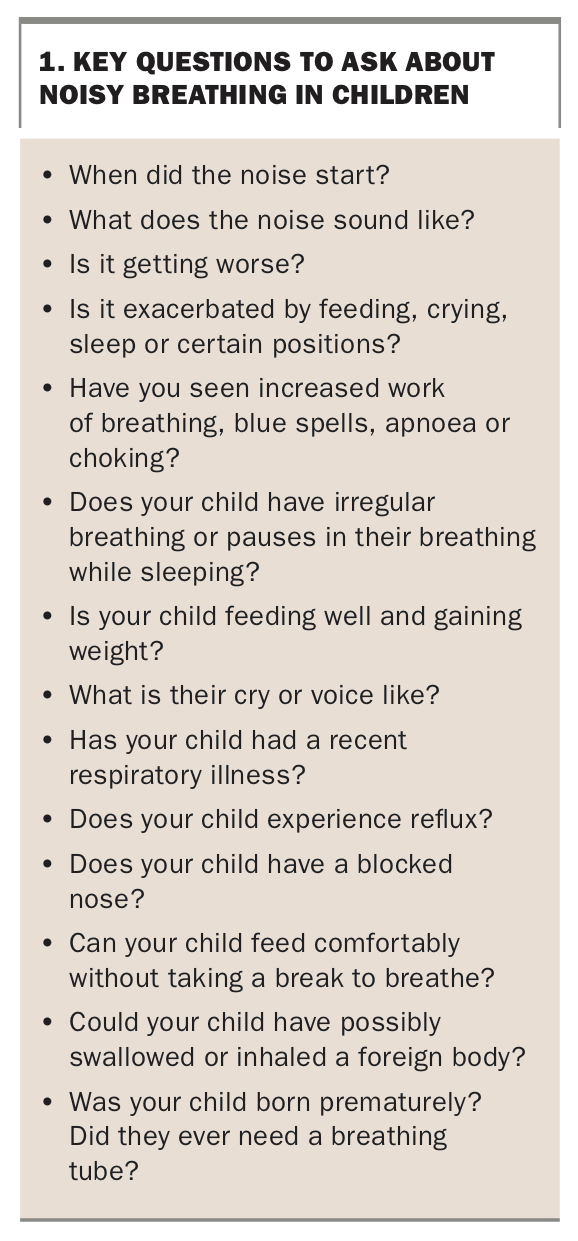
When taking a history about noisy breathing, it is important to gauge the onset, severity and progression of the noise, as well as other associated features, such as impact on feeding, sleep disturbance, unusual cry, work of breathing and occurrence of blue spells or apnoeic episodes. A neonatal history provides significant context if the child was born prematurely and had required previous intubation (Box 1). In older children, asking about the possibility of an ingested or inhaled foreign body may be crucial in directing management.
{kind=link}
Examination of the child with noisy breathing
Audible respiration indicates the presence of airway obstruction generating turbulent airflow and noise. Some conditions have hallmark descriptions, although the correlation between breathing sounds and diagnosis is not always accurate. Many parents have smartphone video and audio recordings demonstrating examples of their child’s noisy breathing, and these can be an invaluable adjunct during assessment.
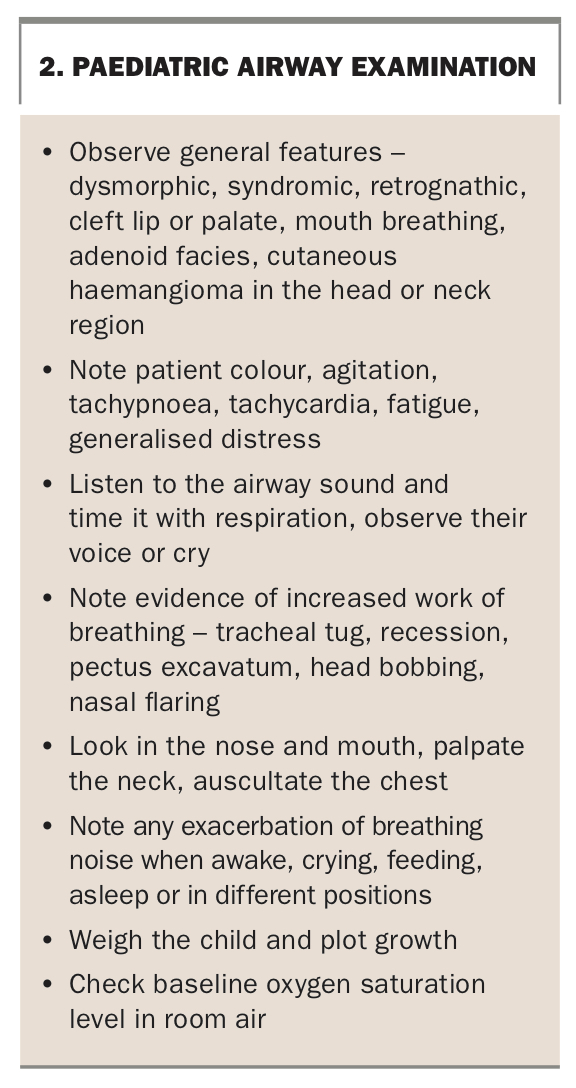
General inspection provides some clues about the source and severity of the obstruction (Box 2). This includes paying attention to craniofacial features, preference for mouth breathing, increased respiratory effort, sound of the voice or cry and degree of overall distress. These may change depending on whether the child is awake, upset, feeding, sleeping or in different positions. A cutaneous haemangioma in the head and neck region should be noted because this can be associated with an airway haemangioma.
{kind=link}
Timing the noise with the phase of breathing may be useful in determining the level of the pathology. Inspiratory noise can signify pathology above the vocal cords (supraglottic), biphasic noise can signify pathology at the level of the vocal cords or just below (glottic or subglottic), and expiratory noise tends to signify pathology of the trachea or lower smaller airways (intrathoracic).
Multiple terms are used to describe noisy breathing. Snorting and snuffliness suggest nasal congestion. Stertor is a low-pitched sound, like a snore, which can occur awake or asleep. It can originate from the nose, nasopharynx or oropharynx and may have a deep vibratory quality. Stridor tends to be high-pitched, squeaky and harsher sounding, and can be predominantly inspiratory in cases of laryngomalacia, or even biphasic with croup or vocal cord pathology.1 Wheezing is also high-pitched but with a musical quality. It tends to be expiratory and is associated with narrowing of the smaller airways of the lungs. These terms will not neatly fit many children’s breathing noises, as the sounds can vary in different situations and there may be more than one level of pathology, which can make interpretation difficult. Some children with significant obstruction can also have surprisingly few symptoms or signs.
Nasal airflow is assessed by observing misting of a mirror or metal speculum held under the nose and looking into the nasal cavity with a light. The oral cavity and neck should be checked for any masses and the chest auscultated for added sounds or diminished airflow. Weighing the child and plotting their growth will show whether increased respiratory effort is affecting their ability to thrive. Respiratory rate, observation for signs of increased work of breathing and oxygen saturation level should be assessed. Tachypnoea and a low baseline oxygen saturation level may indicate a more severe degree of obstruction.
Investigations to consider
The workup for children with noisy breathing is dictated by their age, associated symptoms and severity of their presentation. Referral to an ENT surgeon for examination with flexible fibreoptic nasendoscopy and laryngoscopy in the office may yield or exclude a diagnosis in children who are able to tolerate the procedure. If there is concern about pathology below the level of the vocal cords then a diagnostic assessment under general anaesthesia may be recommended (laryngoscopy, bronchoscopy and even oesophagoscopy).
A nasopharyngeal swab for respiratory viruses can be helpful in the setting of upper respiratory tract symptoms. Referral to a sleep medicine specialist for overnight pulse oximetry or full polysomnography is appropriate for children with sleep-predominant symptoms. A few paediatric ENT specialists offer drug-induced sleep endoscopy to help identify dynamic airway changes that are not apparent in the awake state. Spirometry, lung function and exercise testing are not performed in the early childhood years but can be attempted in older children if appropriate.
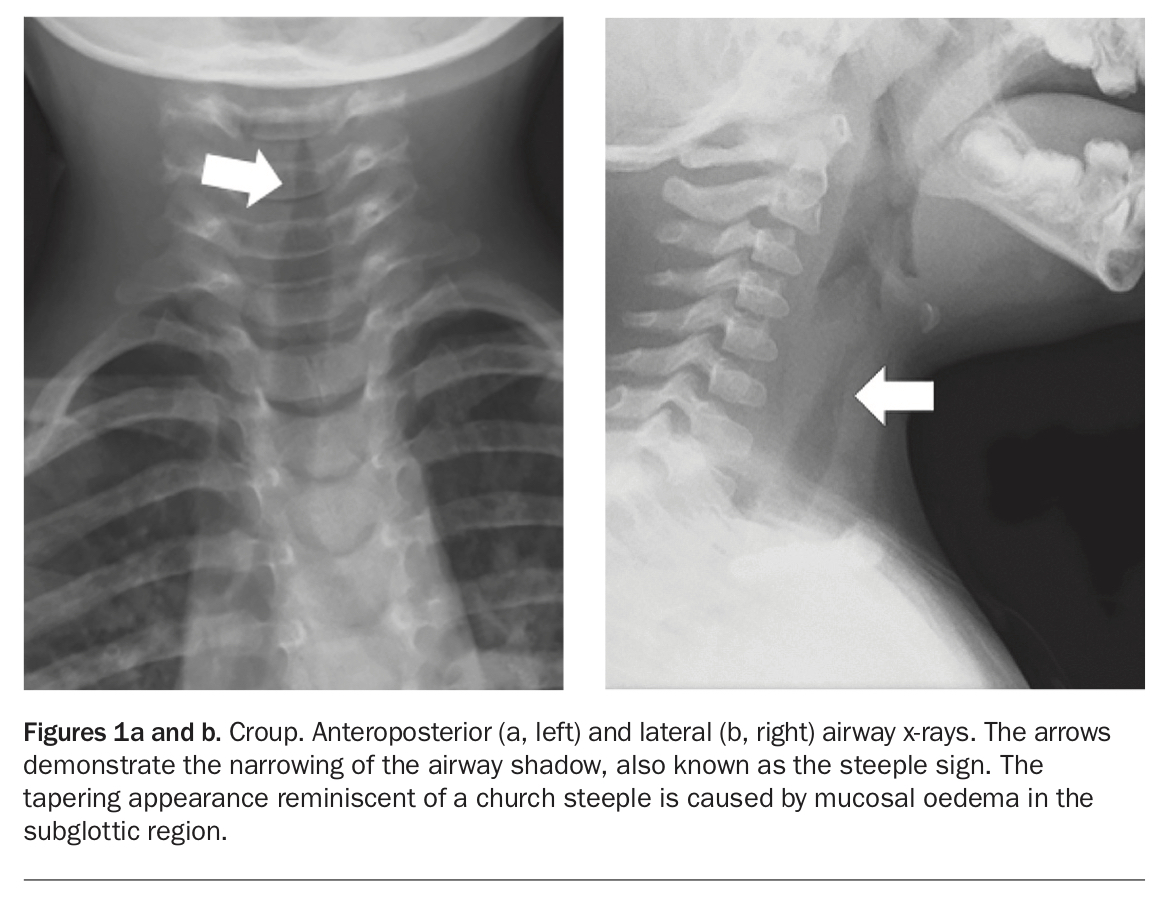
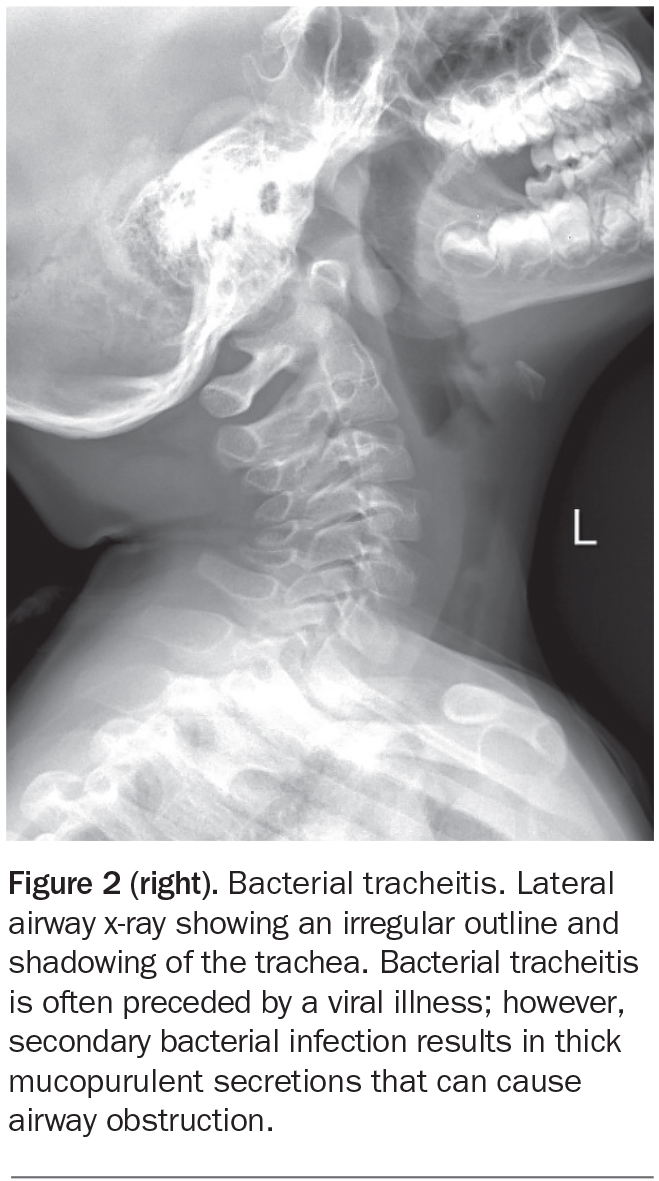
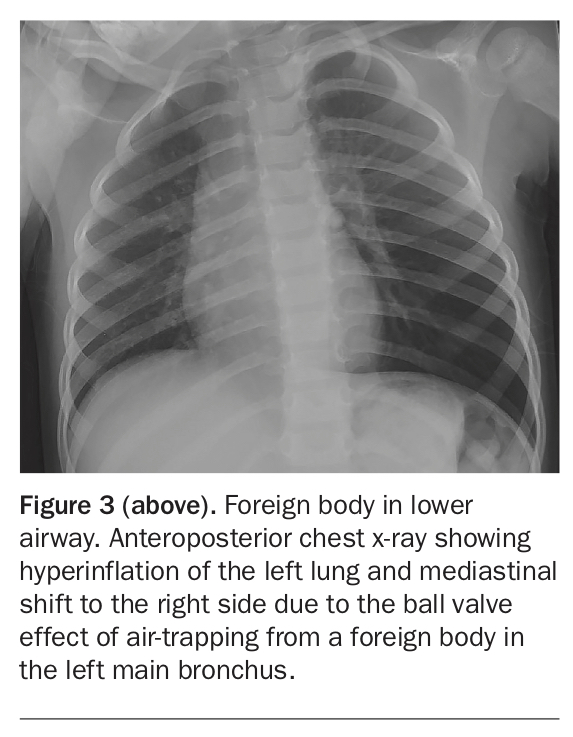
Radiological studies may be considered, depending on access to ENT services, but are not routinely ordered. A lateral airway x-ray can assist in the diagnosis of adenoid hypertrophy, croup (Figures 1a and b), bacterial tracheitis (Figure 2), foreign bodies and epiglottitis. A chest x-ray can help diagnose an inhaled foreign body or lower respiratory illness (Figure 3). A barium swallow may be indicated in patients with swallowing or suspected aspiration issues that are present in addition to the noisy breathing. Upper airway fluoroscopy has become less common as fibreoptic technology has improved and awareness about childhood exposure to radiation has increased. CT pulmonary angiography and thoracic MRI are generally reserved to delineate cardiovascular anatomy and intrathoracic pathology only after other first-line investigations have been performed.
{kind=link}
{kind=link}
{kind=link}
Differential diagnosis of paediatric airway noise
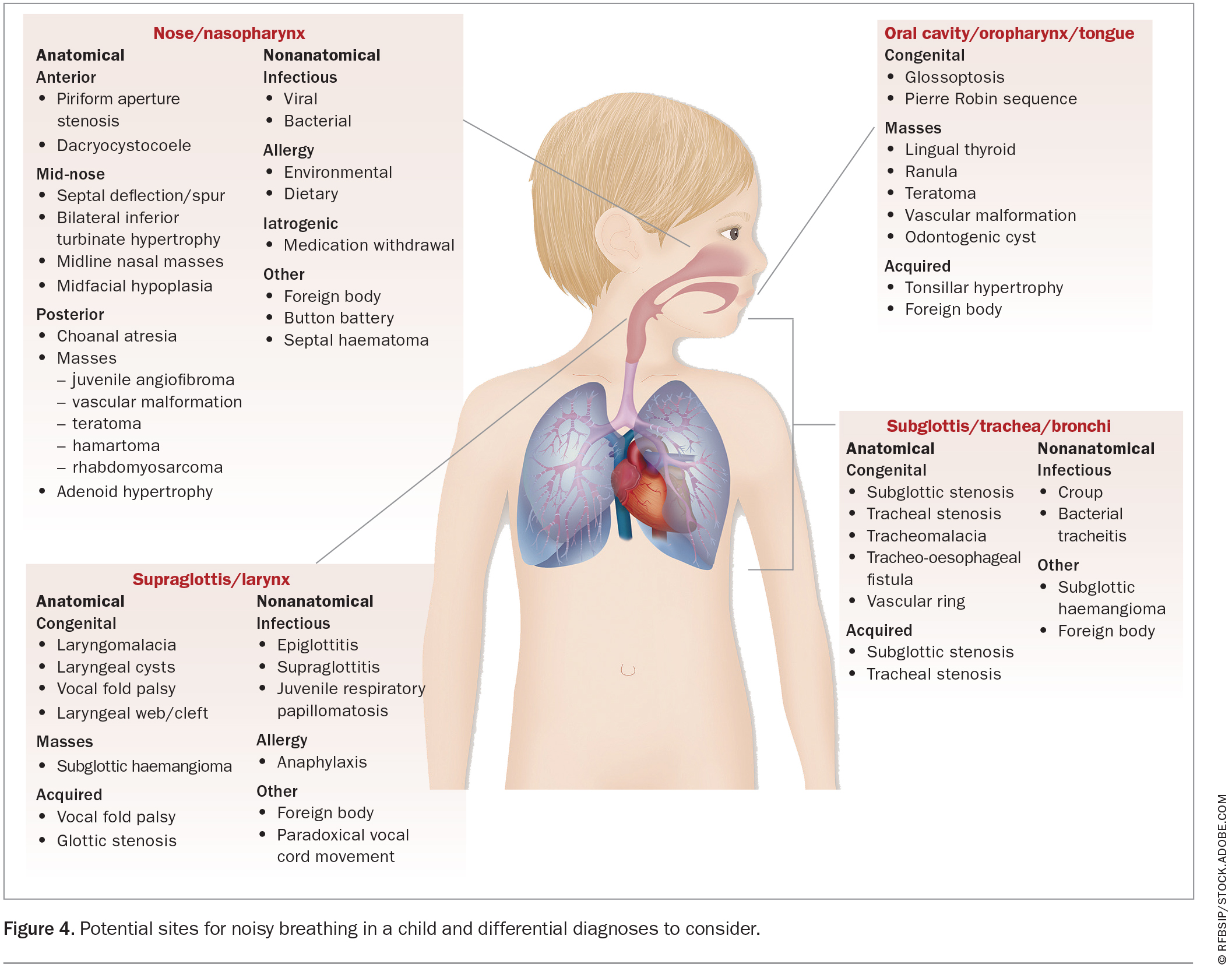
A systematic approach considering four regions (nasal, oral, laryngeal and tracheal) can help focus the differential diagnosis of noisy breathing in children (Figure 4) and guide recommendations for intervention. Some conditions are due to static anatomical obstruction, whereas others are dynamic. An appreciation of the timing of symptom onset is also essential, as certain pathologies are more likely to affect different age groups.
{kind=link}
Nose and nasopharynx
The nose and nasopharynx are common sites of obstruction throughout childhood. This can be intermittent due to mucosal congestion in response to infectious, inflammatory or allergic triggers, or more persistent if there is a structural lesion affecting the septum, nasal cavity, choanae or postnasal space.2 Noisy breathing from this area may be described as mucousy, snorting or snuffling with an almost porcine quality, and is often worse with oral intake or sleep. It can be distressing for neonates and young infants who are preferential nasal breathers, due to interference with their ability to co-ordinate sucking, swallowing and respiration. In older children, signs of nasal obstruction include chronic mouth breathing, transverse nasal crease from perpetual nose rubbing, allergic shiners, rhinorrhoea, hyponasal voice (sounding sick with a cold) and even craniofacial changes with a long face, open mouth, short upper lip, prominent upper teeth, high-arched palate and dental crowding.
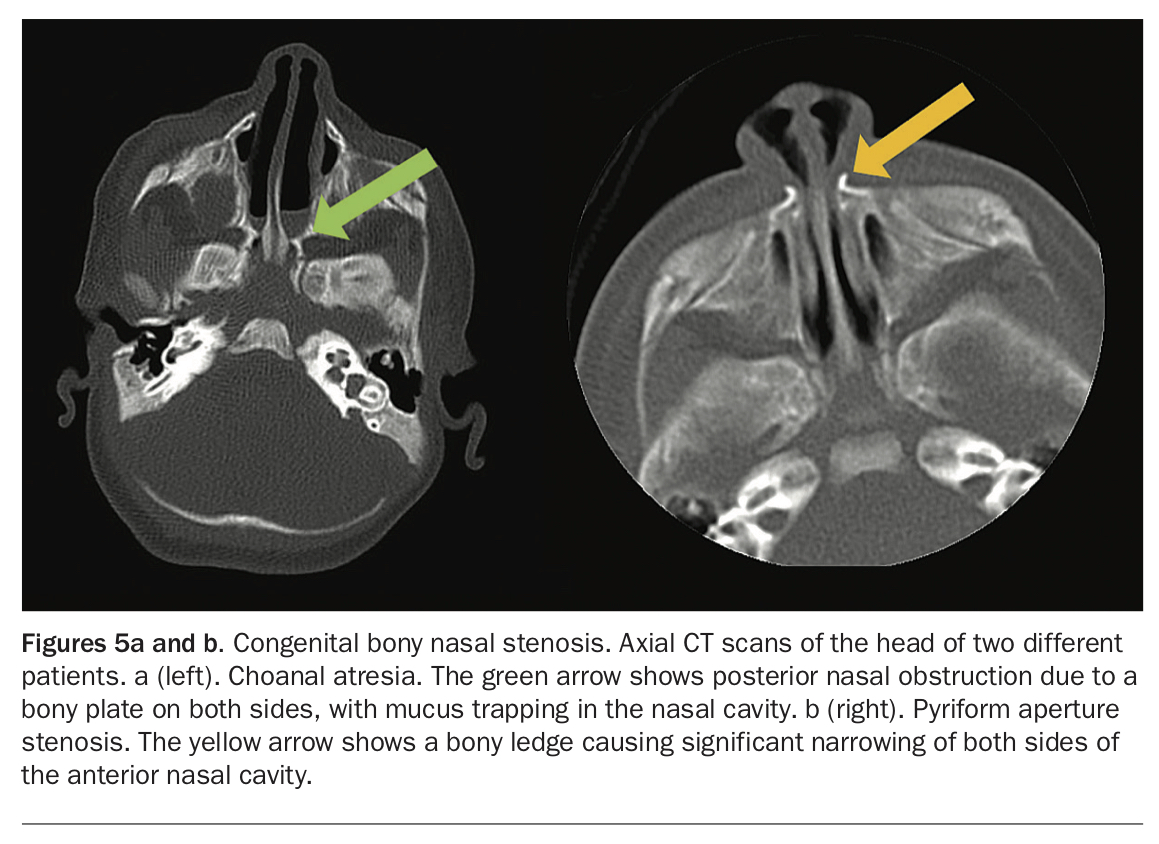
Congenital septal deviation can create bony or cartilaginous nasal obstruction.In choanal atresia (Figure 5a), the posterior internal nostrils are completely occluded by bone, whereas in pyriform aperture stenosis (Figure 5b), bony ledges narrow the anterior nose. Soft tissue obstruction can arise from a blocked nasolacrimal duct system or masses such as dermoid cysts, encephalocoeles or gliomas associated with congenital skull base defects.
{kind=link}
In older children, rhinitis from viral exposure or a sensitivity to environmental aeroallergens is a frequent cause of turbinate congestion. Adenoid hypertrophy is at its greatest between 12 months and 7 years of age, but can also be seen in younger babies and in some teenagers, occasionally persisting into adulthood.2 Consider a septal haematoma in the context of nasal trauma, even if time has lapsed from the original insult. Similarly, insertion of a nasal foreign body may have been unwitnessed and might be only discovered during clinical examination.
Oral cavity and oropharynx
The oral cavity and oropharynx are easier to illuminate and directly visualise than the nose and nasopharynx. Noisy breathing generated from this level results from vibration of the soft tissue structures. It is variably pitched and can be described as snoring, fluttering, purring, choking or gasping. Older children may have a muffled sound quality when they speak, likened to a person having very hot potato in their mouth.
Tonsillar hypertrophy is the most common cause of airway obstruction in the oropharynx region and can be associated with significant sleep disordered breathing and apnoea.3 Infections from the tonsils can spread to the peritonsillar tissues with associated soft palate swelling and uvula deviation (quinsy), or to other deeper neck spaces, with abscess formation sometimes indicated by lateral pharyngeal wall bulging. A lingual thyroid or mucocoele may be located towards the tongue base.
Pierre Robin sequence or syndrome is a congenital birth defect characterised by micrognathia and glossoptosis that is usually (but not always) associated with a cleft palate. This can cause significant airway obstruction in infancy, especially when the child is supine, due to tongue-base prolapse. A recessed mandible or retrognathia alone in some children causes a similar effect. Hypotonia in neuromuscular conditions can contribute to the palate, pharyngeal walls and tongue base collapsing, which can be compounded by reduced co-ordination of secretions.
Supraglottis and larynx
The supraglottis and larynx are important sites for airway obstruction, especially in the neonatal and infant age groups. Sounds generated from this area are typically described as high-pitched, inspiratory and squeaky, and often worse during times of increased oxygen requirement, such as when feeding or unsettled. An unusual cry or voice can be associated if the vocal cords are involved.
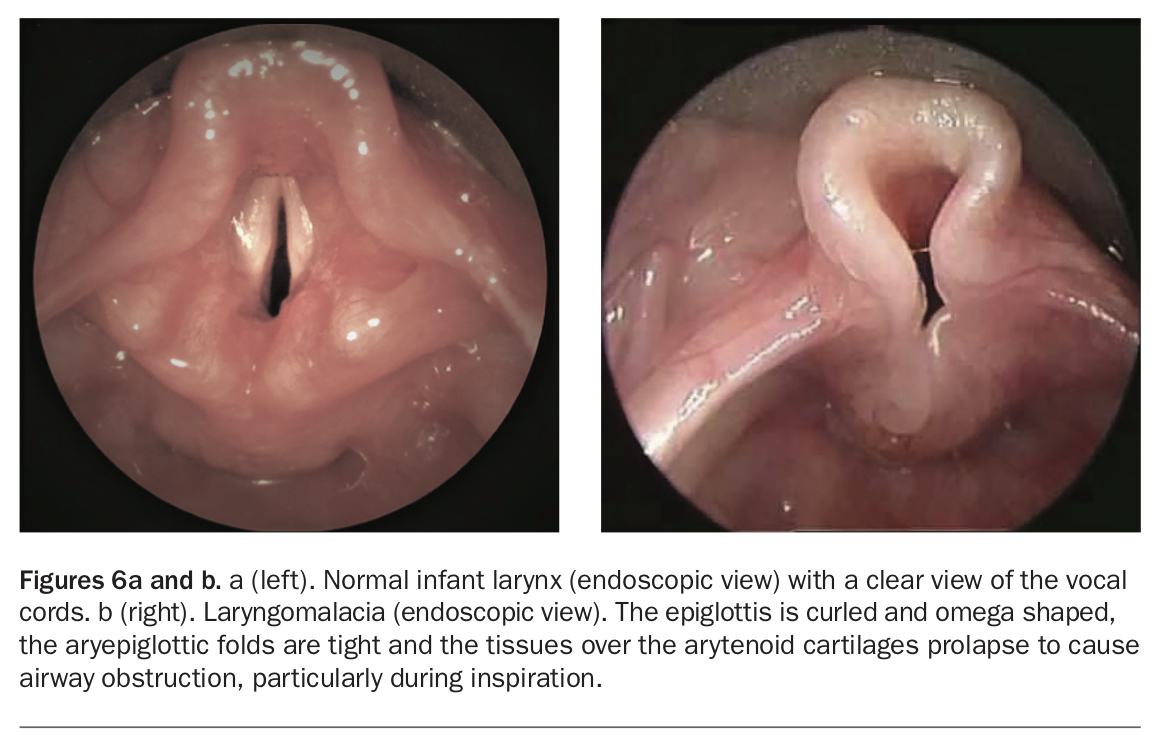
Laryngomalacia is the most common cause of inspiratory stridor in neonates.4 It is caused by dynamic collapse of the epiglottis and tissues around the arytenoid cartilages covering the laryngeal opening (Figures 6a and b) and is exacerbated by gastro-oesophageal reflux.4 Unilateral vocal cord palsy may present with airway noise, coughing with liquids and a weak, hoarse or breathy cry.5 Children with bilateral vocal cord palsy may have a surprisingly strong cry if the resting position of the vocal cords is close to midline, and predominantly present with airway compromise.5 Obstructed mucous glands, which cause cystic swellings around the supraglottis and larynx, are benign but can have significant impact, depending on their location. With a laryngeal cleft, there is deficient tissue between the larynx and upper oesophagus, often resulting in aspiration and sometimes airway noise.
{kind=link}
A foreign body lodged in the upper airway or oesophagus is a possible cause of noisy breathing if there has been a relatively short history of the condition, especially without other illness. Epiglottitis has diminished over recent years due to Haemophilus influenzae type B immunisation; however, respiratory tract pathogens other than Haemophilus may still cause supraglottic inflammation and airway distress. Juvenile-onset respiratory papillomatosis is a differential diagnosis in children with an altered voice quality. Vocal cord dysfunction causing paradoxical adduction on inspiration can be confused with asthma and can cause significant distress in older children.
Subglottis, trachea and main bronchi
Obstruction in the subglottis, trachea and main bronchi can be hard to clinically differentiate. The sounds range from inspiratory stridor caused by subglottic narrowing, through to biphasic, expiratory, coarse and variably pitched noises with distal lesions. Descriptions include barking, croupy, rattly, vibratory, wheeze and sounding like a seal. A prominent, deep-sounding cough from the lower airway walls reverberating with trapped mucus may draw attention to the child from passers-by. Unlike the other regions described, this area generally requires an assessment under general anaesthetic for diagnosis confirmation.
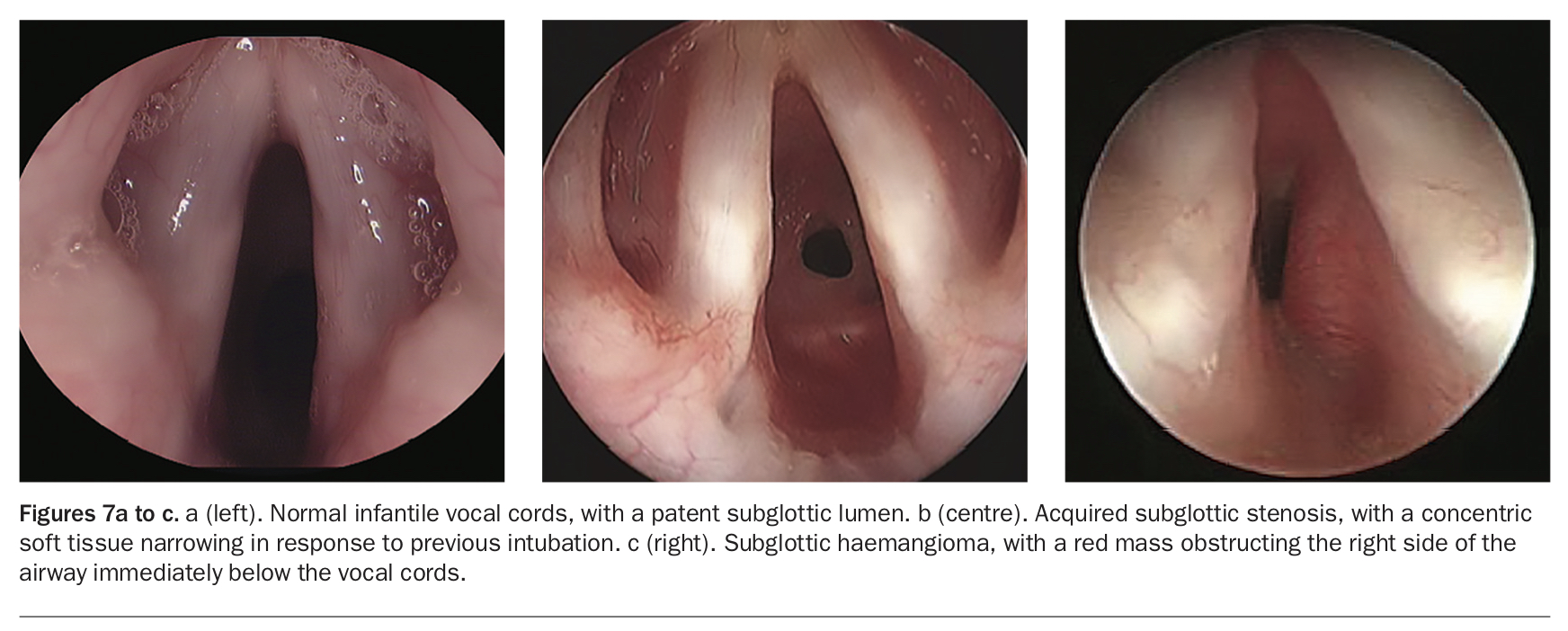
Congenital subglottic stenosis is due to a narrow formation of the cricoid cartilage, whereas acquired subglottic stenosis is commonly from previous intubation and soft tissue scarring (Figures 7a and b).6 The most frequent cause of subglottic noise is croup (viral laryngotracheo-bronchitis), to which children with an underlying airway narrowing can be more predisposed. A subglottic haemangioma (Figure 7c) may produce relatively sudden symptoms and be mistaken for croup as it causes a narrowing in a similar site and is corticosteroid responsive.
{kind=link}
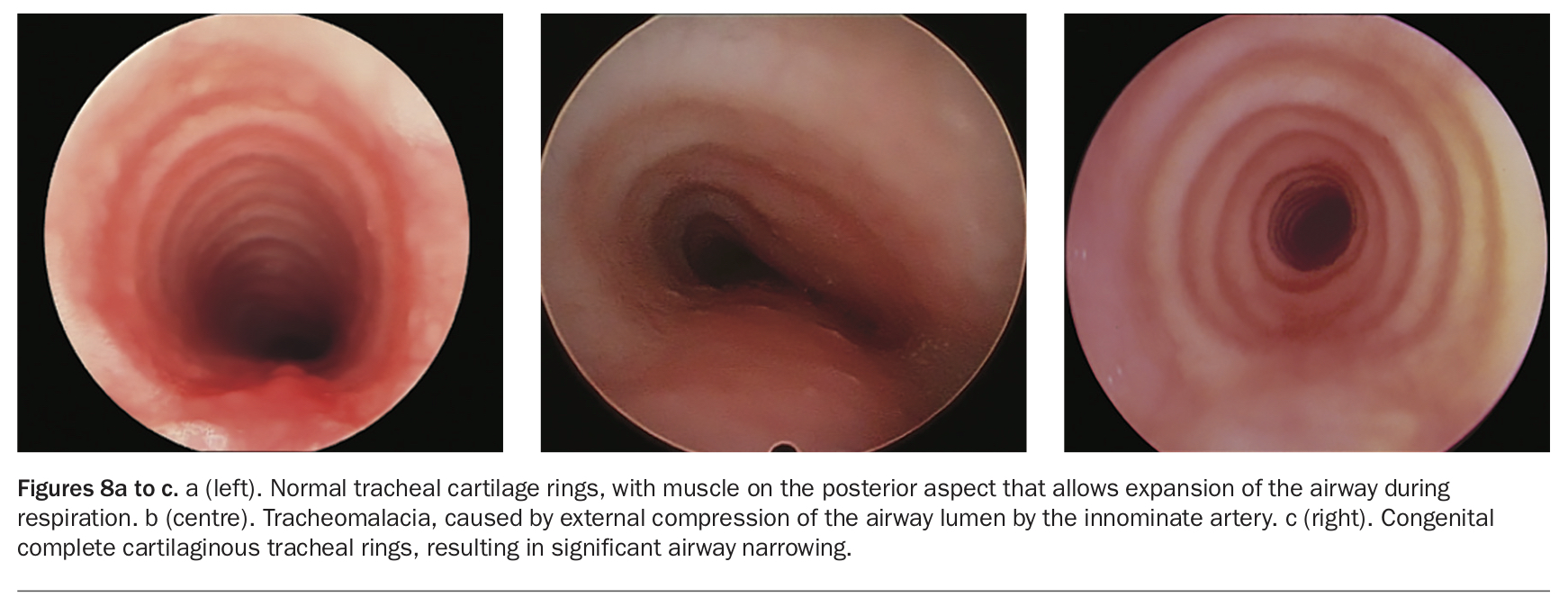
Tracheomalacia, the collapse of the tracheal cartilages, can occur with other congenital abnormalities such as tracheo-oesophageal fistula, or secondary to external compression from the major cardiac vessels. Tracheal stenosis, on the other hand, can be due to complete tracheal rings of cartilage with absent posterior wall muscle, limiting natural airway expansion and secretion clearance (Figures 8a to c).6 The infection bacterial tracheitis is associated with significant airway secretions and toxicity.
{kind=link}
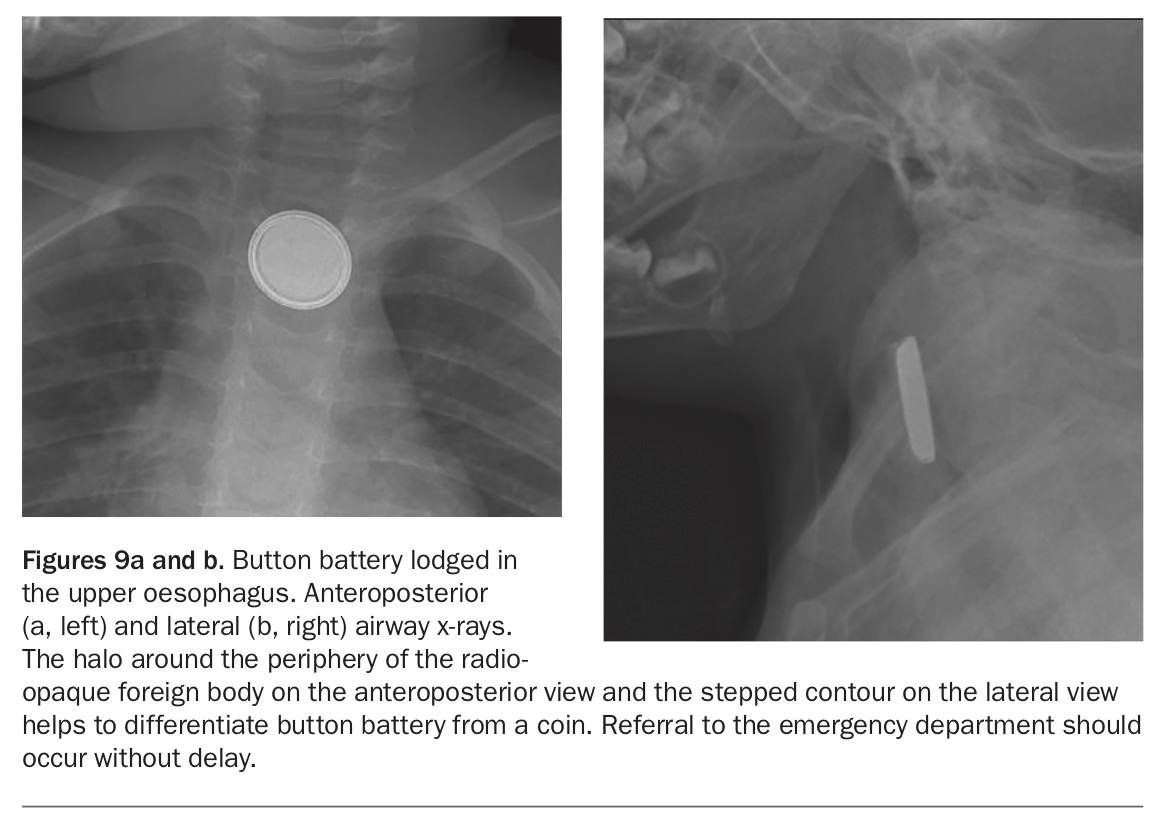
An inhaled foreign body should be suspected in children under 5 years of age who are systemically well with short onset of cough, wheeze or decreased breath sounds. Button battery ingestion is a time-critical emergency because of the caustic burn and perforation that is quickly induced on mucosal contact (Figures 9a and b).7,8
{kind=link}
Timing of symptom presentation
The patient’s age and timing of symptom onset is important, as certain diagnoses for children with noisy breathing have a pattern of presentation. Noisy breathing evident from birth raises suspicion for a congenital malformation or craniofacial abnormality. Laryngomalacia will usually become symptomatic within the first two weeks of life, as the infant starts to have more awake time. A subglottic haemangioma, however, may be similar to infantile cutaneous haemangioma and not grow until the infant is a few months of age.
Tracheomalacia may cause more symptoms when the child commences solid intake, due to indentation of the bolus through the oesophagus on the adjacent posterior tracheal wall, or when there is increased activity and oxygen requirement from crawling or walking. Croup is unusual in infants under 6 months of age, however some children may have early viral exposure from day-care attendance or older siblings.
Foreign body ingestion generally requires a degree of fine motor skill to pick up a small object, although choking and aspiration of oral intake can happen at any age. Other infections and adenotonsillar hypertrophy tend to become more symptomatic after 12 months of age.
When to be concerned
It is not unusual for some newborns to sound noisy and full of mucus for the first few weeks of life. They may have periodic breathing with an inconsistent rhythm that improves spontaneously with increasing maturity. Intermittent grunting sounds are heard in many normal infants and can be related to their small airways, nasal secretions, salivary clearance, digestion, colic and wind.
Airway noises that are persistent over several breaths for prolonged periods, however, warrant further review, particularly if there is parental anxiety, difficulty feeding, slow or poor weight gain, increased work of breathing, apnoeas, dusky episodes or blue spells. Pectus deformity and signs of cor pulmonale are worrying signs. In older children, concern should be raised if there are symptoms of aspiration, sleep-disordered breathing, deterioration with respiratory illness, recurrent croup, exercise limitation or possible foreign body inhalation or ingestion, especially of a button battery.
The role of the GP is to help determine the children who require immediate referral to the emergency department and those who would benefit from semiurgent or routine review by an ENT surgeon, general paediatrician, sleep medicine physician or respiratory medicine physician. Referral to a tertiary centre with specialised paediatric ENT services is often necessary for anatomical assessment and treatment, depending on the patient’s age and associated symptoms.
Conclusion
A thorough history, observation of the child and their airway noise, consideration of the anatomical level of obstruction and correlation of this with age can aid in demystifying noisy breathing in children. Airway presentations associated with respiratory distress, failure to thrive, apnoea, foreign body suspicion or anatomical obstruction should be referred to an ENT surgeon, the urgency of any referral being dependent on the acuity and severity of the presentation. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.