Managing hallux rigidus – every step of the way

Hallux rigidus is a painful arthritic condition of the great toe, with even mild disease causing functional limitation. Fortunately, it can be managed effectively.
Hallux rigidus (‘great toe arthritis’) is one of the most common arthritic conditions of the foot, presenting as pain and stiffness in the metatarsophalangeal joint (MTPJ). It has a bimodal presentation, commonly presenting in patients aged in their 50s or 60s and less commonly in young athletic patients after ligament trauma.1,2 The condition is progressive in nature and early symptoms can be managed nonoperatively; however, many patients seek surgical intervention as symptoms progress.3
The great toe has an important role in foot biomechanics and even mild radiological arthritis can be functionally limiting for a patient. Good range of motion (ROM) of the great toe is important to allow adequate push off, with an arc of movement of the first MTPJ of 110 degrees, which includes 75 degrees of dorsiflexion.4 The medial column of the foot and the great toe form one of the three points of contact with the ground, with the great toe taking twice the pressure of the other four toes.5-7
Clinical presentation and assessment
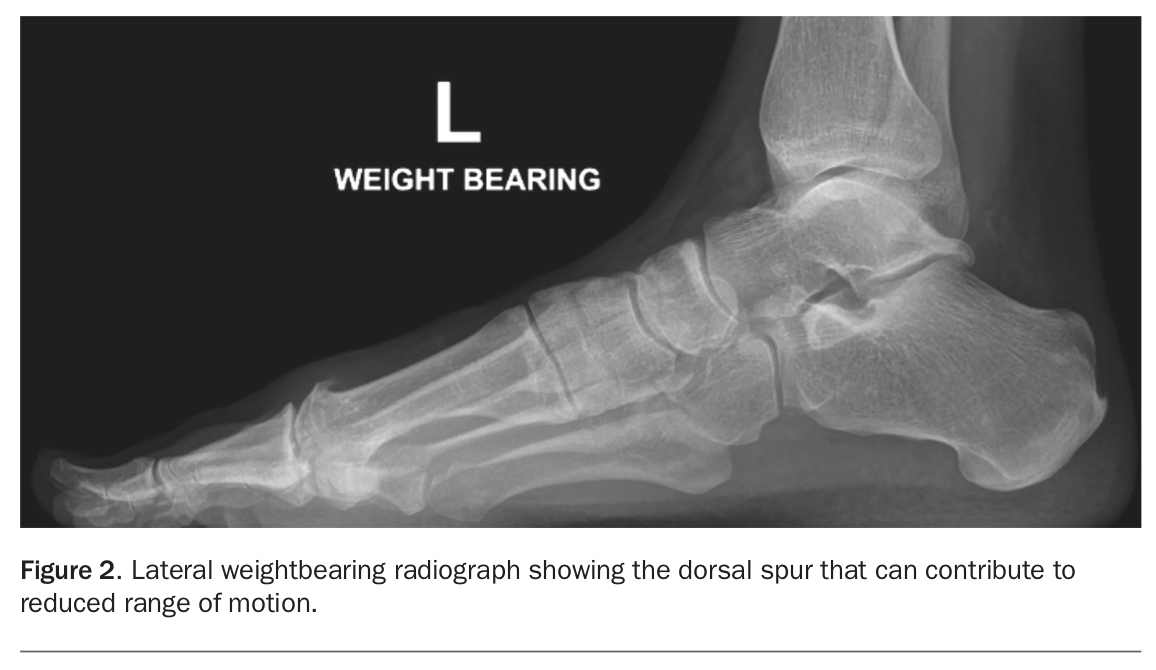
The presentation of hallux rigidus is often insidious onset of an aching pain in the first MTPJ. Commonly a patient will present with a lump on the dorsal great toe and a ‘bunion’ and be surprised to learn that hallux rigidus is the diagnosis (Figures 1a and b). This is caused by osteophyte formation and is not a true bunion deformity (Figure 2). Symptoms are usually local to the first MTPJ, with pain that is aggravated during the push off phase of gait and often worse when high-heeled shoes are worn because of the increased dorsiflexion required.
{kind=link}
{kind=link}
Palpation often localises the tenderness to the first MTPJ, especially dorsally (more than on the plantar aspect) due to the spur that impinges in dorsiflexion. Hallux rigidus leads to a short stance phase or external rotation of the lower leg and foot to reduce the pain of MTPJ dorsiflexion during ‘toe off’. Examination of the patient’s shoes may reveal lateral wearing as a result of compensatory unloading of the great toe.
It can be helpful to perform the grind test by applying an axial load through the first MTPJ – if this elicits pain then central chondral wear and advanced disease is implied. The examination should include a review of the joints above and below (i.e. ankle, midfoot and interphalangeal joints) and tendon insertion and function, as well as a neurovascular assessment.
Investigations
Investigations to order in the first instance for a patient with suspected hallux rigidus are standard weightbearing AP/lateral with supine oblique x-rays. This is often the only imaging required prior to referral to a specialist centre. CT can be beneficial in assessing subchondral bone prior to surgical intervention and MRI can be useful in assessing soft tissue structures, but both are generally not necessary with standard presentations.8
The differential diagnoses of hallux rigidus include gout, rheumatic disorders and hallux valgus; in addition, there are important spinal conditions radiating to the foot that should not be missed, such as L5 radiculopathy. Pathology tests may be helpful – these include uric acid (for gout) and C-reactive protein and rheumatoid factor levels (for inflammatory arthropathies). If results of these raise concerns then a joint aspirate can be performed to further clarify the pathology.
Grading
The grading system for hallux rigidus is based on ROM, radiological changes and clinical findings, with increasing severity associated with reducing ROM, increasing pain and increasing osteophytes and joint space narrowing.9 There is, however, a lack of correlation between symptom severity and radiographic changes.10
Management
Initial management of hallux rigidus is nonoperative. Footwear should be accommodative, with a large toe box (area for the forefoot) and a stiff sole to reduce motion of the great toe during gait. We recommend involving a good podiatrist who can suggest appropriate shoe brands – this can seem insignificant to the clinician but can make a huge difference to patient comfort.11 Simple oral analgesia is part of initial management.
It is very important to provide patient education about the condition, including its natural history and tendency to slowly worsen over time.3 We often explain to patients that the dorsal spur is created over time in response to painful cartilage loss in order to splint and reduce motion in the toe – the body’s coping mechanisms are often amazing. Unfortunately, activities such as hiking, running and gym work often then cause spur impingement pain, and this is the usual time of the initial presentation. To encourage patients to continue an active lifestyle, it can be helpful to tactfully ask if those who run or hike on uneven ground might try nonloading activities such as cycling or water sports or flat ground walking.
Corticosteroid injections to the first MTPJ may provide temporary symptomatic relief, which can delay the need for surgical intervention.12 Currently, there is limited evidence to support platelet-rich plasma or cartilage stimulant injections in the management of hallux rigidus.13,14
If hallux rigidus is refractory to the above measures then surgical management is warranted.3 Cheilectomy or simple removal of the bunion is sometimes indicated, but the patient must be informed that the increased ROM afforded by removal of a spur can lead to increased pain in the intermediate to long term, by reversal of the body’s coping mechanism outlined above. When patients understand why the spur exists this concept can become easy for them to understand. Joint replacement procedures and artificial joint substitutes have less reliable patient satisfaction and outcomes.15
There is sometimes a stigma surrounding arthrodesis of the first MTPJ (great toe fusion), as patients are rightly concerned about the impact this will have on lifestyle and function. However, unlike fusion of other larger joints in the body, a great toe fusion is an excellent procedure that philosophically turns a stiff painful toe into a stiff painless toe. Unless patients perform unusual activities requiring very deep toe flexion, such as ballet or rock climbing, they are usually extremely satisfied with the outcomes of such a procedure.2,3
Conclusion
Hallux rigidus is a very common condition, and its incidence is increasing as the general population becomes more aware of the importance of being fit and active. With correct diagnosis and management, it is very effectively treated with high levels of patient satisfaction. MT