The gut microbiome in health and illness

The gut microbiome plays a vital role in maintaining normal metabolism, nutrition and health, and when perturbed is associated with disease. Evidence suggests that eating a varied diet that includes a diverse intake of plant foods may enhance the gut microbiome. In patients with recurrent Clostridioides difficile infection or ulcerative colitis, faecal microbiota transplant can help re-establish a healthy gut microbiome and induce remission.
- The gut microbiome is the most extensive in the human body and is important for the synthesis, extraction and absorption of numerous metabolites and nutrients.
- The microbiome is influenced by prenatal and environmental factors including maternal prenatal health and postnatal pet exposure, mode of feeding and location of upbringing.
- A diet high and diverse in plant foods may enhance the gut microbiome.
- There is no definitive evidence that fermented foods, such as kimchi, kefir and kombucha, or probiotics are beneficial to gut microbiota.
- Faecal microbiota transplants can help re-establish a healthy gut microbiome and can be used as therapy for Clostridioides difficile infection and ulcerative colitis.
Micro-organisms have lived in symbiosis with humans for millennia and distinct microbiomes are present throughout the body including the skin, genitourinary tract, eyes, lungs and gastrointestinal (GI) tract. The gut microbiome is the most extensive and comprises over 100 trillion microorganisms, mostly bacteria, in addition to viruses, fungi and archaea. These microbes encode more than three million genes, producing thousands of proteins and metabolites, eclipsing the human genome of 20,000 to 25,000 genes.1 The majority reside in the colon, where there is minimal peristalsis and a stable acid-free environment to facilitate colonisation. Although there are close to 1000 bacterial species and over 50 phyla, around 90% of the human microbiome belong to the phyla Bacteroidetes and Firmicutes with other major phyla including Actinobacteria, Proteobacteria, Fusobacteria and Verrucomicrobia.2
Gut microbiota are key regulators of digestion. They aid in the synthesis, extraction and absorption of numerous metabolites and nutrients including all B group vitamins, amino acids, short chain fatty acids (SCFAs, such as butyrate), lipids, bile acids, starches and gums.2 They are also responsible for the production of hormones and neurotransmitters or their precursors such as serotonin, tryptophan, dopamine, noradrenaline, cortisol and glucagon-like peptide-1.3 Gut microbiota also play a crucial role in preventing attack and colonisation from pathogenic bacteria by inhibiting their growth, competing for attachment sites, consuming available nutrients, producing antimicrobial peptides and maintaining intestinal epithelial integrity. The development of the mucosal innate immune system is reliant on exposure to diverse gut microbiota and their products so that appropriate inflammatory responses occur towards pathogens, but not self-antigens that lead to allergy and autoimmune disease.4
There is no such thing as an ideal gut microbiome and each person’s microbiome is unique and changes throughout life. High levels of microbial diversity, richness and resilience are key to a healthy gut microbiome, giving the ability to withstand the threats of disease, stress, poor diet, antibiotics and immunosuppression.2 This article discusses interventions to enhance the gut microbiome through a series of case vignettes, with particular focus on diet and faecal microbiota transplant (FMT).
Development of the microbiome
A 29-year-old woman who is 34 weeks’ pregnant wants to know what factors may influence the development of her baby’s microbiome.
The human gut microbiome is shaped in early infancy and matures in the first few years of life to resemble the more diverse composition of an adult.5 Although the womb was originally thought to be sterile, there is emerging evidence that microbial colonies from the placental and amniotic fluid seed the uterus and the developing fetal microbiome.6,7 Early life events affect the subsequent evolution of the microbiome and its diversity, which in turn may influence the individual’s susceptibility to disease. Environmental factors such as maternal prenatal health, age and antibiotic use, as well as postnatal pet exposure, mode of feeding and location of upbringing may influence an individual’s microbiome.6,8-10
Inoculation with protective vaginal and faecal microbiota occurs during delivery as the fetus traverses the vaginal canal and affects future colonisation in the infant’s gut.11,12 By contrast, infants delivered via caesarean section initially have reduced numbers of Bacteroidetes and a microbiome that is less diverse and healthy, with differences to vaginally-born babies lasting up to 4 years of age.12,13
Early establishment of a healthy microbiome is important as it can affect brain development, stress response, immune programming and metabolic pathways.14 Children born via caesarean section subsequently have a higher risk of obesity, type 1 diabetes, allergies and asthma.11,15 Vaginal seeding, where a caesarean-born baby is swabbed with their mother’s vaginal secretions immediately after birth, has shown promise in partially restoring an infant’s microbiome, but remains controversial, with concerns about safety and efficacy.16 A number of randomised controlled trials (RCTs) are currently underway with both short- and long-term follow up and will guide the utility of this intervention.
Effect of diet on the microbiome
A couple with young children want dietary advice on how to maintain a healthy microbiome for the family without taking any supplements.
Diet, from the moment of birth, plays an integral part in the development and maintenance of the gut microbiome. Breast-fed infants obtain bacteria and prebiotic oligosaccharides from breast milk and surrounding areolar skin and tend to have higher levels of Bifidobacterium and Lactobacillus species, although these differences in microbiota are less prominent with the advent of modern prebiotic-enriched formulae.5,17 As a child transitions to solid food, the composition of their microbiome starts to resemble an adult’s, abundant in bacterial species such as Bacteroides, Roseburia, Clostridium and Anaerostipes species.18
Nondigestible foods that are high in fibre or oligosaccharides such as cereal grains, asparagus, leek, artichoke, legumes, cabbage and kale are important for the maintenance of the microbiome. Often called prebiotics, their selective fermentation in the colon produces SCFAs that provide energy for resident microbes and colonic cells, exert anti-inflammatory effects, maintain gut homeostasis and enhance bacterial diversity.19,20 Overall, plant-based proteins tend to shift the microbiome in beneficial ways with increased production of SCFAs, whereas animal proteins do not.21
Diets that are high in fat, sugar, meat and processed grains, like the Western diet, provide reduced nutrients and substrate to colonic bacteria and are associated with reduced microbiome diversity and increased risk of diseases such as obesity, diabetes and colorectal cancer.22 In contrast, the Mediterranean diet, which is high in fibre, monounsaturated fats, fruits and vegetables, but low in added sugar and red meat, increases microbial diversity, SCFA production and beneficial Bifidobacterium and Lactobacillus species.21 Perhaps the most compelling and simple dietary prescription can be found in results from a massive community-based study of 10,000 individuals, which found that plant diversity strongly correlated to microbiome health and diversity, independent of underlying diet type, with those who consumed over 30 different plants (fruits, vegetables and grains) per week receiving the most benefit (Figure 1).23
{kind=link}
Fermented foods
A patient wants your thoughts on the value of consuming fermented foods to maintain ‘gut health’ as they have recently started drinking their own kombucha and eating sauerkraut each day.
Fermented foods or beverages are produced through controlled microbial growth and enzymatic conversion of food components, a process historically used for food preservation. Common examples include kombucha, sauerkraut, kefir, miso, kimchi and sourdough bread. Recently, fermented food has gained popularity due to proposed health benefits, particularly for the gut microbiome. These potential benefits have primarily been demonstrated in vitro and are mediated by probiotic effects and fermentation-derived bioactive peptides and amines.24
Kefir, a fermented milk drink with a sour taste, is the most studied, with in vitro evidence of antimicrobial properties and in vivo evidence of microbiome enhancement in animals, but not humans. No benefit to functional or inflammatory gastrointestinal disease has been demonstrated.
Kombucha, produced by fermenting black tea with bacteria and yeast, affects oxidative stress and glycaemia in animal studies, but there have been no published studies on gut microbiome or diseases in humans. There have been reports of serious lactic acidosis and hepatotoxicity from kombucha consumption.25
Fermented cabbage (sauerkraut) was shown in one study to reduce symptoms of irritable bowel syndrome (IBS) unrelated to microbiota changes.26 Kimchi (fermented and salted vegetables), miso (fermented soybeans) and sourdough bread may augment a healthy microbiome, but have not been shown to impact health or disease.
Therefore, there is insufficient evidence to recommend any fermented foods be consumed on a regular basis for the purposes of maintaining healthy gut microbiota.
Clostridioides difficile infection
A 45-year-old man with type II diabetes has recurrent episodes of leg cellulitis requiring oral antibiotics. He develops watery diarrhoea, and stool tests are positive for Clostridioides difficile. He is treated with metronidazole 400 mg three times a day for 10 days and his bowels settle.
C lostridioides difficile (formerly known as Clostridium difficile) is a motile, anaerobic, gram-positive rod that is found widely in nature (especially in soil) and forms spores that can survive for months outside the body. C. difficile infection (CDI) is a spectrum ranging from asymptomatic colonisation, to mild diarrhoea, to colitis with severe watery diarrhoea and, finally, pseudomembranous colitis, which carries a risk of bowel perforation and death. Disease is caused by secretion of exotoxins A (TcdA) and B (TcdB), with toxin B having a more prominent role in pathogenesis.27
In healthy individuals, C. difficile rarely causes clinically evident disease because the normal microbiome out-competes C. difficile for nutrients and attachment sites and prevents its spores from germinating. Disruption of the normal microbiome by broad-spectrum antibiotics is the most common risk factor for CDI, and CDI in turn is a common cause of post-antibiotic diarrhoea, accounting for about 10 to 20% of cases. Other important risk factors for CDI are advanced age, diabetes, renal impairment, immunosuppression and use of acid-lowering medications.28 CDI is now the most common nosocomial infection in Australia and the overall burden of disease has been progressively rising over the past 10 years.29
Three weeks later, a repeat stool sample taken from the patient to check for cure is once again positive for C. difficile. The patient has formed stools and is well.
In Australia, the vast majority of stool assays for C. difficile are polymerase chain reaction (PCR) tests looking for C. difficile species expressing the TcdB gene. A positive result simply means a patient is colonised, rather than confirming active disease. Tests of cure should, therefore, not be performed and most laboratories will not process a formed stool. In patients with ongoing diarrhoea, a repeat C. difficile stool test should include an enzyme-linked immunoassay for the toxin as well as the PCR test, to more accurately gauge if the patient has recurrent CDI or simply post-infectious IBS.
Faecal microbiota transplant
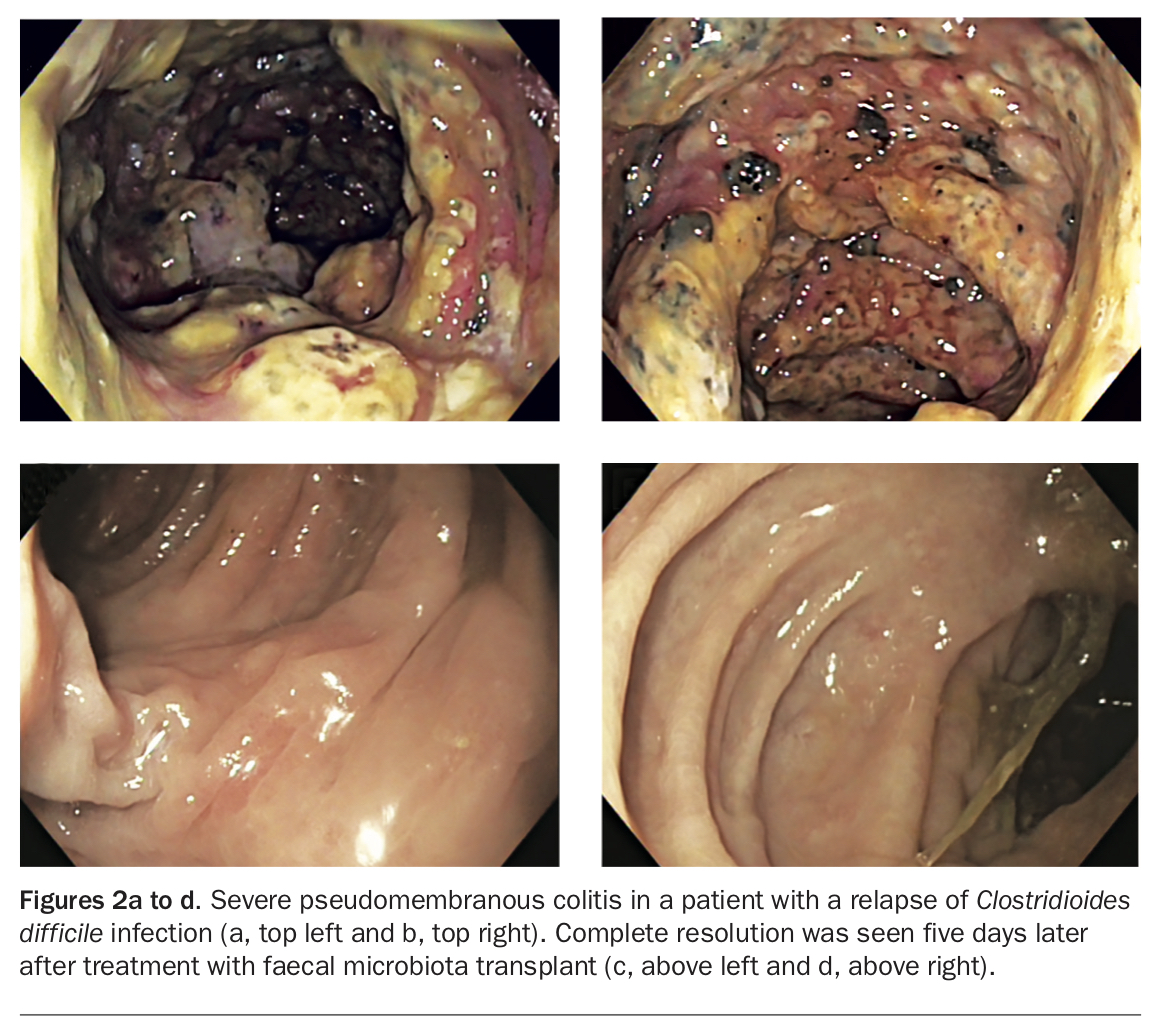
Four months later, the same patient is hospitalised with pneumonia and while on intravenous antibiotics develops watery diarrhoea with a positive test result for C. difficile toxin. He is treated with oral vancomycin 125 mg four times a day for 10 days.
His symptoms settle, but two weeks after he finishes the course of vancomycin, his condition deteriorates, with severe bloody diarrhoea and abdominal pain. Colonoscopy shows pseudomembranes and purulent material coating the entire colon (Figures 2a and b). The patient is treated with faecal microbiota transplant (FMT) via colonoscopy and recovers, with no further diarrhoea, or requirement for antibiotics (Figures 2c and d).
{kind=link}
Up to 30% of patients experience a relapse of CDI after treatment and this increases with every failed therapy. Metronidazole is an appropriate first-line treatment for well outpatients, but those who are hospitalised or have previously failed therapy require oral vancomycin 125 mg four times a day for 10 to 14 days. In patients who experience further relapses or severe disease, FMT is now considered the standard of care, with overall cure rates up to 90% in pooled RCTs.30
FMT as a concept has been around for millennia, with reports of human faecal suspension being used to treat diarrhoea as early as 4th century China in the handbook Zhou Hou Bei Ji Fang (Handy Therapy for Emergencies).31 In 1958, the first Western reports of FMT described faecal enemas for patients with pseudomembranous colitis, but it was not until a Dutch RCT in 2013 that it became more widely accepted and used for recurrent CDI.32,33
The production of FMT as a therapeutic treatment and guidelines for performing FMT have been refined over the past 10 years, with recent Australian-led consensus statements published internationally and regulation in Australia under the Therapeutic Goods Administration (TGA) that commenced in January 2020.30 The TGA regulates FMT as a Class 1 Biological if manufactured and used in the same hospital, or a Class 2 Biological if manufactured elsewhere, with the latter group required to fulfil rigorous good manufacturing practice (GMP) guidelines and be registered in the Australian Register of Therapeutic Goods (ARTG).
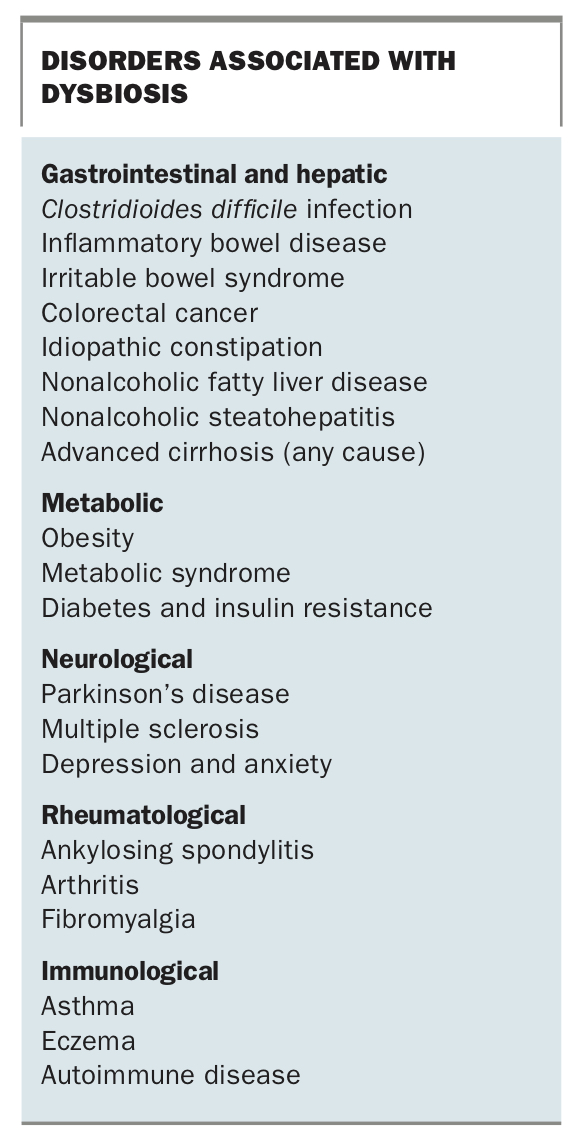
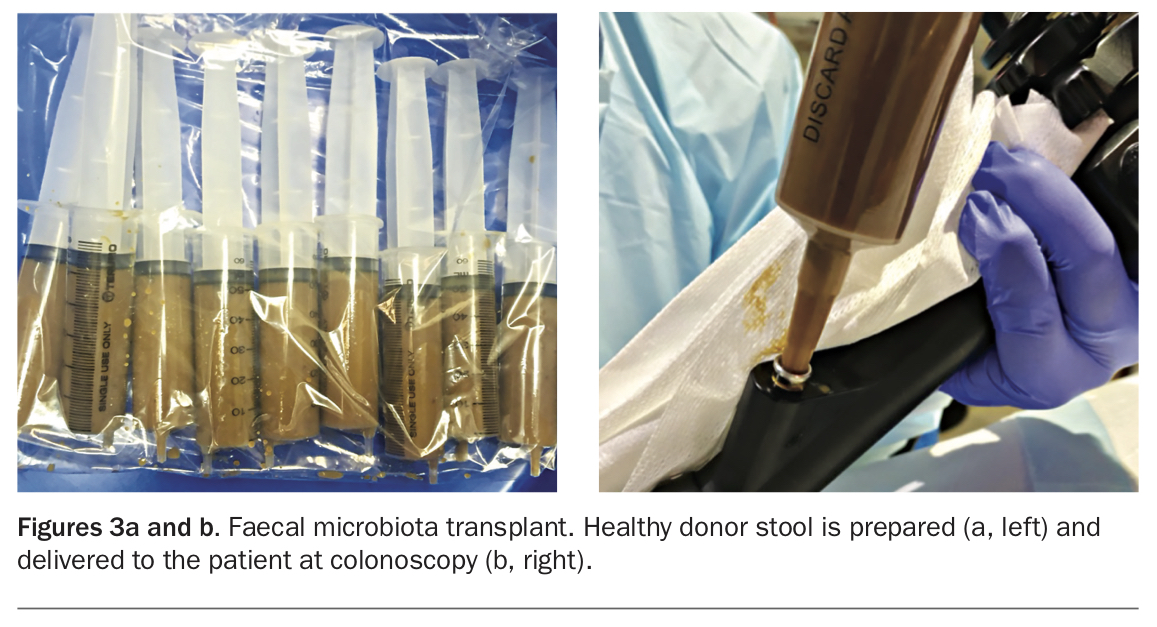
FMT donors must be healthy, lean individuals, aged between 16 and 60 years, free of blood- or stool-borne infections, chronic gastrointestinal disease or any pre-existing conditions associated with dysbiosis, listed in the Box. To prepare an FMT aliquot, donor stool is blended with saline, most commonly in a ratio of 50 g stool to 200 mL saline, with or without 10% glycerol, depending on the need to freeze and store the sample (Figure 3a). Frozen aliquots kept at −80°C remain viable and effective for up to 12 months.34 Stool is then delivered to the colon by instilling it into the caecum at colonoscopy (Figure 3b), via an enema, via a nasojejunal tube or in capsules.
{kind=link}
{kind=link}
FMT is generally safe, with mild bloating, diarrhoea and abdominal discomfort in the first day the most common side effects. More serious adverse events have been reported, however, including infectious, inflammatory or procedure-related events. Transmission of disease susceptibility to autoimmune, metabolic or malignant disease remains a theoretical concern, as does infection with as yet unidentified organisms.30 After two cases of Escherichia coli sepsis, including one death in a patient enrolled in FMT capsule trials, all donor stool is now screened for multiresistant organisms.35
Ulcerative colitis
A 37-year-old woman has a two-year history of left-sided ulcerative colitis that has remained active despite therapy with oral and enema mesalazine and several courses of corticosteroids. She is concerned about taking immunosuppressants or biological drugs and is recruited into a clinical trial of FMT.
Ulcerative colitis (UC) is a chronic relapsing inflammatory disease of unknown aetiology whose pathophysiology is increasingly thought to be linked to alterations in the gut microbiome and gut immune system. Patients with UC have dysbiosis even when in remission, with less microbiome diversity, higher ratios of pathogenic-to-commensal bacteria and areas of bacterial mucosal invasion.36 Specific reductions in Firmicutes genera and some beneficial Clostridium, Akkermansia and Faecalibacterium species are also seen.37 It therefore makes sense that FMT might help induce remission in active UC. Meta-analysis of four placebo-controlled RCTs showed that clinical response and clinical remission to FMT was significantly higher than placebo (49% and 29% vs 28% and 9%, respectively) at an average follow-up of 12 weeks.38 Lower GI delivery of donor stool via colonoscopy or enema appeared more effective in these studies, but further work is needed to determine the optimal route for FMT administration.38 These response rates compare favourably with those of biologicals like infliximab and vedolizumab, leading to a recent consensus group supporting FMT as an efficacious induction therapy for mild to moderate UC, but not for maintenance therapy due to insufficient data.30 Like other therapies, FMT should not be continued when there is a lack of response or disease progression.
Crohn's disease
A 35-year-old man with ileo-colonic Crohn’s disease is keen to have FMT as his sister, who has UC, had a great response to FMT therapy in a recent clinical trial.
Dysbiosis is a hallmark of the Crohn’s microbiome, with reduced diversity and an imbalance between pro-inflammatory and anti-inflammatory bacterial species.39 To date, there has been a paucity of quality data surrounding FMT in Crohn’s disease with only a single pilot RCT that did not meet its primary endpoint or show a statistically significant difference between FMT and placebo.40 The use of FMT for Crohn’s disease therefore cannot currently be recommended outside of a properly conducted RCT.
Irritable bowel syndrome
Evidence that alterations in gut microbiota contribute to the development of IBS is increasing, along with other factors including genetics, dysmotility and altered central nervous system and visceral sensitivity. Patients with IBS have a less diverse microbiome, and specific microbiota profiles have been associated with severity of disease.41 IBS is frequently triggered by prior gut infections, and both probiotics and antibiotics, such as rifaximin, have been shown to ameliorate symptoms of the condition.42 There is mixed evidence for the benefit of FMT in treating IBS, with a meta-analysis of four RCTs showing placebo capsules to be more effective than FMT capsules and only modest benefit for colonoscopy-delivered FMT.41 A more recent meta-analysis of all previously conducted RCTs (seven in total) concluded there was no benefit for FMT in the management of global IBS symptoms.43
Metabolic disease
Obese patients have dysbiosis characterised by reduced richness and diversity that is thought to increase dietary energy harvesting and absorption, which exacerbates weight gain.44 Studies using animal models have shown that the gut microbiome is essential for the development of obesity and the obese phenotype is readily transmissible by FMT in mice. A lean microbial phenotype is also transmissible by FMT and leads to weight loss and normalisation of metabolic parameters in obese mice.28 Two pilot studies in humans have shown an improvement in insulin sensitivity in patients with metabolic syndrome who were given a single FMT from a lean donor.45 However, recently published RCTs in which ‘lean’ FMT capsules were given to obese patients with an average body mass index above 35 have been disappointing.46,47 Despite both studies showing adequate engraftment of the new microbiome, there was no weight loss and no change in insulin sensitivity nor indeed any metabolic parameter at all after 12 weeks. Multiple studies using different FMT preparations or patented microbial mixtures are underway for this indication.
Effect of probiotics on the gut microbiome
A 56-year-old woman is treated with antibiotics for a lower respiratory tract infection and asks whether taking probiotics will help her ‘good bacteria’ get back to normal more quickly. You recommend she maintain a healthy and diverse diet, but not to take probiotics.
Probiotics are live bacteria or yeasts that have the potential to provide a health benefit through enhancement of the intestinal barrier, down-regulation of cytokine production and direct antagonism of gut pathogens.28 Probiotics have been shown to have a modest benefit to symptoms of IBS, and also can assist in the treatment of pouchitis in patients with UC after colectomy.42,48 Meta-analysis of oral probiotics in allergic disease show small improvements in quality of life for patients with allergic rhinitis, but no improvement in overall symptoms and no benefit in the treatment or prevention of eczema.49,50
But can probiotics help the microbiome more rapidly return to baseline after illness or antibiotics? It is well established that antibiotics can cause dysbiosis, at times depleting gut microbiota numbers and diversity by up to 66%.51 Data from a Cochrane review suggest probiotics may reduce the incidence of antibiotic-related diarrhoea in children and positive results were seen in a similar study in adults.52,53 However, probiotics may actively harm microbiome reconstitution after antibiotics. In a recent study, patients given broad-spectrum antibiotics (ciprofloxacin and metronidazole) and supplemented with an 11-strain probiotic mix for four weeks developed a markedly prolonged dysbiosis that lasted for over five months with altered bacterial function, composition and abundance. By contrast, patients who received no therapy after antibiotics developed dysbiosis that slowly but completely resolved over 21 days. Stool samples as late as 180 days after antibiotics had not returned to baseline microbiome configuration in probiotic-treated patients.51
In its latest practice guidelines, the American College of Gastroenterology highlights that probiotics are not recommended for most digestive conditions and found low quality evidence for their use to prevent C. difficile in antibiotic therapy. They specifically advise against using probiotics in children with acute infectious gastroenteritis.54
COVID-19 and the gut microbiome
A 47-year-old develops a high fever, nausea and diarrhoea five days after attending a family wedding where other guests were noticed to be coughing. A nasopharyngeal swab is positive for SARS-CoV-2.
Millions of individuals worldwide have now been diagnosed with SARS-COV-2 infection, the causative virus for COVID-19.55 Although COVID-19 is predominantly a respiratory illness, manifestations and complications involving almost every organ system have been reported. GI symptoms are evident in up to 26% of patients, with the most common being anorexia, nausea/vomiting, diarrhoea and abdominal pain.56 Over 10% of patients in one series presented with GI symptoms and fever only, with no cough or dyspnoea.56 The virus is thought to affect the GI tract by direct tissue injury and entry into enterocytes and endothelial cells via the angiotensin-converting enzyme 2 receptor.57,58 Over 50% of patients with COVID-19 have detectable viral RNA in stool samples, which can persist for many days after respiratory samples become negative and symptoms resolve.57,59,60 This raises the distinct possibility that COVID-19 could be spread by a faecal-oral route.
There is already evidence of a bidirectional ‘crosstalk’ between gut microbiota and the lungs, with bacterial endotoxin and metabolites interacting with the lungs via the bloodstream and lung infections impacting on gut bacteria. It is certainly possible that dysbiosis, which is more common in the elderly and those with metabolic disease, may make those individuals more susceptible to serious outcomes of COVID-19.61 Moreover, animal models suggest that a healthy microbiome reduces enterocyte angiotensin-converting enzyme 2 expression and hence could reduce infectivity.57 To prevent the spread of COVID-19, we are all being urged to use more disinfectants and hand sanitisers, and antimicrobial use has also increased. This will inevitably lead to alterations in gut microbiome and potentially dysbiosis, highlighting the importance of strategies to maintain gut health during this time.
Conclusion
The gut microbiome plays a vital and irreplaceable role in regulating normal health and protection against disease, with high levels of diversity, richness and resilience hallmarks of a healthy microbiome. Sophisticated therapies that alter the microbiome hold great promise for the future, as does the simple act of eating a wide range of fresh fruits, vegetables and grains. MT