Managing mammalian meat allergy and tick anaphylaxis

Tick-induced allergies, including mammalian meat allergy after tick bite and tick anaphylaxis, are increasingly prevalent, particularly on Australia’s eastern seaboard. Tick bite prevention and appropriate management are crucial to both primary and secondary prevention of these allergies. Sensitisation to alpha-gal in mammalian meat can have many consequences, mostly affecting use of certain medical therapies.
Correction
A correction for this article has been published in the April 2021 issue of Medicine Today. The online version and the full text PDF of this article (see link above) have been corrected.
- Tick-induced allergies are emerging worldwide, and tick anaphylaxis has caused fatalities in Australia.
- Mammalian meat allergy after tick bite (MMA) classically presents as severe anaphylaxis that is delayed (typically three to 6 hours after ingesting mammalian meat, i.e. ‘middle of the night’) and evolves rapidly in an individual with a past history of tick bite.
- The MMA spectrum comprises anaphylaxis, other systemic allergic reactions (urticaria and angioedema), gut-predominant symptoms, ‘asymptomatic’ alpha-gal sensitisation and, rarely, food-dependent carbohydrate- induced enterocolitis syndrome.
- Evidence-based tick bite prevention and management strategies are crucial to primary and secondary prevention of MMA and tick anaphylaxis.
- Consequences of developing alpha-gal specific IgE are myriad, affecting the use of medical therapies such as certain vaccines, heparin and cetuximab, and probably increasing atheroma risk.
In Australia, tick-induced allergies are the most common medical conditions caused by tick bites.1 Tick-related allergies are the cause of many presentations to hospital emergency departments (EDs) in tick-hyperendemic regions. For example, a two-year survey of a NSW hospital ED found over 500 presentations of tick bite, 34 of which resulted in anaphylaxis.2
This article describes the spectrum of tick-induced allergies and their presentation, management and prevention.
Spectrum of tick-induced allergies
Tick-induced allergies comprise:
- mammalian meat allergy after tick bites (MMA), caused by allergy to the carbohydrate moiety alpha-gal in mammalian meat3-5
- rarely, probable T cell-mediated food carbohydrate-induced enterocolitis syndrome (FCIES)6
- large local reactions to tick bites and tick anaphylaxis, caused by allergies to tick salivary proteins.1
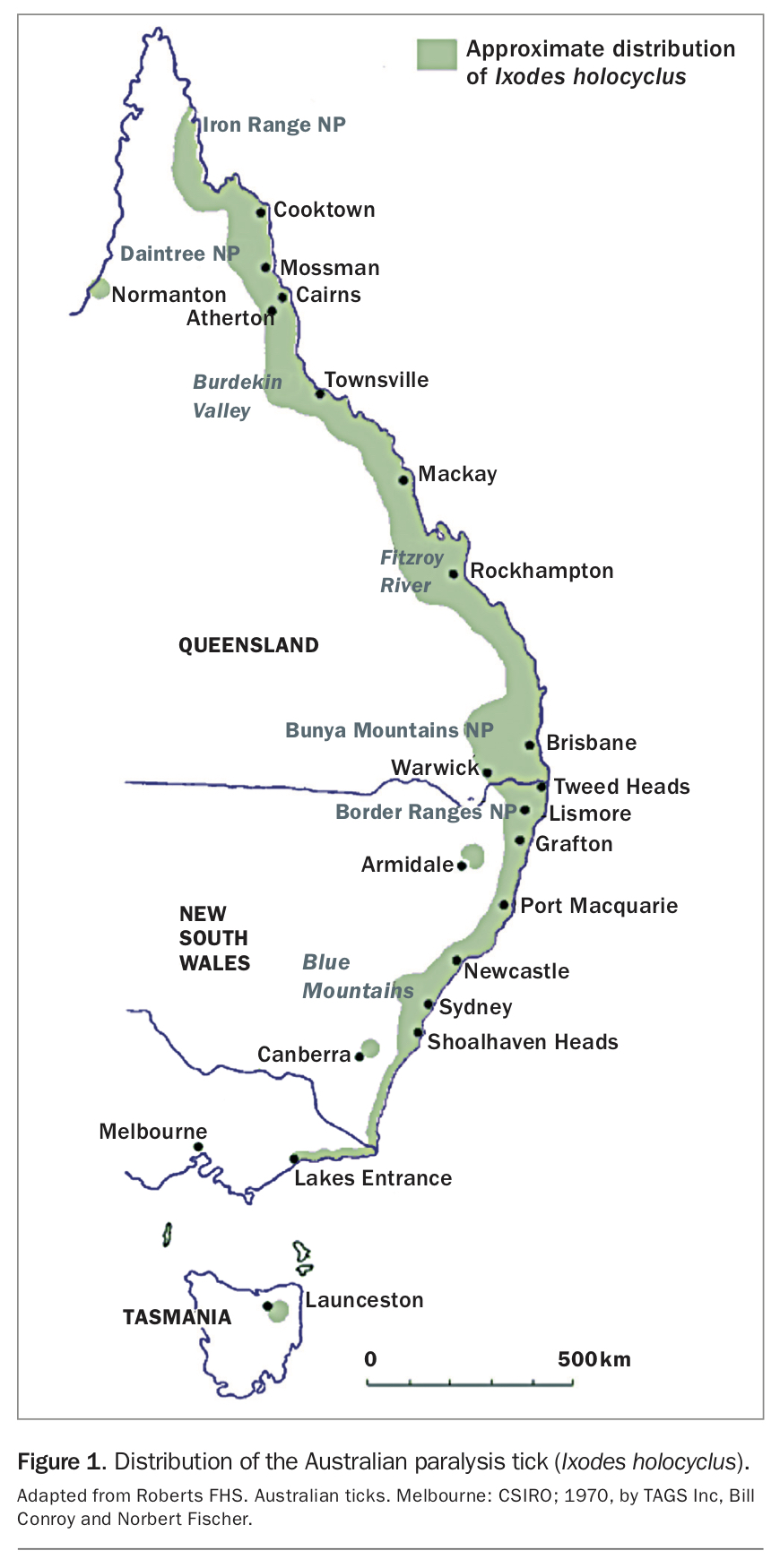
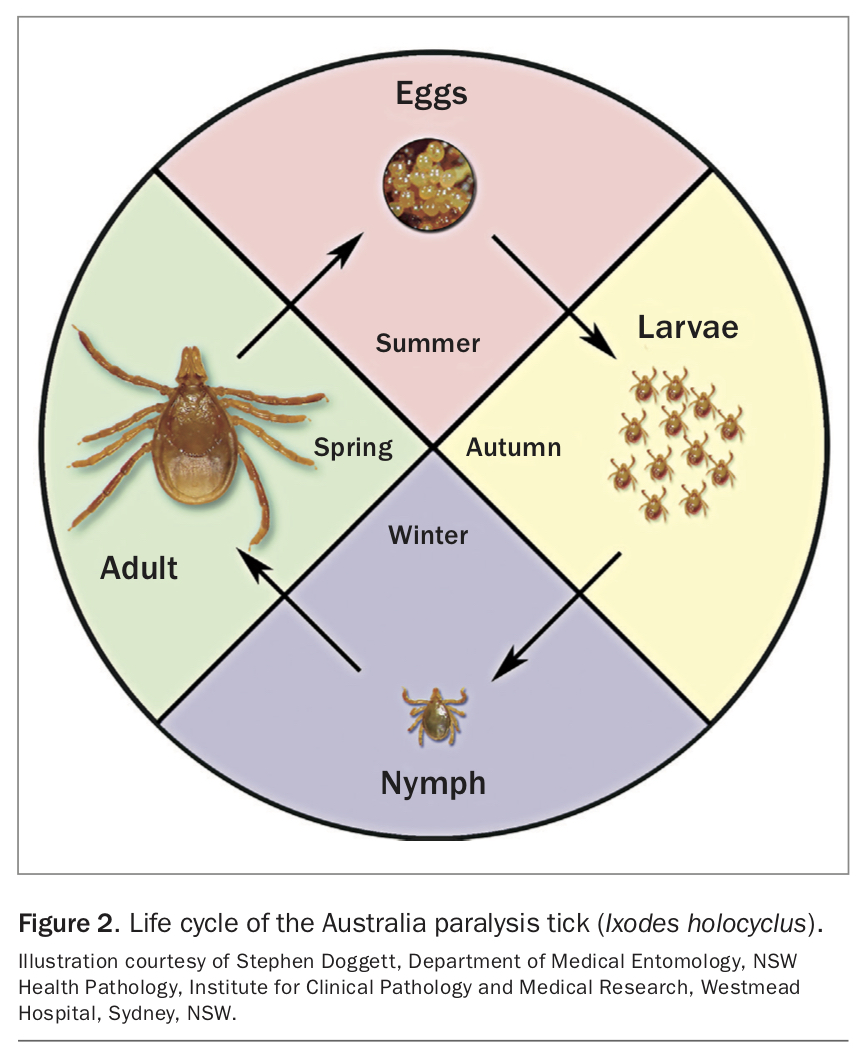
MMA is the most common tick-induced allergy. First described in 2007, MMA has now been reported in 18 countries worldwide, on every continent where humans are bitten by ticks.1,3,4 Depending on the country, different tick species are involved in MMA.1 In Australia, 95% of tick bites are caused by the Australian paralysis tick (Ixodes holocyclus), which is found along most of the eastern seaboard of Australia, from Lakes Entrance in Victoria to Cape York in Queensland (Figure 1).1 A single bite of a nymph stage tick may trigger MMA, as can bites from adult ticks. The life cycle of I. holocyclus is shown in Figure 2. Because individuals who have been bitten only by larval ticks are rare, it is unclear whether larval tick bites alone can trigger the development of MMA.
{kind=link}
{kind=link}
Australia has the highest prevalence of MMA (113 per 100,000 population).7 More than half of all Australians live in regions where I. holocyclus is endemic. The recent description in Western Australia of a second tick species able to cause MMA, Ixodes (Endopalpiger) australiensis, increases the number of people exposed in Australia to around 60%.8
In tick-endemic regions of Germany and the USA, sensitisation rates to alpha-gal allergen have been estimated to be as high as 35%, with MMA symptoms occurring in 8 to 9% of the population.7 Most people with tick anaphylaxis also have specific IgE (sIgE) against alpha-gal but often have no clinical sensitivity to mammalian meat at the time of the tick anaphylaxis.9
Preventing tick-bite allergies
Evidence-based strategies for tick bite prevention and management have been developed with the aim of preventing tick-induced allergies. Research published in 2019 has verified the advice given since 2013 by the Australasian Society of Clinical Immunology and Allergy (ASCIA), Tick-induced Allergies Research and Awareness (TiARA) and the Emergency Care Institute New South Wales.10
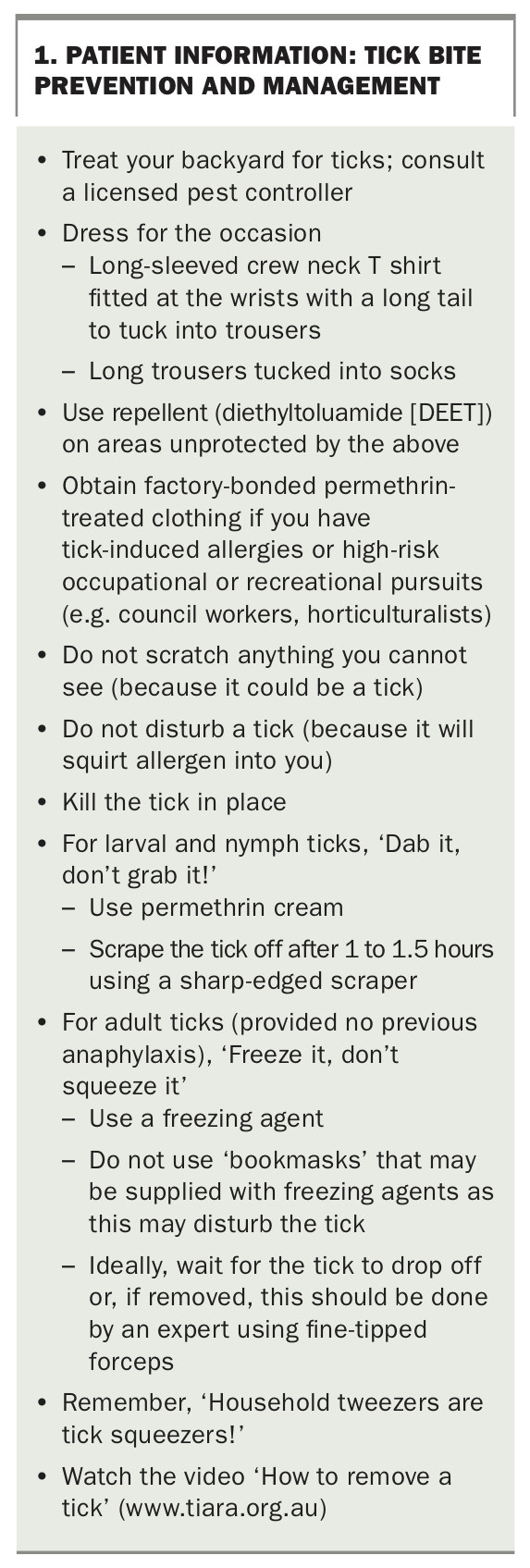
The essential elements of recommended management of tick bites are:10
- Kill the tick in situ by freezing
- After the tick is killed, allow it to drop off or, if removal is undertaken, this should be done by an expert using fine-tipped forceps
- Avoid any compression of the tick, which will likely transmit tick saliva containing multiple salivary protein allergens as well as alpha-gal
- Use tick repellent to help prevent tick bites; diethyltoluamide (DEET) is established as the most practical and effective tick repellent.11
Patient information on tick bite prevention and management is summarised in Box 1.
{kind=link}
Allergies to tick salivary proteins
Large local reactions to tick bites
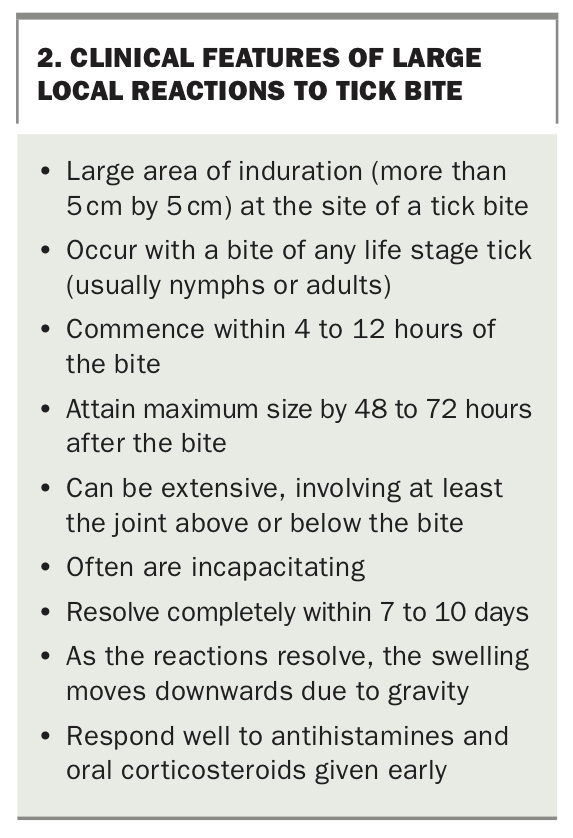
Large local reactions to tick bites are the least severe form of tick-induced allergy. The clinical features of large local reactions are summarised in Box 2.
{kind=link}
Recommended management of a large local reaction to a tick bite comprises:
- elevation of the bite area above the level of the heart
- application of ice
- early use of oral antihistamines (which should be continued for seven to 10 days depending on duration of pruritus), and
- early use of a short course of moderate-dose corticosteroids (e.g. 50 mg for an adult daily for three days) or a single dose of dexamethasone 4 mg.
Often, large local reactions to tick bite are indistinguishable from cellulitis, and patients may be treated with antibiotics, sometimes parenterally, especially when the reaction affects the periorbital area. Patients who have experienced a large local reaction should keep antihistamine and oral corticosteroid to hand, as early use after a subsequent tick bite may limit a subsequent reaction and reduce the possibility of requiring antibiotics.
Tick anaphylaxis
Tick anaphylaxis is the most severe form of tick-induced allergy and was responsible for four deaths in Australia between 1997 and 2013.12,13 Tick anaphylaxis, like MMA, is increasing in prevalence on the eastern seaboard of Australia. However, unlike MMA, tick anaphylaxis has rarely been recorded overseas, although reports of tick anaphylaxis are increasing from Spain and Japan.14-17
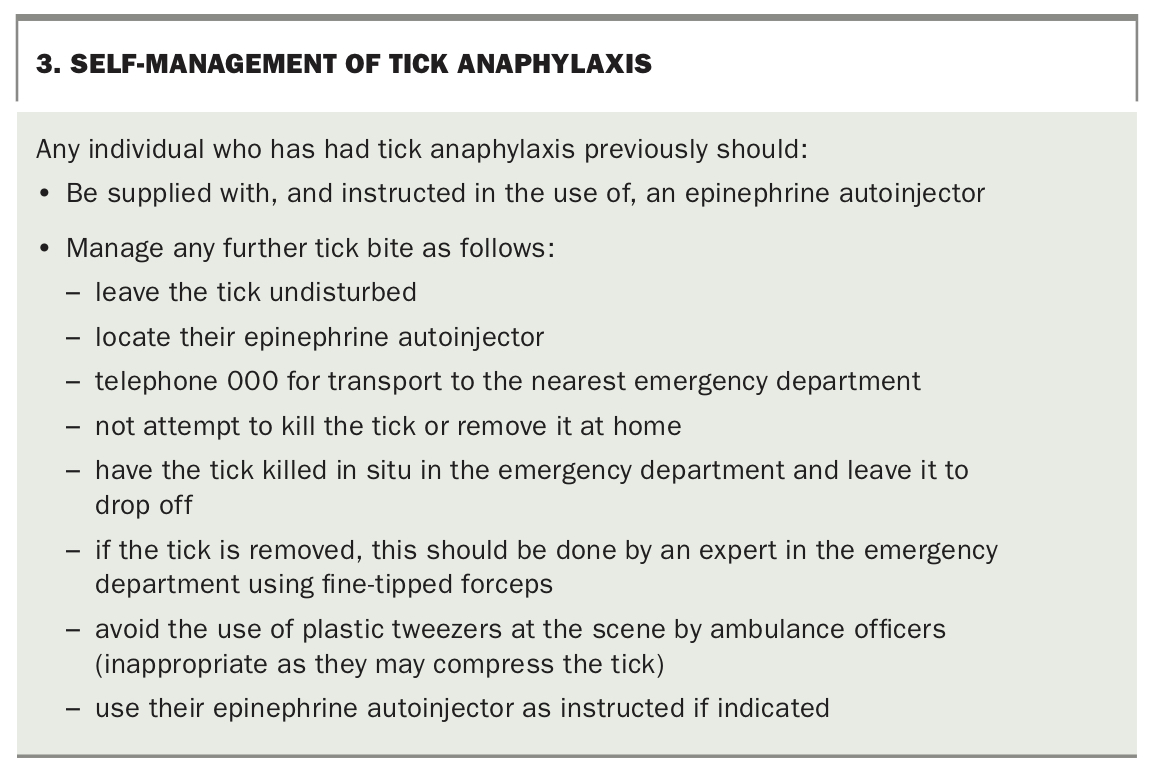
Tick anaphylaxis is due to an IgE-mediated allergic reaction to one of five tick salivary proteins injected into the host by the tick when feeding.18-22 Bites from nymph and larval ticks may prime the production of sIgE to tick salivary proteins; however, only the bite from an adult tick can trigger an episode of anaphylaxis, which occurs when the tick is disturbed by inappropriate handling.23 Prevention of tick anaphylaxis involves preventing tick bites and managing any tick bite with evidence-based techniques (Box 3).
{kind=link}
Mammalian meat allergy after tick bite
Alpha-gal is a carbohydrate formed from the combination of two galactose molecules by the enzyme alpha-galactosyltransferase. Alpha-gal is a constituent of the connective tissue of many mammals, but is not found in the tissues of humans, great apes or Old World monkeys. It is known to be present in tick saliva.24 As alpha-gal is foreign to the human immune system, it stimulates the formation of IgG antibodies. Alpha-gal is also manufactured by the mucosal biome and coats the proteins of infectious agents on mucosal surfaces. This enhances the immune system’s ability to recognise the pathogen and to mount an efficient IgG-based immune response.25
Although the immune response to alpha-gal is usually an IgG response, some predisposed individuals also elaborate IgE directed against alpha-gal.20 When humans with sIgE against alpha-gal later ingest alpha-gal in mammalian meat or other products, they may develop an allergic reaction.
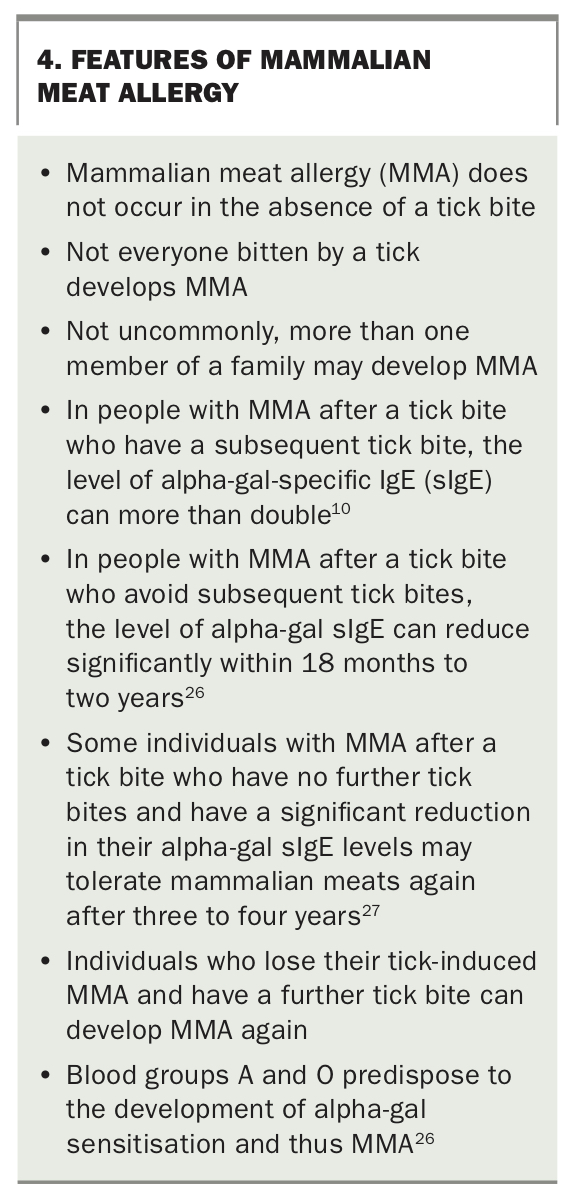
Features of MMA are shown in Box 4.10,26,27 MMA does not occur in the absence of a tick bite, but some individuals may be unaware of having been bitten by a tick.28 This may happen if they are visitors rather than residents in tick-hyperendemic area (e.g. the Northern Beaches area of Sydney, Maleny in Queensland, Denmark in Western Australia and Lakes Entrance, Victoria), especially if it is a nymph stage tick (2 mm long, resembling a black splinter) or is removed without being visualised (e.g. scratched from the scalp).
{kind=link}
The MMA spectrum comprises:
- the classic presentation of mammalian meat anaphylaxis
- other systemic reactions (urticaria and angioedema)
- gut-predominant symptoms
- ‘asymptomatic’ alpha-gal sensitisation
- FCIES (uncommon).
An algorithm for the diagnosis and management of MMA is shown in the Flowchart.
Mammalian meat anaphylaxis
Presentation
The classic presentation of MMA is delayed anaphylaxis after a mammalian meat meal in an individual with a past history of tick bite. The reaction typically occurs three to six hours after ingesting mammalian meat (i.e. ‘middle of the night’). The anaphylaxis evolves rapidly, is often severe and is due to intravascular basophil activation.29 It occurs in people with a past history of tick bite, but as mentioned above this history may be difficult to elicit.28
Symptoms of mammalian meat anaphylaxis are those of anaphylaxis in general, except for the delay in onset. This delay is due to the time taken for the glycolipid allergen to be absorbed from the gut into intestinal lymphatics and thence the inferior vena cava, and to activate basophils in the circulation, thus triggering anaphylaxis.
Mammalian meat anaphylaxis may also present as anaphylaxis to gelatine. This is more likely after parenteral administration, for example in a vaccine such as Zostavax.
Diagnosis and management
Treatment of mammalian meat anaphylaxis is nonspecific and the same as for any patient with anaphylaxis. Provision of an epinephrine autoinjector, instruction in its use and an anaphylaxis action plan are essential.
Diagnosis of mammalian meat anaphylaxis depends on the clinical features. Radioallergosorbent (RAST) measurement of allergen-specific IgE levels against alpha-gal, beef, lamb, pork and bovine gelatine is recommended at diagnosis as a baseline to facilitate future advice. Measurement of the convalescent tryptase level is prudent to exclude coincident mastocytosis.
Patients diagnosed with MMA require dietary advice from an accredited practising dietitian, with supplementary information available from TiARA (www.tiara.org.au). For patients who have had mammalian meat anaphylaxis, initial strict avoidance of mammalian meats is recommended. Some people with mammalian meat anaphylaxis also react to mammalian meat vapours (e.g. barbecue meat fumes).30
A minority of individuals who have experienced mammalian meat anaphylaxis will also react to mammalian milk and milk products. Typically, they react to soft cheeses and cheeses containing animal rennet (in some imported cheeses) but tolerate hard cheeses. Mammalian milks and their products should be excluded only if they cause symptoms at any stage.
Patients who are negative for sIgE to bovine gelatine usually tolerate oral gelatine, but parenteral gelatine (e.g. in certain vaccines) should usually be avoided.31
Patient education is essential for people with MMA about:
- prevention and management of further tick bites (Box 1)
- the risks of alpha-gal sensitisation (see below).
Provided the patient has no further tick bites, they may be able to reintroduce mammalian meat after several years. Reintroduction should be guided by a reduction in alpha-gal sIgE levels.32
Other systemic reactions (urticaria and angioedema)
MMA can also manifest as typical urticaria and angioedema appearing three to six hours after mammalian meat ingestion. Lesions may occur at the site of a previous tick bite.
Treatment is as for urticaria and angioedema in general. Further management includes dietary advice and education about tick bite prevention and management and the risks of alpha-gal sensitisation, as for patients with mammalian meat anaphylaxis. However, for people with urticaria and angioedema, further symptoms can usually be prevented by:
- avoiding amplifying factors with mammalian meat ingestion (see below)
- eating small portions of mammalian meats
- avoiding products with higher concentrations of alpha-gal such as offal.
Cured meats (e.g. bacon, ham and prosciutto) are often tolerated in small amounts. As with mammalian meat anaphylaxis, mammalian milks and their products should be excluded only if they cause symptoms. Oral gelatine is usually tolerated by those who are negative for sIgE to bovine gelatine, but parenteral gelatine should usually be avoided, even in this group. Reintroduction of mammalian meats should again be guided by a reduction in alpha-gal sIgE levels.
Gut-predominant symptoms
Some people experience gut-predominant symptoms after mammalian meat ingestion. Colicky abdominal pain is a feature. Nausea may precede the pain, and diarrhoea is common. Urticarial lesions and patchy erythema may be present.
Antihistamines and corticosteroids are usually not helpful for gut-predominant symptoms. Epinephrine is not indicated and does not improve gut symptoms if used. The recommended dietary and other advice is similar to that for people with MMA manifesting as urticaria and angioedema.
Food-dependent carbohydrate-induced enterocolitis syndrome
FCIES affects 1% of people who react to mammalian meat.6 Symptoms are the same as those of food-dependent protein-induced enterocolitis syndrome (FPIES), as follows.
- Protracted severe vomiting and diarrhoea are features
- Hypotension often occurs (due to a fluid phase shift to the gut)
- Pallor and lethargy are typical (in contrast to IgE-mediated reactions where erythema is usual).
Patients with FCIES are convincingly negative for alpha-gal sIgE (as in FPIES). FCIES is thus not considered an IgE-mediated condition but is attributed to T cell-mediation.
Dietary advice for people who have experienced FCIES is similar to that for people with mammalian meat anaphylaxis. Reintroduction of mammalian meat may be possible in future years, provided there is no subsequent bite from a tick at any life stage. However, there is no in vitro test to guide mammalian meat reintroduction in people with FCIES and no current evidence specifically regarding the likely success and timing of this reintroduction.
Role of amplifying factors in MMA
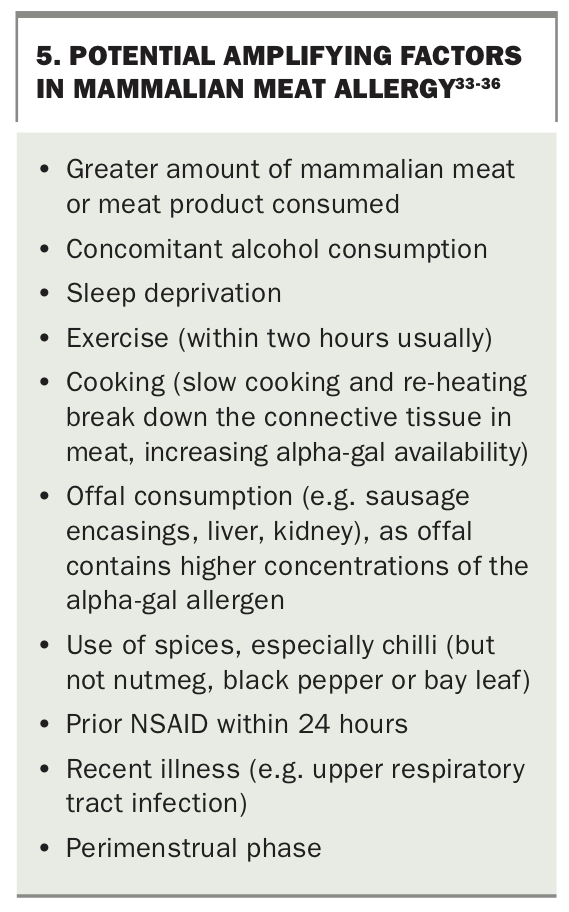
Certain factors (cofactors) around the time of food ingestion can amplify reactions to food allergens in general and in MMA (Box 5).33-36 For example, in people with peanut allergy, the dose of peanut required to elicit an allergic reaction is reduced by 45 to 61% when they have exercised within two hours of eating and by 45% when they are sleep deprived.36 More than one amplifying factor may operate in a single episode of allergic reaction.
{kind=link}
Consequences of alpha-gal sensitisation
‘Asymptomatic’ individuals with alpha-gal sensitisation (i.e. they have developed sIgE to alpha-gal but are not clinically reactive to mammalian meats) may constitute up to 25% of the population in tick-hyperendemic regions.7 After two tick bites, up to 50% of individuals may be sensitised to alpha-gal.17
Almost all individuals with alpha-gal sIgE levels greater than 5.5 kU/L have symptomatic MMA after mammalian meat ingestion (more than 95% probability).32 Among individuals with lower levels of alpha-gal sIgE (less than 5.5 kU/L), about two-thirds will have symptoms when they ingest mammalian meats or products in the presence of an amplifying factor.
Other potential consequences of developing alpha-gal sIgE are myriad, mostly affecting the use of medical therapies.
Therapeutic implications
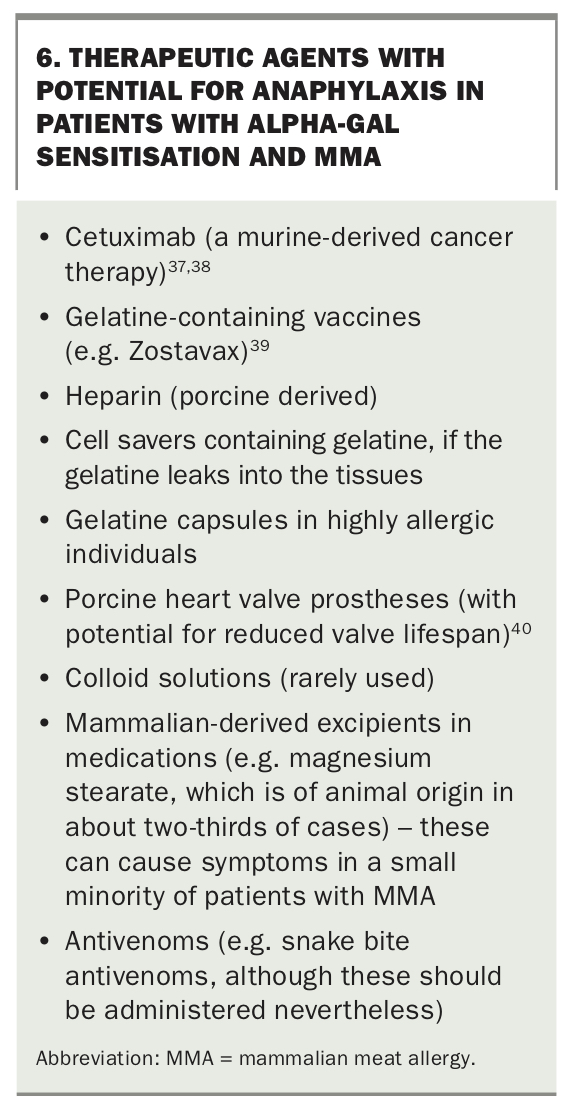
Therapeutic agents with potential for causing anaphylaxis in people with alpha-gal sensitisation and MMA are listed in Box 6.37-40 These include the murine- derived monoclonal antibody cetuximab, used to treat colon and head and neck cancers. There is a 6.9% risk of anaphylaxis with cetuximab use in Northern Sydney, with 59 cases, including two fatalities, reported to the TGA Database of Adverse Event Notifications up to July 2020 (www.tga.gov.au/database-adverse-event-notifications-daen).37,38 Current best practice is to check for alpha-gal sIgE before use of cetuximab. Low levels of alpha-gal sIgE may be associated with life-threatening anaphylaxis, even where mammalian meats are tolerated, typically with the first cetuximab dose.37,38
{kind=link}
Gelatine-containing vaccines such as Zostavax can cause anaphylaxis, with one formal and several anecdotal reports.39 Mammalian-derived excipients in medications can cause symptoms in a small minority of patients with MMA. For example, magnesium stearate in medications is of animal origin in about two-thirds of cases. This is often undeclared, and patients need to check with the pharmaceutical company supplying the drug in Australia.
Alpha-gal sensitisation and atherosclerosis
In people younger than 65 years, alpha-gal sensitisation has been associated with more extensive coronary artery atherosclerotic plaque and more unstable atherosclerotic plaque.41 Preliminary findings of a study in a large Australian cohort support this risk.42 Tick bites constitute a major public health problem on this basis alone.
Reintroduction of mammalian meats
Almost invariably, levels of alpha-gal sIgE in people with MMA are higher against bovine thyroglobulin alpha-gal than against beef, followed by pork, and lowest against lamb and mutton. However, reintroduction of mammalian meat usually begins with cured pork products such as bacon and prosciutto and then ham (providing these foods are allowed in the patient’s usual diet) as these are the mammalian meats most likely to be tolerated.
The patient should begin with a piece of meat the size of a grain of rice, eaten early in the day to avoid the three to six hour delay obscuring milder symptoms during sleep. If this is tolerated, they can progressively double the amount of meat consumed on any day it is convenient until a portion size is reached. If cured pork meats are tolerated then lamb (e.g. lamb cutlet) can be introduced in the same manner, followed by fresh pork and thereafter fresh beef.
Spices and chilli should be avoided, as should raw, reheated or slow-cooked meat, at least until tolerance for the particular mammalian meat is confirmed. The patient should be advised to avoid amplifying factors initially on the days meat is being eaten.
Conclusion
Tick-induced allergies (MMA and tick anaphylaxis) are increasing in prevalence, particularly on Australia’s eastern seaboard. Resources on tick allergies for patients and medical practitioners are listed in Box 7. Tick bite prevention and management are crucial to both primary and secondary prevention of tick-induced allergy. Sensitisation to the allergen alpha-gal in mammalian meat has myriad potential consequences, mostly affecting use of particular therapies. Confirmation of the association between alpha-gal sIgE and atherosclerosis severity, however, means that tick bite prevention and management campaigns will be even more important in keeping Australians safe from the sequelae of tick bites. MT
{kind=link}