Adrenaline injectors – update on prescribing

Anaphylaxis
Allergy
Adrenaline (epinephrine) is the first-line treatment for anaphylaxis, and two types of adrenaline injector are available for use in Australia. Prescribers need to be aware of the different instructions for their use and recent changes to adrenaline dose recommendations.
Anaphylaxis is a severe, potentially life-threatening allergic reaction, and intramuscular (IM) adrenaline (epinephrine) is the treatment of choice.1-4 Adrenaline injectors (AI) have been available for more than 40 years and allow rapid administration of IM adrenaline by the patient or a lay person.5-7 In Australia, the EpiPen AI has been available on the PBS since 2003. From 2021, a second type of AI device that can deliver a higher dose is also available on the PBS, Anapen. Here, we discuss the role of AIs in treating anaphylaxis, how to prescribe them, including dose and patient education, and compare EpiPen and Anapen.
What are adrenaline injector devices?
AIs are single-use devices that deliver a set dose of adrenaline, designed for use by people without medical training to treat anaphylaxis. Adrenaline is the only first-line drug to treat anaphylaxis and should be administered promptly by IM injection into the outer mid-thigh.1-3 IM administration has been the route of choice for optimal delivery of adrenaline in treating anaphylaxis for over 20 years.1,3,4,8 There are no contraindications to the use of IM adrenaline to treat anaphylaxis.2,4
Adrenaline is a nonselective adrenergic agonist with a rapid onset of action. Adrenaline acts to reduce airway mucosal oedema, induce bronchodilation, induce vasoconstriction and increase cardiac contraction strength.1,4 Two AI devices are TGA approved and available in Australia, with both listed on the PBS: Anapen (containing 150, 300 or 500 mcg doses) and EpiPen (containing 150 or 300 mcg doses). A generic AI similar to EpiPen is also PBS listed. AIs are designed to keep adrenaline stable and have an expiry date in excess of one year after manufacture.
When to use an AI device
AIs are used for the first-line treatment of anaphylaxis. Anaphylaxis is a severe allergic reaction that is often under-recognised and undertreated.1,3,9 Definitions vary worldwide, but the Australasian Society of Clinical Immunology and Allergy (ASCIA) defines anaphylaxis as:2
- any acute onset illness with typical skin features (urticarial rash or erythema/flushing, and/or angioedema), plus involvement of respiratory and/or cardiovascular and/or persistent severe gastrointestinal symptoms (gastrointestinal symptoms of any severity are a symptom of anaphylaxis to insect stings or injected drugs); or
- any acute onset of hypotension or bronchospasm or upper airway obstruction where anaphylaxis is considered possible, even if typical skin features are not present.
The ASCIA definition is consistent with the criteria published in the World Allergy Organization (WAO) Anaphylaxis Guidance 2020.3
AIs may be self-administered or given by people without medical training. AIs are also sometimes used to treat anaphylaxis in medical facilities as they contain a fixed dose of adrenaline, which may reduce the risk of overdose and delays in administration.
Although most anaphylactic reactions are not fatal, reactions are unpredictable.10,11 Factors that may affect the severity of reactions include dose of the allergen, route of exposure, presence of asthma, other drug use (alcohol, beta blockers, ACE inhibitors) and exercise, but importantly, there are no reliable clinical predicators of a severe reaction.3,4,10 Although patients who have previously had anaphylaxis would be considered at risk of subsequent severe reactions, a history of previously mild reactions is not a good predictor of subsequent reaction severity.10,12 Early use of IM adrenaline can treat the symptoms of anaphylaxis and reduce the risk of fatal reactions, although these sometimes still occur.1,3,4,12,13
Antihistamines and corticosteroids do not treat or prevent anaphylaxis and should not be used in the first-line treatment of anaphylaxis.1,10 Patients may fear adrenaline or feel reassured that past reactions with respiratory or cardiovascular symptoms have resolved either without treatment or with the use of antihistamines or corticosteroids. However, any apparent benefit is not due to the action of either medication, whose onset and mechanisms of action will not reverse symptoms of anaphylaxis, but due to endogenous responses, which may vary with each reaction.1,4,10 Although antihistamines are listed on the ASCIA action plans to treat mild to moderate symptoms of allergic reactions such as hives, progression to respiratory or cardiovascular symptoms should be treated with an AI without delay.
How to give AI devices
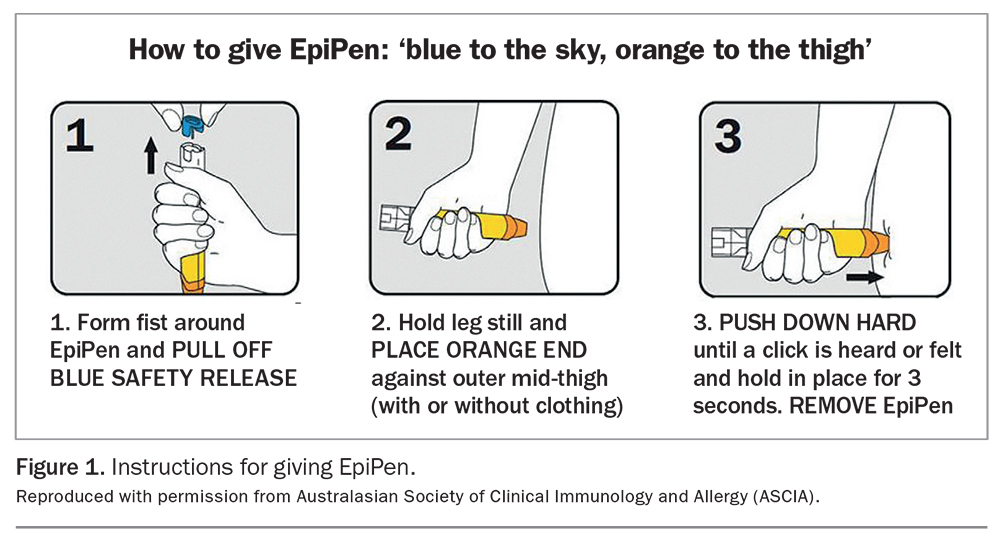
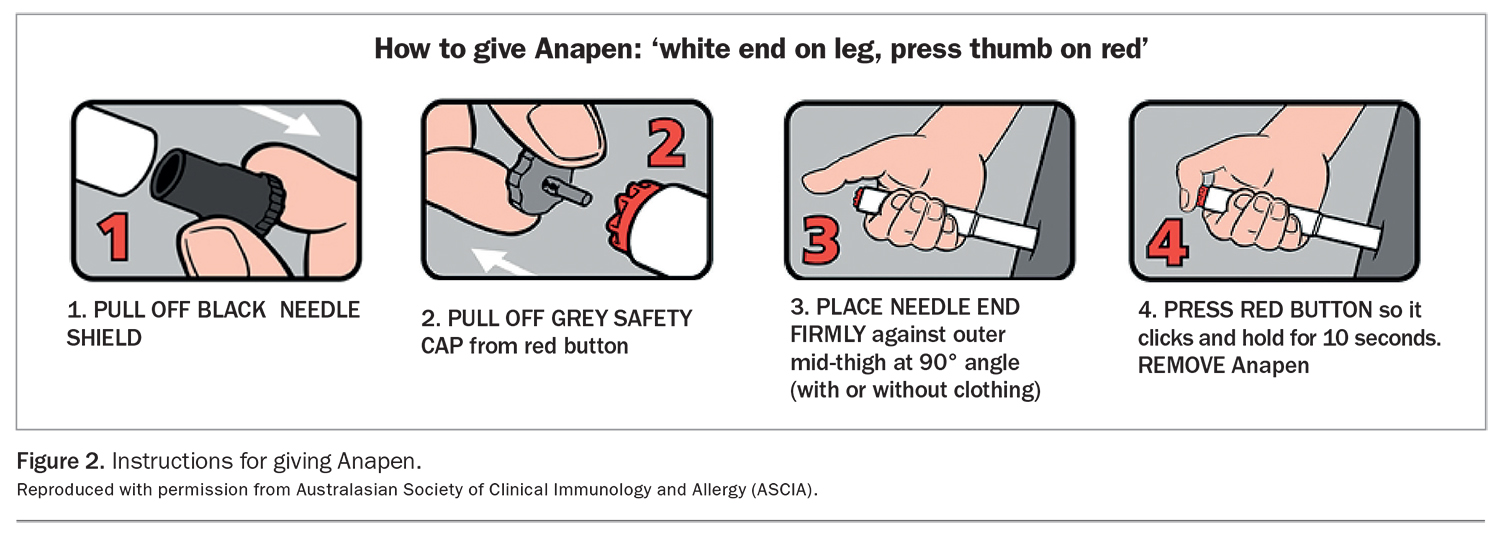
Instructions on how to administer adrenaline with EpiPen and Anapen are shown in Figure 1 and Figure 2, respectively. Instructions and videos are also available on the websites of ASCIA (https://allergy.org.au/) and the patient support organisation Allergy and Anaphylaxis Australia (https://allergyfacts.org.au).
{kind=link}
{kind=link}
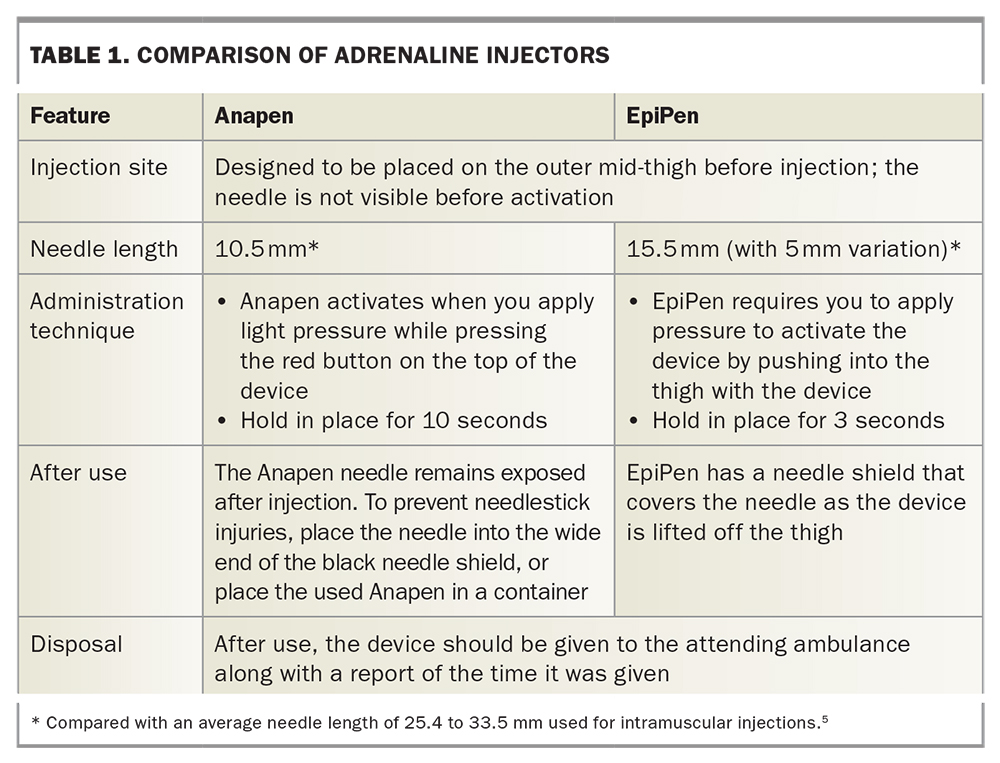
Features of Anapen and EpiPen are compared in Table 1. Patient cost is the same as both are subsidised by the PBS and they have similar over-the-counter prices.
{kind=link}
Prescribing AI devices
AI devices are available in Australia on PBS authority prescription, and an initial prescription is indicated for the anticipated treatment of anaphylaxis. This can be prescribed by a clinical immunologist or allergy specialist, paediatrician or respiratory physician, or by a doctor or nurse practitioner if the patient has been discharged from hospital or an emergency department after treatment with adrenaline for anaphylaxis. Because of different legislation, emergency physicians in NSW are unable to prescribe AI on authority prescription, but it is recommended that the patient is provided with at least one AI by the hospital pharmacy on discharge.
Sometimes, patients who have had a clear episode of anaphylaxis do not receive adrenaline in the emergency department for a range of reasons, including failure to present, symptom improvement by the time they arrive in the emergency department, or failure of treating staff to recognise anaphylaxis. In these cases, GPs (and emergency department medical officers) have the option to contact an on-call hospital immunologist to discuss authorisation for an initial AI prescription, given the PBS criteria state that the patient ‘must have been assessed to be at significant risk of anaphylaxis by, or in consultation with, a clinical immunologist’. This can prevent a possible excessive delay for AI prescription, given the potentially long wait time to see an immunologist or other specialist.
Patients are eligible for up to two devices per prescription with no repeats. Continuing PBS supply for anticipated treatment of anaphylaxis can be prescribed by a doctor or nurse practitioner if the patient has previously been issued with an authority prescription and their devices have been used or expired. It is important to specify the brand and tick the ‘no substitution’ box on a PBS prescription to ensure the brand is not substituted. AIs are also available without prescription at a nonsubsidised cost.
Prescribing an AI alone is not enough to manage patients at risk of anaphylaxis. It is important also to provide education on allergen avoidance, recognition of anaphylaxis and AI use, and to encourage patients and families to practise regularly with a training device. Training devices can be reused and are available from Allergy and Anaphylaxis Australia. An ASCIA action plan for anaphylaxis should always be provided with an AI. Anapen- and EpiPen-specific versions are available (https://www.allergy.org.au/hp/anaphylaxis/ascia-action-plan-for-anaphylaxis).
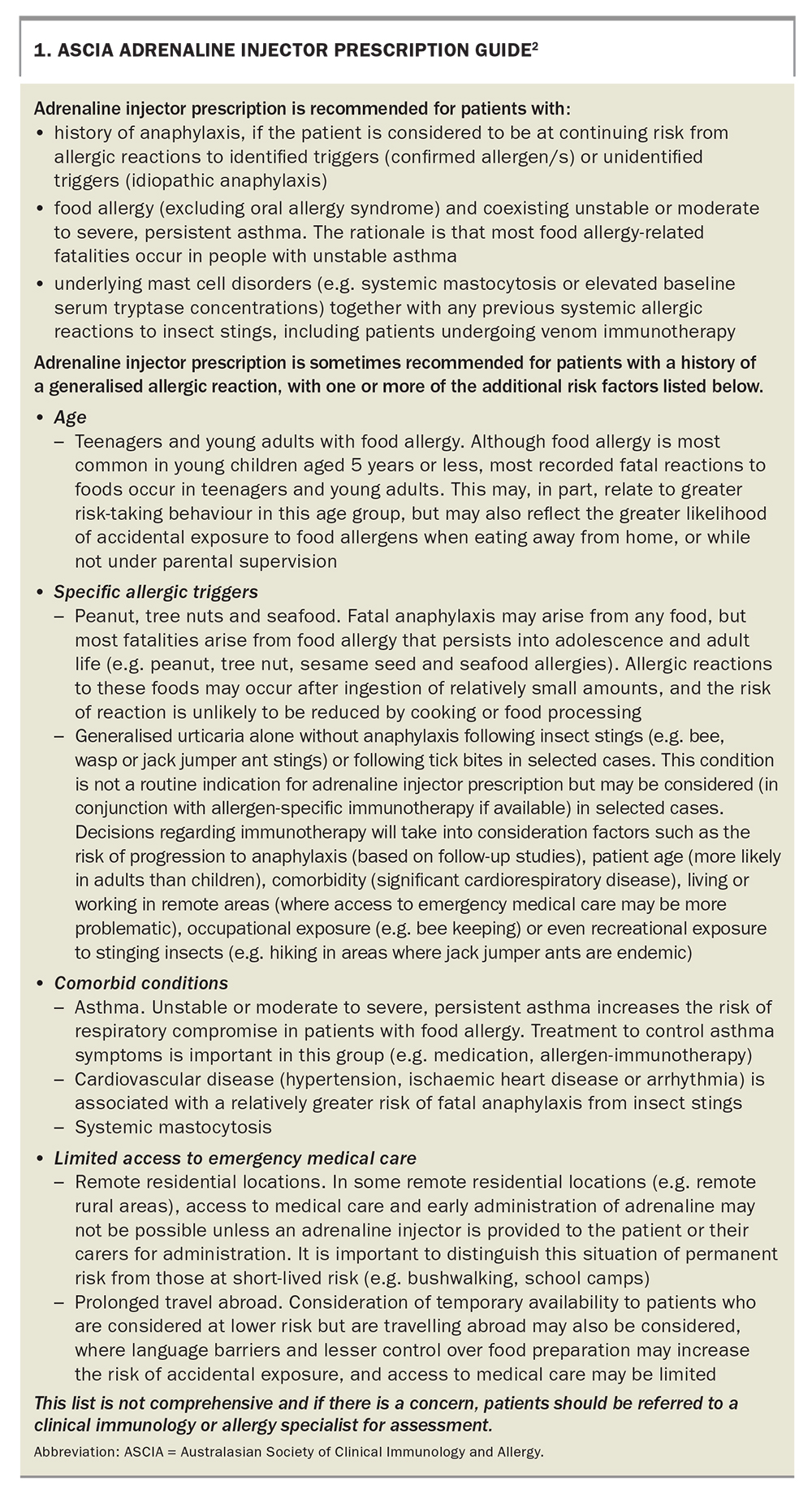
The ASCIA adrenaline injector prescription guide is shown in Box 1.
{kind=link}
Adrenaline dose
The optimal dose of adrenaline to treat anaphylaxis is not known.5-7 Current recommendations are based on limited pharmacokinetic studies in healthy people but are supported by decades of clinical practice.1,3-7
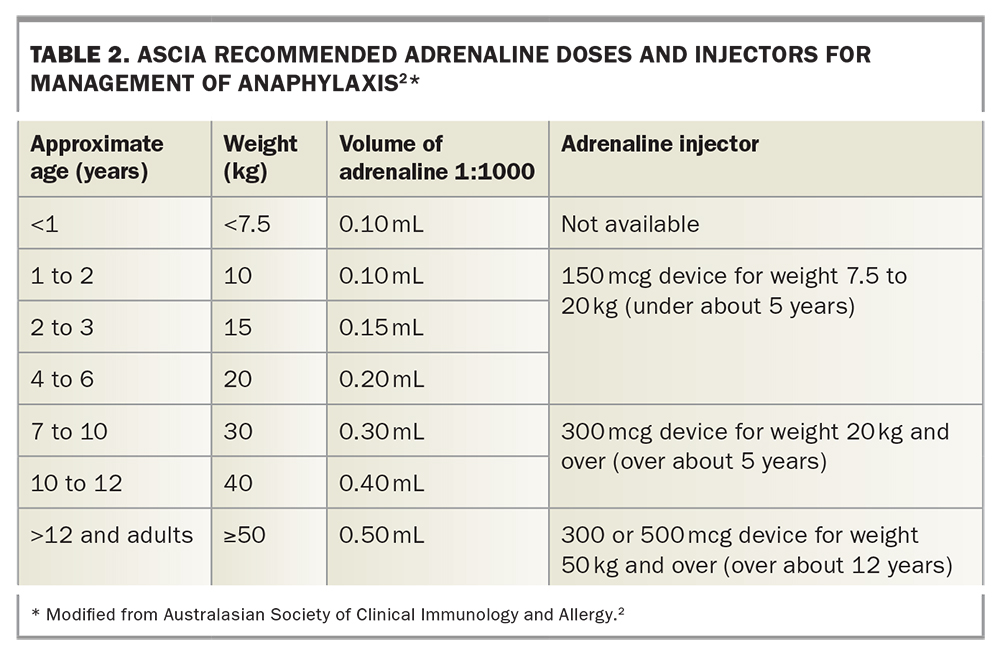
In line with international guidelines, ASCIA recommends an adrenaline dose of 0.01 mg/kg (maximum 0.5 mg) to treat anaphylaxis (Table 2).1,3,4 IM adrenaline should be given at a dose of 0.01 mL/kg of a 1:1000 (1 mg/mL) solution, as this gives acceptable volumes for IM injection.
{kind=link}
For adrenaline IM autoinjection, ASCIA recommends a 150 mcg AI device for patients weighing between 7.5 and 20 kg, a 300 mcg device for patients weighing between 20 kg and 50 kg, and a 300 mcg or 500 mcg device for patients weighing 50 kg or more.
ASCIA’s weight recommendations differ from those in the product information for both the Anapen and EpiPen AIs. In 2021, ASCIA revised the lower limit of its weight recommendation for the 150 mcg AI device from 10 kg to 7.5 kg, based on the following rationale.
- The change aimed to reduce potential underdosing and provide AI options for infants weighing less than 10 kg. Food allergy is prevalent in this age group, and prescribing adrenaline to those at risk of anaphylaxis is challenging.7,10 Currently, a 100 mcg AI is not available in Australia. The options are either to provide an ampoule of adrenaline with a sterile syringe or a prefilled syringe or to prescribe a 150 mcg AI.
- Although the use of a 150 mcg AI delivers double the recommended 0.01mg/kg dose in a 7.5 kg infant, IM adrenaline has a good safety profile and is generally well tolerated.7,12,14
- Providing a syringe and ampoule of adrenaline to parents is strongly discouraged as it increases the risk of significant dosing errors (as a high as 40-fold in one study) and leads to delays in administration.15
- Providing a pre-filled syringe of adrenaline also has disadvantages as a method to prevent the plunger being depressed is not easy to achieve, and the syringe needs to be refilled regularly as adrenaline is stable in a syringe for only up to three months.7
The recommended dose of adrenaline for adults weighing 50 kg or over is 0.5 mg.1-4 Although either a 300 mcg or 500 mcg AI can be used in teenagers and adults, a 500 mcg device gives a higher maximum concentration of adrenaline. A person weighing 50 kg would receive almost 50% less than the recommended dose with a 300 mcg device.6,7 Adrenaline generally reaches its peak concentration five to 10 minutes after injection by AI, so if anaphylaxis symptoms persist at five minutes then a second dose is recommended.2,3,5,6
Concerns have also been raised about the potential for subcutaneous injection with AIs in people with a greater skin-to-muscle distance. Although larger head-to-head studies of AIs are needed, a recent systematic review concluded that device-dependent injection force and speed may be more important than needle length in determining adrenaline pharmacokinetics, and that the time to peak adrenaline concentration was generally longer in people with a greater skin-to-muscle distance, although overall bioavailability was similar.6,16
Why are there two AI devices available in Australia?
Since 1 September 2021, two AI devices have been available in Australia on the PBS. Most countries have multiple brands of adrenaline injector devices available, and both EpiPen and Anapen devices are widely used in other countries. Having both EpiPen and Anapen available is important:
- to ensure continued supply of life saving adrenaline, particularly if one brand has stock shortages
- to provide doctors with a choice of dose as
– they may prefer to prescribe a higher dose (500 mcg device) for people who weigh over 50 kg
– a 500 mcg dose may potentially prevent the need for further doses of adrenaline (which is important due to increasing ambulance delays and many people carrying only one device) - to encourage suppliers to provide devices with longer shelf life
- to provide choice for consumers to access devices with points of difference to best suit their needs.
AI complications
AIs are generally safe. Potential injuries related to AI use include injection into a digit, lacerations, embedded needles and bone injury.7,17 Training can reduce the risk of AI complications, and redesign of AIs over the years has aimed to reduce the risk of injury. Lacerations requiring sutures have been reported in children after AI use.17 The risk of laceration can be reduced by holding the device in place on the thigh before activating it, and securely holding the child to immobilise the leg and reduce movement.7,17 Although bone injury is a theoretical risk, particularly in infants and children with shorter skin-to-bone distance, no confirmed bone injuries caused by AIs have been reported.7,17,18 Bunching the skin before injection may help reduce the risk of bone injury.7
How to store an AI
AIs should be stored in a readily available location, in a cool dark place at room temperature (15 to 25°C). AIs should not be kept in a locked cupboard or refrigerated, as temperatures below 15°C may damage the injector mechanism. People at risk of anaphylaxis should have their adrenaline injector with them at all times. An insulated wallet is recommended if a person carrying a device is outside for an extended time, as studies have shown that after even 12 hours in a car on a warm day the concentration of adrenaline in an AI can reduce by up to 14%.19
Conclusion
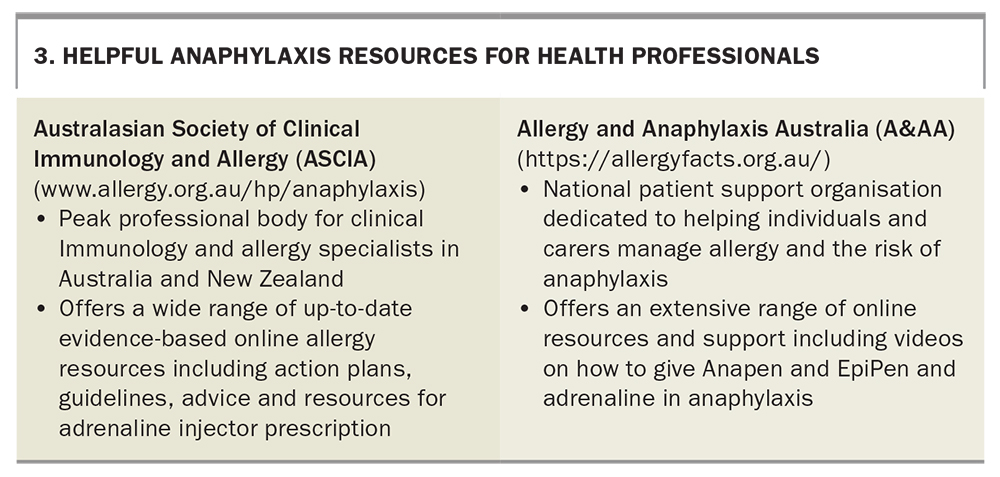
Prescribing an AI is an essential part of the management of people with anaphylaxis. The availability of a second type of AI device adds to the treatment options and can provide a higher adrenaline dose (500 mcg) for people who weigh 50 kg or over. Practice points on AIs are summarised in Box 2 and helpful online resources on anaphylaxis for health professionals are listed in Box 3.
{kind=link}
{kind=link}
COMPETING INTERESTS: Dr Frith has received payment for an educational video on anaphylaxis from Arterial Education. Ms Smith reports that ASCIA receives unrestricted educational grants from sponsors which help ASCIA develop and update online resources; content is not influenced by sponsors. Professor Katelaris: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.