Vaccination for adolescents

Immunisation
Adolescent health
GPs are often unaware of their important role in supporting adolescent vaccination, which primarily occurs through the school-based vaccination program. Ensuring vaccinations are up to date and missed doses are completed should be considered a standard preventive health activity for the adolescent patient in general practice.
Correction
A correction for this article is published in the June 2021 issue of Medicine Today. The online version and the full text PDF of this article (see link above) have been corrected.
Note
An updated version of this article is available in the March 2022 issue of Medicine Today.
Australia has achieved high rates of childhood vaccination, with substantial increases over the past 20 years.1,2 Much of this success can be attributed to the commitment of general practitioners and the effective strategies they have implemented. Vaccination of adolescents has become increasingly important, especially since the introduction of the national human papillomavirus (HPV) vaccination program, which has had a substantial impact on HPV-related disease, and other vaccines relevant to this age group. These have included the pertussis booster (diphtheria-tetanus-acellular pertussis [dTpa] vaccine), meningococcal ACWY and B vaccines and influenza vaccine for vulnerable groups (Table 1).3 Equally high rates of vaccination need to be achieved in adolescents as in young children.
{kind=link}
As vaccination of adolescents primarily occurs through the school-based vaccination program, GPs may not see themselves as playing an important role. However, working alongside the school program, GPs are crucial in achieving the same high coverage that is seen in early childhood vaccination programs. GPs can ensure all adolescent patients in their practice are up to date with their vaccinations and provide any that have been missed in the school program. Disruption to student attendance at school from closures or restrictions during the COVID-19 pandemic may have interrupted vaccination initiation or completion, especially when more than one vaccine dose is required.4 Although GPs have always had a vital role in providing vaccinations to adolescents with anxiety or special needs, as well as those who are Aboriginal or Torres Strait Islander, culturally and linguistically diverse, homeless or do not regularly attend school, reviewing all adolescents’ vaccination status in general practice has never been more timely.
School-based vaccination and vaccination coverage
The Australian National Immunisation Program (NIP) funds vaccination across the lifespan, with vaccines listed in the schedule provided free for target groups. Unlike other populations, adolescents are primarily vaccinated en masse at school after parental consent is obtained.5 School-based vaccination has proven to be an effective and cost-efficient means to promote relatively high vaccination coverage for adolescents.6-9 In 2017, when the Australian quadrivalent HPV vaccine schedule required three doses, 80.2% of girls aged 15 years and 75.9% of boys aged 15 years received a full course of the vaccine.2 Of Aboriginal and Torres Strait Islander girls and boys aged 15 years who received the first dose, 79% and 77%, respectively, completed the three doses, compared with 91% and 90% of non-Indigenous girls and boys, respectively.2 Data are not yet available on coverage of the two-dose nonavalent HPV vaccine (implemented from 2018 for adolescents aged 14 years or younger at the first dose) or dTpa and meningococcal ACWY vaccines.
It is important to provide catch-up vaccinations to low-coverage groups, particularly Aboriginal and Torres Strait Islander adolescents, given their lower vaccination completion rates and longer time to completion.2,10 As Aboriginal and Torres Strait Islander women have twice the incidence and four times the mortality rate of cervical cancer as other Australian women, recommending HPV vaccination to Aboriginal and Torres Strait Islander adolescents represents an opportunity to reduce this health disparity.2,11,12
Although school programs aimed at adolescents generally result in relatively high vaccination uptake, coverage for adolescent vaccinations remains more than 10 percentage points lower than that achieved for childhood vaccinations.1 Ideally, vaccination coverage rates in adolescence should be higher; for example, the WHO has called for coverage of 90% to achieve elimination of cervical cancer.13 GPs are an important part of the solution for achieving this goal (Box).
{kind=link}
Role of GPs in adolescent vaccination
Addressing missed opportunities for vaccination in general practice
Missed vaccination opportunities during consultations in healthcare settings are a major concern during both childhood and adolescence. Adolescents who have missed vaccinations offered in the school program because of school absence or other reasons are usually provided with a letter and recommendation to visit a GP or council clinic to catch up on the vaccine doses missed. Given the decline in frequency of visits to GPs in adolescence compared with childhood, this often does not eventuate.14 Young people aged 15 to 25 years have the lowest proportion of face-to-face time spent with GPs in Australia.15
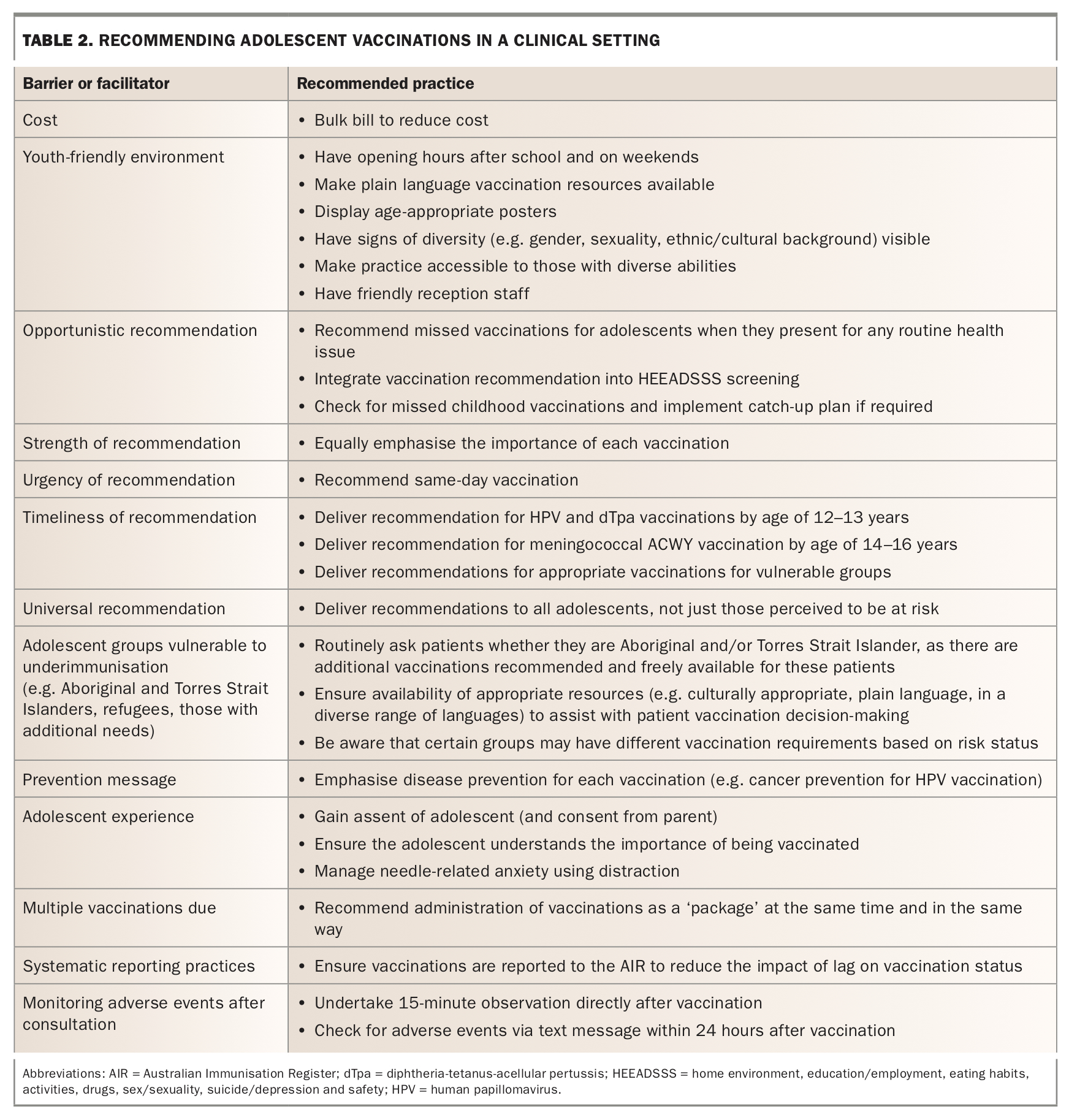
Unlike in some countries, such as the United States, where reimbursements are provided for preventive primary care visits in adolescence, during which HEEADSSS (home environment, education/employment, eating habits, activities, drugs, sex/sexuality, suicide/depression and safety) screening and vaccinations routinely take place, there is no Medicare rebate for GP preventive health care visits for adolescents and young adults in Australia.16,17 This means that GPs need to actively consider assessing immunisation status of adolescents attending their practice for other reasons and opportunistically vaccinate them when it is clear they have missed a vaccine dose in the school program (Table 2). Adolescence is also an opportune time to ensure catch-up of missed doses of childhood vaccines.3,18
{kind=link}
Providing a strong recommendation
GPs also play a key role in facilitating adolescent vaccination through the school program, with multiple studies showing that a recommendation from a healthcare provider is the most important driver to increase vaccination uptake.19,20 Parental vaccination decision-making on behalf of adolescents is influenced by physician recommendation, government recommendation, perceived benefits of the vaccine and concerns about side effects and vaccine safety.19,21-23 Social determinants of health, including socioeconomic status and ethnicity, and factors relating to patient engagement have also been found to influence vaccination uptake, although to a lesser extent in school-based programs.24,25 Parental barriers to adolescent vaccination include not receiving a provider’s recommendation, lack of information about vaccination, concerns about timing of vaccination (e.g. adolescent’s age for HPV vaccination) and misconceptions about efficacy and safety.
Offering vaccines as a package
It is important to present adolescent vaccinations that may have been missed as a ‘package’.26 If more than one vaccination has been missed, more than one should be offered at the same time. If an appointment is made to complete the course on another day, there is increased risk of noncompletion. For example, emphasising cancer prevention benefits and discussing HPV vaccination at the same time as recommending dTpa vaccination is more likely to result in higher uptake of both vaccinations.
Promoting vaccine health literacy among adolescents and their parents
GPs have a unique opportunity to overcome health and vaccine literacy deficits among adolescents and parents. Parents’ health literacy is positively correlated with adolescent health literacy and health.27 Providing recommendations and education to parents and adolescents about vaccination as a prevention strategy to reduce disease burden and promote health and wellbeing is crucial. Challenges may include different cultural and religious beliefs, low literacy generally, misinformation and inequities, such as reduced access to health services and diminished ability to seek help with the vaccine decision-making process.24 These factors should be considered when dealing with parent and adolescent queries and concerns about vaccines; well-designed resources, such as the Sharing Knowledge About Immunisation ‘Is the HPV vaccine really safe?’ factsheet, can be used to support conversations.28
Research has identified several challenges that providers face in discussing vaccination with adolescents and their parents: discomfort with talking about sexual behaviour (e.g. with HPV vaccination), lack of time or incentive for patient education, and lack of a system that issues reminders about vaccine status and whether multiple doses are required.29,30 Overcoming these barriers, such as by using automated systems for reminders, can directly affect adolescent vaccination uptake.
Overcoming incomplete vaccination of adolescents
Assessing vaccination history of all adolescents in the practice
Young people aged 10 to 19 years require an assessment of their immunisation history to ascertain any missing childhood or adolescent vaccinations and to develop a catch-up schedule. The vaccination records of all adolescent patients in the practice can be reviewed by checking their records in the Australian Immunisation Register (AIR), including checking that any previous vaccines were administered in the recommended dosing intervals and at the correct age.18 Appointments should be scheduled to complete vaccinations for patients who are clearly behind on the schedule.
Assessing vaccination history of adolescents presenting to the practice as new patients
An adolescent presenting to the practice as a new patient for any reason should be asked about vaccination, ideally when undertaking a HEEADSSS assessment, but any time is appropriate. As parents and adolescents may not have accurate records or knowledge of vaccination status, GPs can identify whether vaccinations are up to date using Health Professional Online Services (www.servicesaustralia.gov.au/
organisations/health-professionals/services/medicare/hpos) or by calling the AIR enquiries line (1800 653 809).3
If a vaccination may have been administered but is not recorded on the AIR, the relevant immunisation provider for that vaccine should be contacted.3 If doses cannot be confirmed because of incomplete documentation, it should be assumed that those doses have not been administered. Serological testing is not routinely recommended.18 There are no risks associated with additional doses of vaccines when they have already been received, apart from a possible increase in local adverse events with frequent doses of dTpa-containing vaccines.18 All vaccine doses administered should be reported to the AIR, and data will need to be entered directly if the general practice software does not automatically report vaccinations.
Missing out or being late for vaccinations listed in the NIP may have financial ramifications for families who will be unable to receive their appropriate childcare and Family Tax Benefit payments on time.
Communicating with adolescents and parents about vaccination
Trust can be built with adolescents and parents through open and respectful communication, underpinned by evidence-based information on vaccination risks and benefits. At the same time, it is important that clear recommendations to vaccinate are provided and that opportunities to vaccinate are not missed. Regardless of the reason for a consultation, when there are vaccinations outstanding, using language such as ‘I recommend you receive these vaccinations today’, rather than ‘What would you like to do about these vaccinations?’, can influence parent and adolescent decision-making.26
Given that policies in the education environment mean that parents usually provide consent for vaccination of adolescents under 18 years of age in the school vaccination program, there are ethical considerations in balancing emerging adolescent autonomy and their desire to also be involved in vaccine decision-making.31 All states and territories have medical consent policies that recognise the competency of mature minors. This means that adolescents under the age of 18 years are able to provide their own consent to vaccination if they are assessed as Gillick competent by the practitioner. Generally, healthy adolescents aged at least 14 years have capacity to consent to a low-risk intervention, such as vaccination.32
Adolescents do not always make connections between their behaviour (e.g. sexual activity or smoking) and their current or future health outcomes, and they can experience difficulty assessing the quality of health information, which they most frequently access online. Nuanced messaging targeted at specific age groups may be required, recognising that different barriers may exist to receiving HPV vaccination for a younger adolescent compared with barriers to receiving meningococcal ACWY vaccination for an older adolescent.
Younger adolescents are less able to moderate their needle-related fear and anxiety because of incomplete cognitive maturation. Vasovagal syncope is the most common severe adverse event experienced with vaccination in adolescence.33 Needle-related anxiety can affect an adolescent’s choice of whether to have a vaccine, despite parental consent. Using youth-friendly language and resources to explain vaccination benefits and side effects can promote adolescent vaccination literacy and facilitate discussion with parents and involvement in vaccination decision-making, as well as helping to mitigate needle-related anxiety. The WHO has produced an excellent resource to assist vaccination providers in managing this anxiety.34 Explanations of exactly what will happen and what the needle will feel like, along with appropriate distraction methods, can also assist younger adolescents to cope with needle-related anxiety.35 Communicating successes achieved through vaccination programs can assist in counteracting concerns about vaccine efficacy and safety and mitigate vaccine hesitancy.
Conclusion
GPs are key players in parents’ and adolescents’ decisions to have vaccinations. They can opportunistically prioritise vaccination during routine consultations and ensure the adolescent is up to date with the vaccination schedule recommended in the NIP. The partnership between GPs and the school-based vaccination program is important for achieving high vaccination uptake in adolescence. We need to eliminate the long-standing health inequity experienced by adolescents due to lower vaccination coverage compared with that in early childhood. GPs are also key to improving uptake in marginalised adolescent populations with persisting low vaccination coverage. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.