Perimenopausal hormone therapy – assessment and prescribing

Perimenopause is characterised by menstrual cycle and hormonal changes leading to the final menstrual period. Women benefit from a comprehensive assessment including screening, health promotion and, if symptomatic, a discussion about treatment options.
The perimenopause is the beginning of the hormonal fluctuations that lead to the final menstrual period and is characterised by menstrual cycle irregularity and symptoms related to hormonal fluctuations. All patients at perimenopause benefit from the opportunity for a full assessment, including health screening and preventative activities, along with a personalised discussion of treatment options if they have symptoms. This includes a discussion about the risks and benefits of menopausal hormone therapy (MHT) or other treatments for symptoms. MHT is the most effective treatment for menopausal symptoms and can be offered to most patients with symptoms.1 Some gender diverse patients can experience perimenopause and menopause, and may benefit from special services. For the purpose of this discussion, we refer to cis women (hereafter referred to as women).
What is perimenopause?
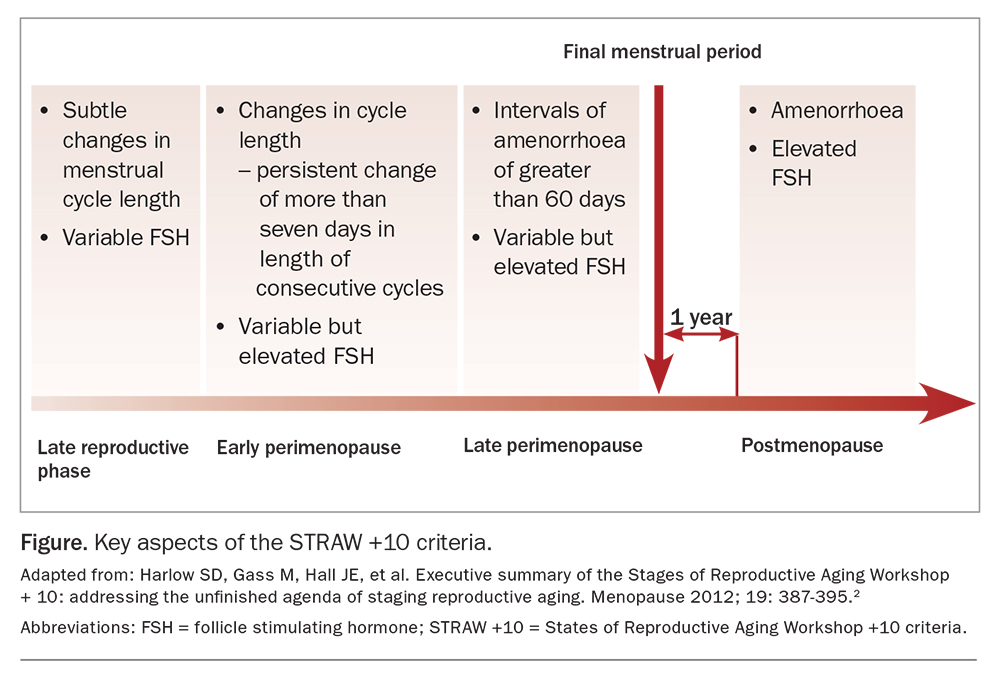
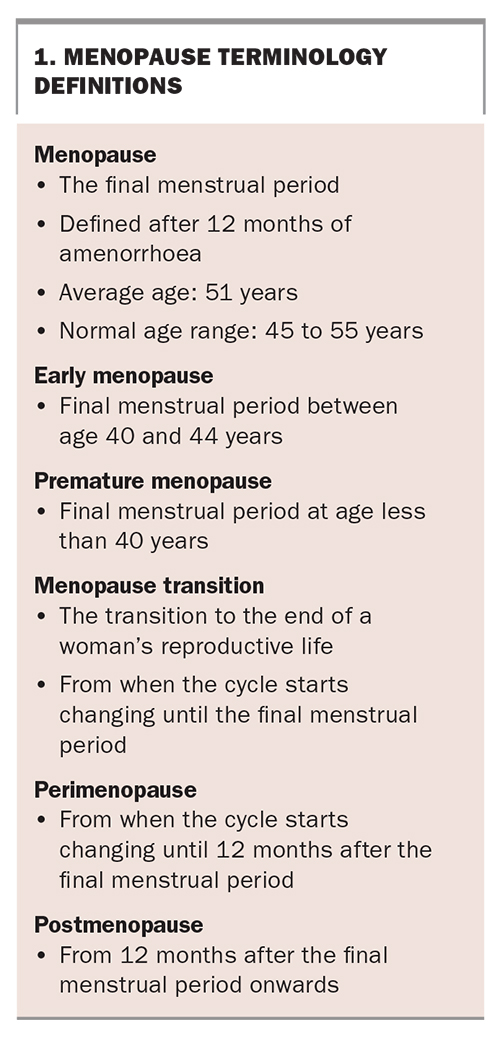
The States of Reproductive Aging Workshop (STRAW) +10 criteria are internationally agreed criteria for stages of reproductive ageing (Figure).2 According to these criteria, perimenopause starts when there are persistent differences in cycle length of seven days or more between consecutive cycles. During perimenopause, symptoms of both oestrogen excess and deficiency can occur. The primary criteria are clinical rather than biochemical, and diagnostic blood tests are not usually recommended for women at the usual age of menopause. Perimenopause continues until 12 months after the final menstrual period. Box 1 outlines the definitions of menopause, early menopause, premature menopause, menopause transition, perimenopause and postmenopause.
{kind=link}
{kind=link}
For some women, criteria that rely on menstrual cycle changes cannot be used. This includes women who have a levonorgestrel intrauterine device (IUD) or use other hormonal contraception, and those who have had an endometrial ablation or hysterectomy. For these patients, perimenopause is heralded by symptoms rather than menstrual changes. Biochemical confirmation with follicle stimulating hormone (FSH) testing is always recommended for women under age 45 years who are experiencing symptoms consistent with perimenopause or early menopause, as well as consideration of other causes such as hyperprolactinaemia or thyroid disease. Women who have a surgical menopause (removal of the ovaries prior to natural menopause) do not undergo perimenopause.
What are the symptoms of perimenopause?
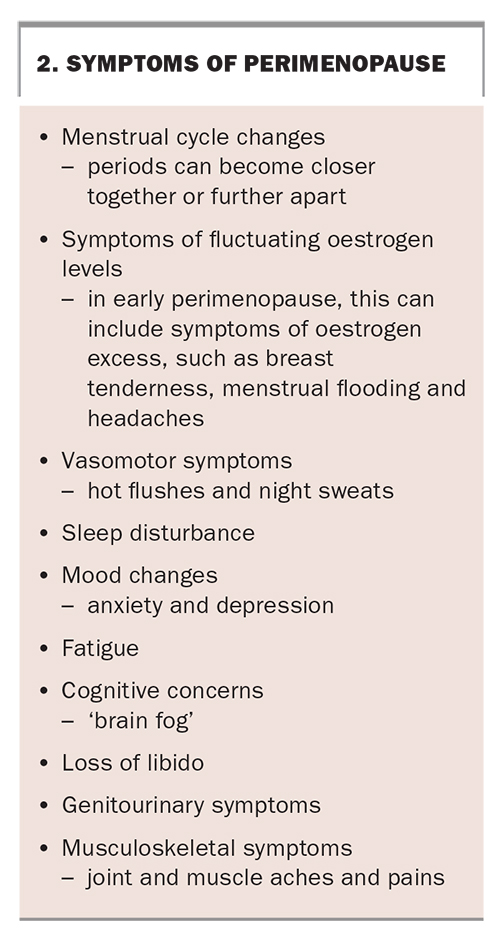
At perimenopause, hormones fluctuate, and women can experience a variety of symptoms (Box 2). In addition to symptoms, risk factors for chronic disease begin to change during perimenopause. This includes an acceleration of bone loss, which begins at the earliest onset of the menopause transition.3 There is also an increase in cardiovascular risk factors, including central adiposity, adverse changes in lipids and changes in glucose metabolism.4
{kind=link}
A structured approach to assessment in perimenopause
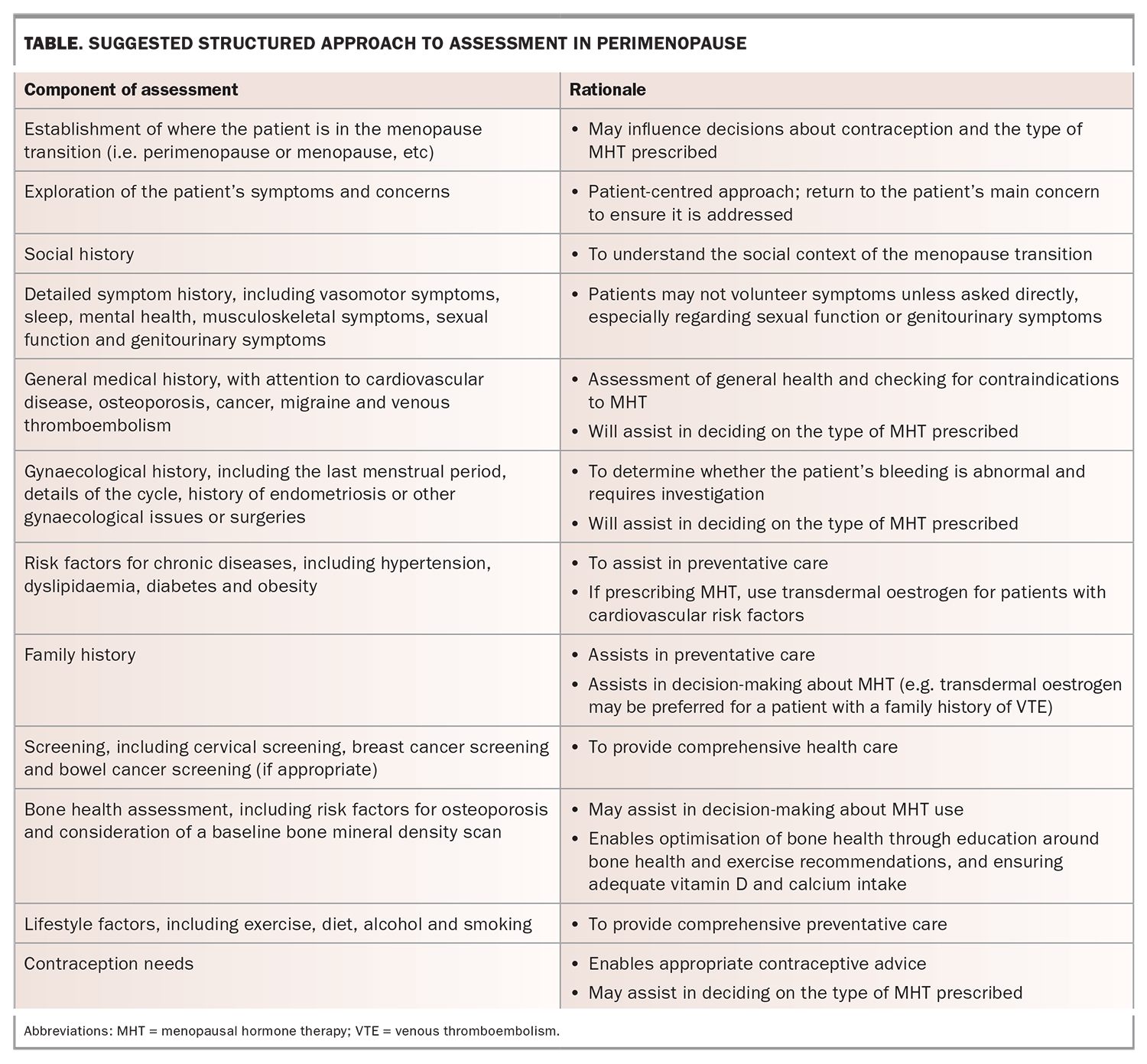
Women can present to GPs with a range of symptoms and concerns, and it can be helpful to perform a systematic assessment. A suggested approach is provided in the Table, with particular reference to decision-making about MHT. Women with early or premature menopause need specific assessment, which is detailed elsewhere.5
{kind=link}
Assessment of bleeding
Perimenopause is characterised by a change in the menstrual cycle. Cycles can become longer or shorter, and periods can become heavier or lighter.
It is important to have a low index of suspicion for investigation of abnormal bleeding, particularly for women with a history of obesity or polycystic ovarian syndrome. Any abnormal bleeding must be investigated before starting MHT. Bleeding that is longer or heavier than usual, intermenstrual, erratic in timing, or postcoital must be investigated, along with any bleeding that occurs after 12 months of amenorrhoea. Women should be examined and tests should be performed as appropriate. This may include cervical co-testing or testing for sexually transmitted infections. Transvaginal ultrasound should be performed, ideally within seven days of a bleed, and further management guided by the findings. Some women will need gynaecological assessment, for example, hysteroscopy and biopsy in cases of heavy, prolonged or unexplained bleeding or if the endometrium is thickened on ultrasound. Guidance on assessment of bleeding is available online (https://www.menopause.org.au/hp/information-sheets/postmenopausal-bleeding-including-breakthrough-on-mht-hrt).
Mental health considerations
The incidence of mood disturbance is higher at perimenopause than in the earlier reproductive years, particularly for women with a history of hormone-related mood disorders, such as premenstrual dysphoric disorder or postnatal depression.6 Patients need a full assessment and comprehensive approach to management, including psychological therapies and lifestyle advice. Along with antidepressant medications, MHT can be considered as a treatment option for some of these women.7
Contraception
Fertility declines during perimenopause, with changes in cycle length and an increase in anovulatory cycles. However, ovulatory cycles can still occur in an unpredictable pattern, necessitating reliable contraception.8 The rate of unplanned pregnancies is relatively high in women aged in their 40s.9 Contraception is recommended for two years after the final menstrual period for women aged under 50 years and for one year for those aged over 50 years.10 Options include long-acting reversible contraceptives such as the etonogestrel implant and the levonorgestrel IUD. These methods, along with progestogen-only pills, can be used until menopause. The new drosperinone 4mg pill, taken in a format of 24 out of 28 days, is a progestogen-only contraceptive option that often causes anovulation. It has high contraceptive efficacy and is usually associated with good cycle control. It can be used for contraception until menopause. The progestogen-only methods will not address menopausal symptoms and cannot be used as the opposing progestogen to oestrogen therapy (with the exception of the 52 mg levonorgestrel IUD).
The combined oral contraceptive pill (COCP) can be used by women aged under 50 years in the absence of contraindications and may provide relief from vasomotor symptoms. COCPs with oestradiol formulations and a short or no unmedicated phase may be particularly suitable. The combined vaginal contraceptive ring is another option for eligible women.
The 52 mg levonorgestrel IUD can be used for the endometrial protection component of MHT for up to five years. However, the 19 mg levonorgestrel IUD, the progestogen-only pills and the etonogestrel implant cannot be used for endometrial protection.11 A discussion about contraception provides an opportunity to discuss the importance of safe sex for patients.
Deciding when it is safe to stop contraception can be a dilemma. For women aged over 50 years who are using progestogen-only method and who have had amenorrhoea for 12 months since turning 50 years old, a single FSH test can be performed. If the FSH level is greater than 30 IU/L, women may stop contraception after a further 12 months of use. If it is less than or equal to 30 IU/L, women should continue using contraception and can retest again after a further 12 months.10
Approach to symptom management
The most effective treatment for menopausal symptoms is MHT. Nonhormonal treatment options can also be discussed, for example, cognitive behavioural therapy for vasomotor symptoms. Herbal and complementary medications have insufficient evidence of efficacy. Prescription medications, including antidepressants, may be of benefit and can be offered to patients with contraindications to MHT or those who do not want to take hormones.12 All women can benefit from lifestyle advice and health promotion.
How to prescribe MHT
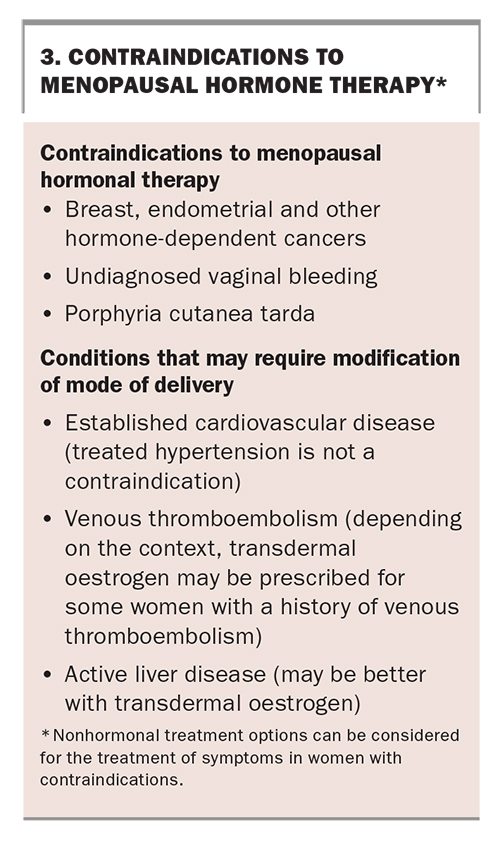
The principal indication for prescribing MHT is for the relief of symptoms, and it can be offered to symptomatic women who do not have contraindications (Box 3). It is not necessary for symptomatic women to wait until menopause to use MHT. A consideration of whether contraception is needed is crucial to appropriate selection of treatment.
{kind=link}
The primary component of MHT is oestrogen, which should be prescribed at the lowest effective dose. Generally, oestrogen should be started at a low dose and increased as needed to manage symptoms. Women with an intact uterus also need a progestogen to prevent endometrial hyperplasia. When starting MHT less than 12 months after the final menstrual period, the progestogen should be cyclical or sequential. This means that the progestogen is given for 12 to 14 days per month, with a bleed occurring at the end of the progestogen phase. Continuous combined MHT and other options, such as tibolone and tissue selective oestrogen complex (oestrogen with selective oestrogen receptor modulators), are not suitable for commencement during perimenopause because of the high incidence of unscheduled bleeding.
Several preparations with fixed combinations of oestrogen and cyclical progestogen are available in tablet or transdermal forms. Another option is to prescribe transdermal or oral oestrogen combined with a separate prescription for a progestogen, which is taken for 12 to 14 days per cycle.
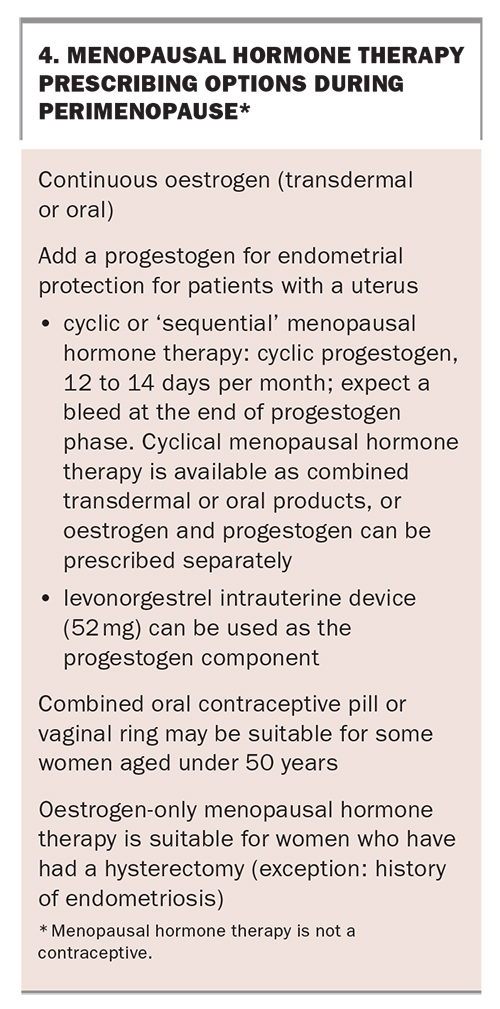
For women with heavy or irregular bleeding during perimenopause, conventional MHT may not control the cycle adequately. In these circumstances, the 52 mg levonorgestrel IUD or the COCP may be suitable options (after appropriate investigation of the bleeding). The 52 mg levonorgestrel IUD can provide contraception, endometrial protection and management of heavy or irregular bleeding, and an oestrogen can be added for the management of perimenopausal symptoms. The COCP may effectively control erratic cycles during perimenopause and vasomotor symptoms. It can be prescribed for women aged less than 50 years in the absence of contraindications. It may be best taken continuously or with long cycles to avoid emergence of symptoms during the placebo phase. An oestradiol-containing preparation may be preferable. Box 4 outlines prescribing options for systemic MHT during perimenopause.
{kind=link}
Options for MHT available in Australia, including appropriate doses of progestogens to match oestrogen doses, are available online (https://www.menopause.org.au/hp/information-sheets/ams-guide-to-equivalent-mht-hrt-doses). Women taking cyclical MHT often experience irregular bleeding or spotting in the first few months. Sometimes the regimen needs to be adjusted. If unscheduled bleeding persists beyond six months of commencement of MHT, it should be investigated.
Genitourinary symptoms can commence during perimenopause and topical vaginal oestrogen is an effective treatment, in addition to nonhormonal options, such as lubricants. Women with systemic symptoms will often find that MHT improves their symptoms, but some also need additional topical oestrogen. For women who only have genitourinary symptoms, vaginal oestrogen alone is appropriate.
Benefits and risks of MHT
The primary goals of prescribing MHT are to improve symptoms and to reduce bone loss and fracture risk.1 However, in the clinical consultation, the focus is often on potential risks. The findings of the Women’s Health Initiative (WHI) trials were first published 20 years ago. The combination of oestrogen (conjugated equine oestrogens) and progestogen (medroxyprogesterone acetate) was associated with an increase in breast cancer, cardiovascular events and venous thromboembolism (VTE).13 Since then, our understanding of the benefits and risks of MHT has evolved. The findings of this study, in which participants were enrolled at an average age of 63 years and were given oral oestrogen and a synthetic progestogen, have limited relevance to women currently considering using MHT for symptoms during perimenopause.14 Most studies of MHT have been in women who were postmenopausal at the time of enrolment and it is unknown whether the risks of MHT apply in the same way to women starting MHT during perimenopause.
Analysis of the WHI and other studies in recent years has found that, for women starting MHT when aged less than 60 years or within 10 years of menopause, the risks of MHT are very low. In fact, this group had a reduction in coronary heart disease and myocardial infarction at long-term follow up.15 There is increasing support for the ‘timing hypothesis’, whereby women who start MHT close to the time of menopause derive cardiovascular benefit, whereas those who start many years after menopause do not.16,17
Oral oestrogen is associated with an increased risk of VTE; however, transdermal oestrogen is not.18-20 Transdermal oestrogen is the preferred option for women with risk factors for VTE or cardiovascular disease.21
Observational studies indicate that neutral progestogens, such as micronised progesterone and dydrogesterone, are likely to be safer for the breasts and cardiovascular system than the older synthetic progestogens.22,23 Micronised progesterone is available as a capsule and dydrogesterone is available in combination with oestradiol in tablet form.
Oestrogen is effective in the prevention of bone loss and osteoporotic fracture and is an appropriate antiresorptive therapy for this age group.13,24 Women with a family history of osteoporosis, or who themselves have osteoporosis or low bone density, should be made aware of the protective effect of MHT on bones.
Conclusion
Perimenopause can present challenges for women and their clinicians. Most women who are symptomatic can be offered MHT during perimenopause, after a detailed discussion of the risks and benefits. When starting MHT, women with a uterus should have sequential progestogen. All women benefit from assessment, management of contraceptive needs, screening activities and a discussion about healthy lifestyle. MT