Perinatal depression and anxiety

Although pregnancy and birth should be, and often are, a time of great joy for new and expectant parents, many struggle with mental illness during this period. Universal screening for perinatal depression and anxiety in this population can help ensure affected women and partners receive the support and treatment they need, which may include medication, inpatient care in a mother–baby unit or community support.
The perinatal period can be defined as the period from conception to the end of the first postnatal year. For most women and their partners, this is a time of joy and happiness. However, for many it can be a complex and stressful time of adjustment, and a significant number of women, and men, develop a mental health disorder during the perinatal period. This may manifest as an exacerbation of existing mental illness, an adjustment disorder, post-traumatic stress disorder, postnatal psychosis, or perinatal depression and anxiety (PNDA).
Anxiety and depression during the perinatal period are diagnosed using the same criteria as outside of pregnancy and should not be confused with transient ‘baby blues’, which usually only last a few days. PNDA is characterised by a substantial change of mood that lasts for two or more weeks, affects usual functioning and is accompanied by anhedonia. This article focuses on PNDA and how GPs can support women and men who are experiencing this disorder.
Prevalence of perinatal depression and anxiety
Although its prevalence is variously reported, PNDA is observed to affect one in five women and one in 10 men.1,2 This means it is common, affecting 100,000 families in Australia each year.
Although there are many recognised risk factors for PNDA, most overlap with those established for other mood disorders, bearing in mind the specific context (e.g. pregnancy or birth complications, sleep deprivation). What is perhaps less well appreciated is the recognition that becoming a parent is a life-changing event. This factor alone underpins PNDA’s lack of discrimination and its equal prevalence across all socioeconomic and cultural groups. For this reason, screening for PNDA should be universal for everyone going through pregnancy.
Sequelae of PNDA
If untreated, PNDA can have important sequelae. Fifty to 70% of mothers with depression will remain depressed after six months, while 25% will experience chronic depression and 25% will have recurrent depression.3 PNDA can lead to disruption of personal relationships, including marriage breakdown. It can have a negative impact on other children in the family and cause intergenerational trauma. Mother–infant attachment may be compromised. Evidence suggests that maternal PNDA is adversely associated with the child’s development.4 There is also some evidence for a small increase in the incidence of preterm birth and low-birthweight infants when mothers have PNDA. Suicide is the leading cause of maternal death in the year after giving birth in Australia and many other countries.
Screening for PNDA
A biopsychosocial model interprets medical conditions by recognising the interconnection between biological, psychological and socioenvironmental factors. As a person’s mental health is not isolated from their experiences, screening for anxiety and depression should also include a psychosocial assessment that seeks to understand the individual in the context of their past and present history and social, economic and relational circumstances.
In many countries, universal mental health screening and psychosocial assessment during pregnancy have been recommended as best practice. Australia is a recognised leader in this field, with published national guidelines.5 Uniquely, in Australia, the Medicare Benefits Schedule mandates this screening for all pregnant women. It has been implemented in most public hospitals, but uptake of universal screening programs in the Australian private hospital system has been slower. Resistance to screening from private hospital health practitioners is widespread, because of time factors, inadequate remuneration, practitioner discomfort or lack of expertise, poorly defined referral pathways and a lack of resources if a mood disorder is identified.6
Ideally, mental health screening and psychosocial assessment using a recommended screening tool should be conducted twice during pregnancy. Given the recognised constraints, GPs can use the opportunity presented by each antenatal and postnatal encounter to enquire about emotional health. The Centre of Perinatal Excellence (www.cope.org.au) provides resources for health professionals, including screening tools, perinatal mental health fact sheets and advice about best practice and referral.
Screening tools
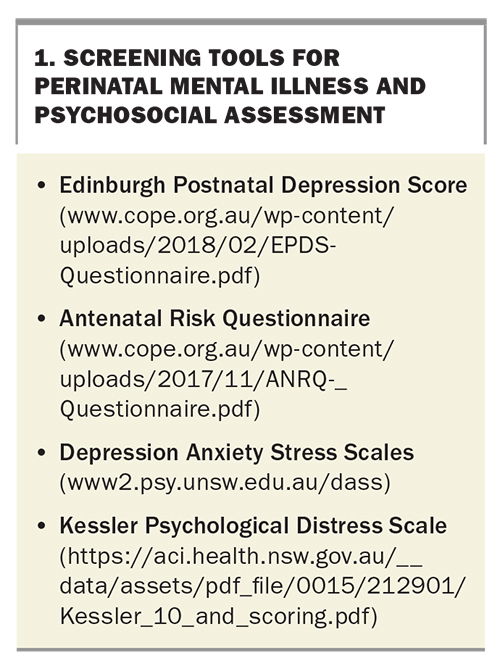
Two screening tools are commonly used in PNDA screening: the Edinburgh Postnatal Depression Score (EPDS) and the Antenatal Risk Questionnaire (ANRQ) (Box 1).
{kind=link}
The EPDS is a 10-item self-report measure that is designed to screen women for symptoms of emotional distress during pregnancy and the postnatal period.7 It is not diagnostic and must always be used in conjunction with clinical assessment. The EPDS includes one question (item 10) about suicidal thoughts, which mandates further action if positive. As it reflects the woman’s experience in the past seven days, the EPDS may need to be repeated as clinically warranted.
The ANRQ is a 13-item structured questionnaire with categorical (yes/no) and dimensional (five options) responses, which generates a total psychosocial risk score, indicating cumulative risk.8 It also identifies specific risk factors (history of trauma or significant mental health condition) that independently put a woman at greater psychosocial risk. The ANRQ covers the woman’s relationship with her partner, social support, recent stressful life events, anxiety or perfectionism, history of depression or other mental health conditions (and treatment for these), experience of abuse as a child or an adult and quality of relationship with her own mother during childhood.
Other screening tools include the Depression Anxiety Stress Scales (DASS) and Kessler Psychological Distress Scale (K10) (Box 1). The DASS are a set of three self-report scales designed to measure the negative emotional states of depression, anxiety and stress. The K10 is a simple measure of psychological distress that is also used to measure outcomes after treatment for common mental health disorders.
Management
As PNDA can have an adverse effect on the child’s development, it is a key target for prevention and early intervention to support new mothers and safeguard the health and wellbeing of their children.4 The principles of management for PNDA are similar to those for other mental illnesses and include interventions such as cognitive behavioural therapy, interpersonal psychotherapy, medication and hospitalisation. Where possible, the approach to all management should include the family unit.
Perinatal Anxiety and Depression Australia (PANDA) offers resources for health professionals (https://panda.org.au/learn/learn-health-professionals), including helpful fact sheets on available interventions and advice on encouraging disclosure of PNDA and making effective referrals.
Medication
Selective serotonin reuptake inhibitors (SSRIs) and serotonin and noradrenaline reuptake inhibitors (SNRIs) are highly effective for treating anxiety and depression during pregnancy. Criteria for starting medication during pregnancy and lactation should be based on the usual clinical indications, allowing for fetal safety concerns.
Although the data are limited, there is reassuring evidence of maternal and neonatal safety with SSRIs and SNRIs.9 Some studies report a small, statistically insignificant increase in birth defects for SSRIs and SNRIs, with higher doses of paroxetine being specifically associated with cardiovascular anomalies. There is a clinically insignificant association of SSRIs and SNRIs with low birthweight and premature delivery. Neonates should be monitored for signs of withdrawal, poor neonatal adaptation syndrome and, rarely, persistent pulmonary hypertension, all of which are usually transient and self-limiting. Because SSRIs are highly protein bound, transfer through breastmilk is negligible, and breastfeeding should be supported. Long-term data on neurodevelopmental effects are problematic and confounded by the impact of untreated maternal mental health disorders.
Some perinatal psychiatrists prefer to prescribe fluoxetine, with its longer half-life and potential for slower neonatal withdrawal effects, but others prefer shorter-acting SSRIs or SNRIs (citalopram, fluvoxamine or sertraline), as the mother’s response may be faster.9
Patients and clinicians can obtain advice about pharmacological exposure during pregnancy and lactation from the organisations listed in Box 2.
{kind=link}
Other interventions
Dedicated inpatient mother–baby units provide safe short- and longer-term opportunities for multidisciplinary mental health treatment. Access to inpatient care varies from state to state; for instance, Victoria is well-resourced, but there is only one public unit and one private unit in NSW.
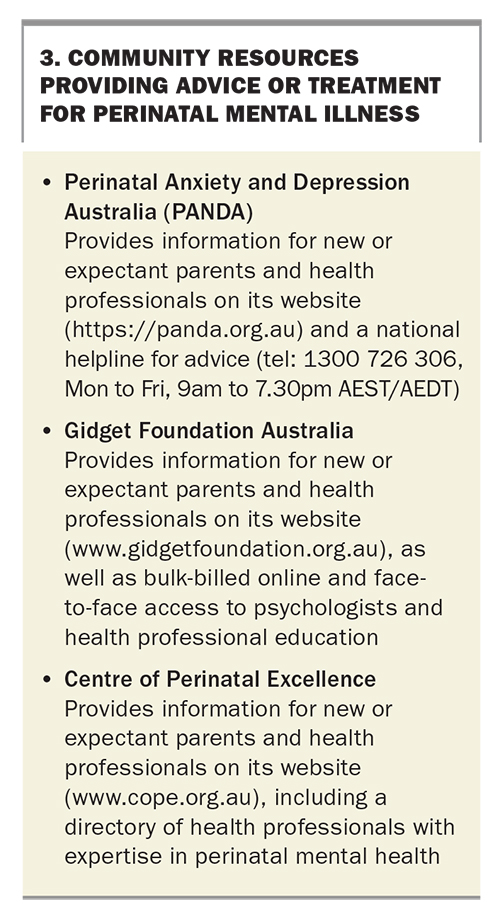
There are valuable community resources that can provide advice or treatment (Box 3). Importantly, GPs should also be aware of nonmedical adjuncts, such as mothers’ groups, support from friends and family (e.g. grandparents), financial support options and assistance with domestic chores. As with all mental health care, diet, exercise and other lifestyle factors should be discussed and addressed.
{kind=link}
Referral
It is important for GPs to identify appropriate health professionals for referral, such as clinical psychologists or perinatal psychiatrists, so that established referral pathways are readily available when needed. Referral is not always appropriate, and many women will prefer that management remain with their GP, as their known and trusted healthcare provider. Referral should be considered if there are acute concerns about maternal or infant health and safety. Untreated perinatal depression is associated with pre-eclampsia, low birthweight and prematurity, as well as an increased risk of adverse effects on the mother and child.10
Conclusion
Perinatal mental health disorders are common and distressing for parents and their children. The impact can be profound for the individuals affected, their families and the wider community, including social and economic costs.
Changing the paradigm in perinatal mental health requires adequate funding and other resources. However, this will be insufficient without a significant accompanying cultural shift in our attitudes towards pregnancy and parenting. We should not detract from the fact that, for many women and their partners, pregnancy and the arrival of a baby is a time of great joy, a journey of excitement and happiness that is celebrated in all communities. A newborn is a source of wonder, love and adoration for their parents and the family and friends around them. Rather, medical practitioners, and the community at large, should accept the alternative paradigm that mental illness can complicate the experience of pregnancy and parenting and seek to identify and manage the disease as an inherent part of medical care. MT
COMPETING INTERESTS: Dr Roach was previously the Chair of Gidget Foundation Australia.