Beware of allergic reactions to stings and bites

Allergy
Stings and bites from insects and ticks commonly cause allergic reactions, ranging from a local swelling to major anaphylaxis. Each patient responds in a unique way and the best course of action must be determined, taking several factors into account, including identification of the offending insect and the severity of the reaction.
- Life-threatening allergic reactions to stings or bites from insects and ticks are relatively common.
- The insects responsible include honey bees; paper, mud and European wasps; and ants.
- Allergic reactions to bites and stings develop rapidly, peak quickly and usually ease within a day or two.
- Adverse reactions range from large local swellings arising from the sting or bite site to systemic responses confined to the skin and anaphylaxis.
- The most effective method to reverse anaphylaxis is an injection of adrenaline. Killing embedded ticks in situ reduces the risk of allergic reaction.
Australia has a wide diversity of stinging and biting insects and arachnids capable of causing severe life-threatening allergic reactions. Measures are available to prevent these events and treat patients when reactions do occur. This article deals with terrestrial but not marine creatures, nor does it deal with the occasional anaphylaxis to snake venom in heavily exposed snake handlers.
Specific immunotherapy is readily available in Australia to reduce the risk of anaphylaxis to bees and some wasps and, in some states (Tasmania, South Australia and Victoria), to jack jumper ants (JJAs). The accepted term now is venom immunotherapy – it does not ‘reverse’ anaphylaxis but reduces the risk of anaphylaxis to future envenomation events.
What is allergy?
A simple definition of allergy is an adverse immediate specific immune response to an external substance. In this context, it is typically abrupt, explosive and brief. Such immediate generalised (allergic) reactions (IGR) begin within 30 to 60 minutes (sometimes in 30 seconds) of exposure and may involve multiple systems in rapid progression. If the patient survives the insult, the reaction will usually ease in a few hours.
How common is allergy to stings and bites?
Allergic reactions to stings and bites from insects and ticks result in a significant degree of morbidity in the community. Overseas experience indicates that the prevalence of life-threatening stinging insect allergy ranges from 0.5 to 7%.1-3 In Australia, almost 5% of the Tasmanian population have had an IGR to a sting, while 6.5% of South Australians self-reported a history of systemic reaction to insect sting.4,5 In South Australia, Tasmania and Western Australia there are 7.5 to 10.6 hospitalisations per 100,000 people per annum as a result of bee stings alone, but the figures in the other states are much lower.6-8
Australian records show that at least one or two people die each year from either bee, wasp or ant stings.7,9 Deaths from tick allergy have also occurred.7 Deaths are likely to be substantially underestimated because of under-reporting, frequently unwitnessed occurrences of stings and bites and poor sensitivity of autopsy for anaphylaxis.10,11
Who is likely to be allergic to insect stings or bites?
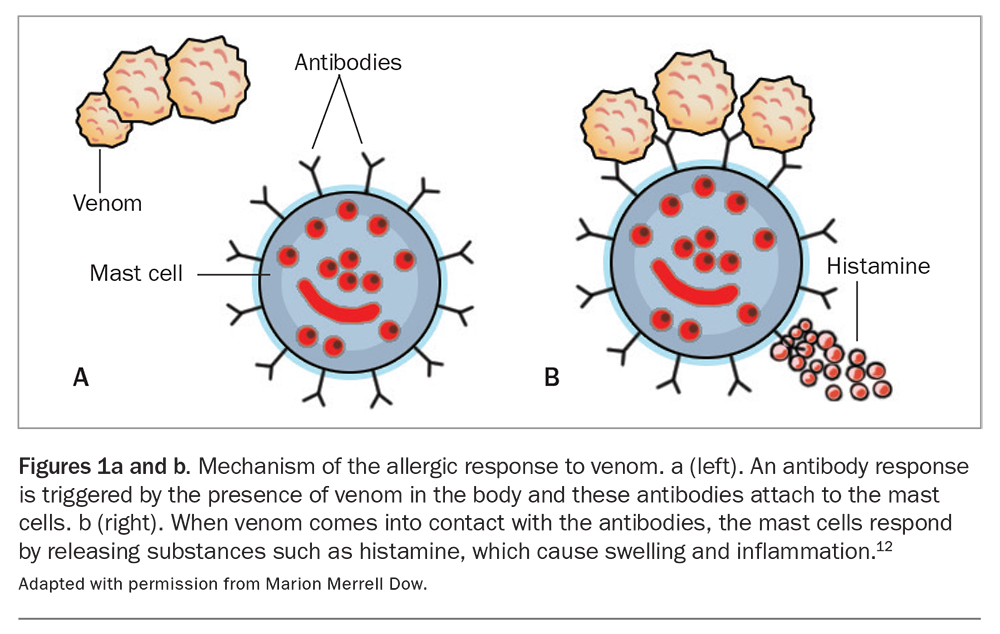
Allergic reactions are determined by genetics and exposure. As a rule, an individual patient will react only to a particular insect species; that is, a patient who has had a severe reaction to a bee sting is most unlikely to react similarly to a wasp sting. An exception to this is that there is significant cross-reactivity between different vespid (wasp and hornet) species. Furthermore, it is almost impossible to experience an allergic response to the first sting from a particular insect. Thus, the patient undergoes a priming or sensitising period in which he or she tolerates one or more stings but is primed to react to a subsequent sting from that species (Figures 1a and b).12
{kind=link}
Species responsible for allergic reactions
All the stinging insects belong to the order Hymenoptera. Allergic reactions occur to the venoms these insects produce. Insects whose stings may cause allergic reactions include:
- European honey bees (Apis mellifera)
- paper wasps with paper nests (Polistes and Ropalidia spp.)
- wasps with mud nests (Sceliphron sp.)
- hornets (Vespa sp. – true hornets), which are not established in Australia
- European wasps, which usually have nests in the ground (Vespula germanica and, in Victoria, Vespula vulgaris)
- Australian ant species: JJAs (Myrmecia pilosula), other bull/inch ants (about 90 species of predominantly larger Myrmecia), greenhead ants (Rhytidoponera metallica) and others13
- the red imported fire ant (Solenopsis invicta) – first recorded in Queensland and targeted for eradication.
The March fly (family Tabanindae) and the paralysis tick (Ixodes holocyclus; an arachnid) are biting (rather than stinging) insects which produce salivary proteins that can cause allergic reactions.
Types of reactions
Responses to insect stings and tick bites vary widely.
Sensitisation
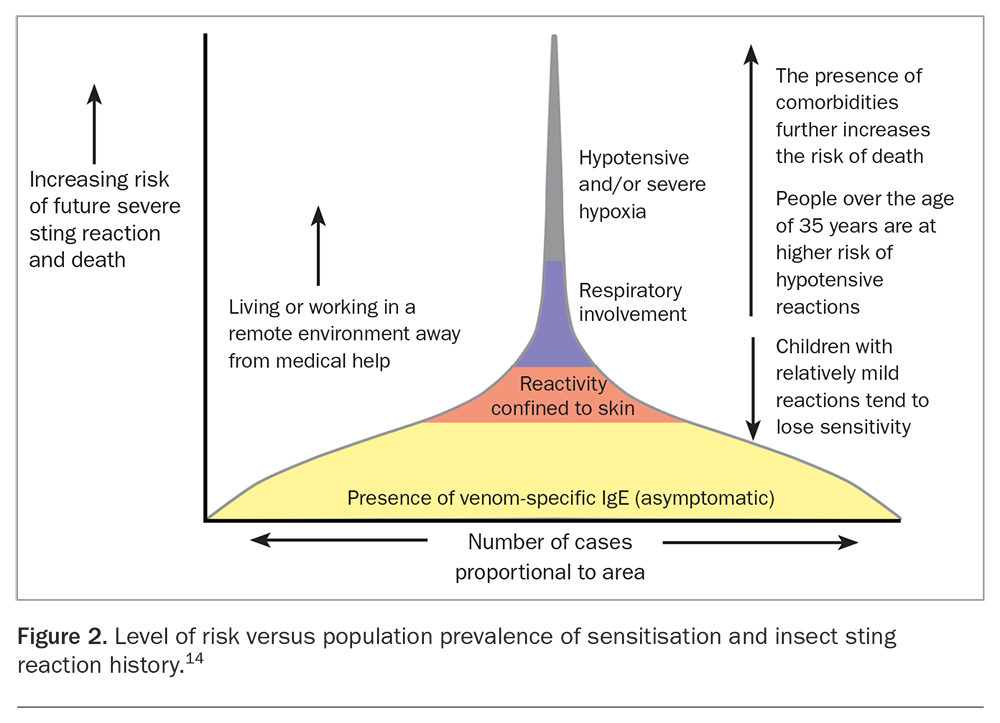
It must be recognised that far more people are sensitised with specific IgE antibodies to the venoms of prevailing Hymenoptera species than have had or will have systemic reactions to stings from these same species (Figure 2).14-16
{kind=link}
Clinical reactions
There are four primary categories of clinical reactions to stings and bites from insects and ticks.
Normal response
A normal response to an insect sting or tick bite is characterised by a burning or painful wheal up to several centimetres in diameter confined to the sting or bite site. It usually resolves in a few hours or days.
Large local swellings
A large local swelling may develop from the sting site and may vary enormously in extent. A sting on the hand, for example, may result in swelling of the entire hand or extend to the elbow, or even to the shoulder or neck. The durations of these reactions vary widely, some resolve within hours, whereas others persist for many days. These reactions may be toxic or allergic, and evolve within 30 minutes or may take up to 24 hours. Allergy-induced large local swellings may develop rapidly and are mediated by the specific antivenom allergic antibody.16
Minor IGR
A minor systemic response involves parts of the body distant from the sting site but without clinically significant cardiovascular or respiratory involvement. The most common manifestation is a reaction confined to the skin (generalised urticaria and/or facial angioedema). Gastrointestinal symptoms are often seen in patients with evolving hypotension, and should not be regarded as mild symptoms in the context of a sting or bite.17
Major IGR/anaphylaxis
In a major systemic response, body organs vital to life (i.e. the respiratory or cardiovascular systems) are impaired by the anaphylactic response. A common response is that within a few minutes of being stung or bitten (e.g. on the arm), the patient may develop facial pruritus or flushing. This is followed quickly by pruritus and then frank urticaria elsewhere on the body. The patient may develop gastrointestinal symptoms or become extremely apprehensive with a sense of imminent death, feel so weak that he or she cannot stand, may lose vision, collapse, become unconscious and/or dyspnoeic, with a choking sensation or chest tightness, or even all of the above. Some patients may develop acute hypotension with collapse or dyspnoea without a rash or swellings. Uterine cramping, which may be the dominant complaint, can be as severe as labour pain.
Risk of a major response
As a general rule, each individual has a unique way of responding to a sting or bite. Therefore, if a minor systemic response has occurred, a subsequent sting or bite will most likely result in a similar reaction.4,16,18 Occasionally, patients may progress from a large local swelling to a minor systemic event or even a major response. Stings on the head or neck do not necessarily put a patient at a higher risk of a major reaction than stings occurring on lower parts of the body, although one study reported a higher rate of systemic reactions in patients who had been stung on the neck or trunk.19,20
As indicated in Figure 2, patients who have never had an adverse response have a low risk of experiencing a future IGR.14 Those with a history of large local reactions have a risk of experiencing a future IGR of about 5 to 10%, whereas those who have had systemic reactions to bees or wasps limited to the skin have up to a 20% risk (lower in children). Many of these IGRs will be minor. However, patients who have already had an anaphylactic reaction to a sting have a 40 to 60% chance of reacting the same way to any future sting from the same species, whereas in JJA allergy it is consistently around 70%.4,16
Rarely, patients may experience serum sickness, a neurological reaction or vasculitis. Occasionally, a patient may have a major systemic reaction after being stung by many insects at the one time. Some may be toxic events but in the absence of allergy, healthy adults can tolerate vast numbers of stings and many of these reactions appear to be allergic.19 Thus, this group has a high risk of anaphylaxis if re-stung by a single insect from the same species.
Reactions to insect and arachnid stings and bites
European honey bees
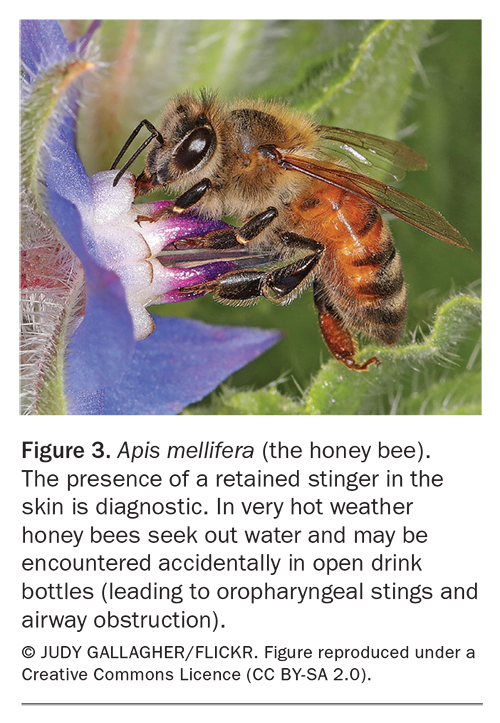
Hospitalisations and deaths due to stings from honey bees (A. mellifera; Figure 3) occur disproportionately in ‘western climates’ of Australia, specifically in Western Australia and South Australia.6-8,10 Immediate systemic reactions to honey bee stings do not peak in spring as expected but with high maximum temperatures.21
{kind=link}
Wasps
Australia has numerous species of paper wasps. They are prevalent in the northern half of the continent. Clinical experience indicates that some patients show allergic reactivity to only certain species of wasps. The two major species in Australia are: Polistes, which build a rosette type of nest, and Ropalidia, which build a nest of two long columns. Diagnostic problems arise because the only available test and immunotherapy reagents come from the USA and are prepared from the American species of Polistes. Thus, about 30% of patients who clearly have had anaphylaxis from wasp stings fail to show positive tests and consequently are not currently candidates for specific immunotherapy.22 European wasps (predominantly V. germanica; Figure 4) are prevalent in cooler urbanised areas of Australia.14,23
{kind=link}
Ants
Australian ants
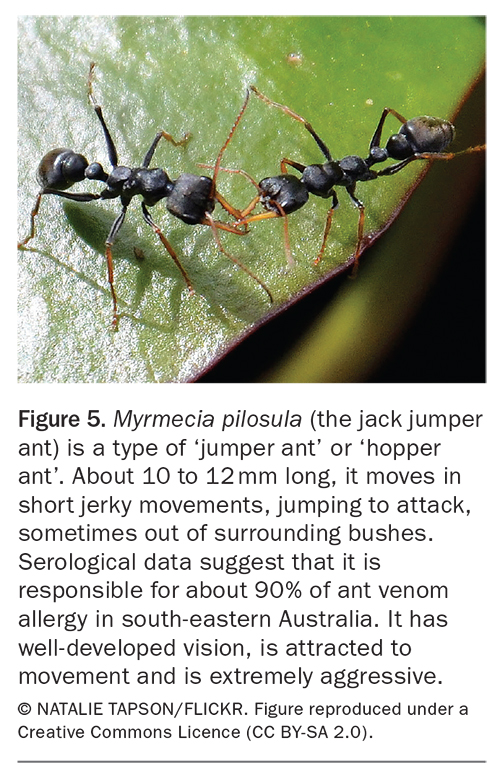
Most ants do not sting but Australia, with its uniquely rich ant fauna, has seven genera of ants capable of inflicting sting anaphylaxis. The native M. pilosula species complex (JJA, a type of jumper/hopper/skipper ant; Figure 5) appears to be the dominant cause of anaphylaxis in many cooler areas of Australia, with hot spots in Tasmania, southern Victoria and the Adelaide Hills.4,13,24 In both sting and epidemiological studies, recurrence rates in people with a history of severe generalised reactions have been consistently 70% or more across several studies.4,25 Multiple deaths have been reported.26,27 In the hinterland of Sydney and further north in Queensland, a morphologically similar jumping ant with a red thorax (Myrmecia nigrocincta) is found. In the far south of Western Australia another type with different coloured hind legs (Myrmecia ludlowi) can be found.
{kind=link}
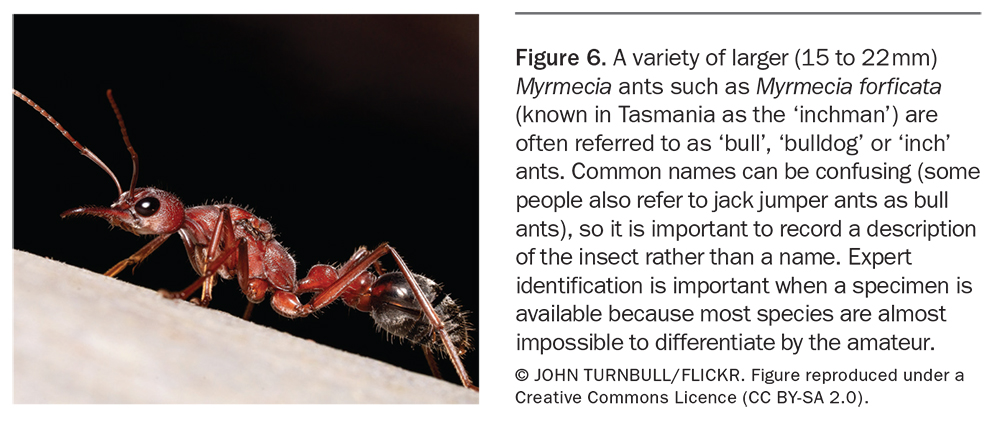
Most of the about 90 species of Myrmecia might aptly be termed ‘inch ants’, and they are larger and less aggressive than M. pilosula and are often nocturnal (Figure 6). Despite occupying diverse habitats across Australia and some nearby Pacific islands, including one species in New Zealand, these diverse ants are less prominent as causes of anaphylaxis than M. pilosula.13
{kind=link}
The Myrmecia diverged from other hymenopterans about 30 million years ago. To date significant cross-reactivity with other stinging hymenopterans has not been demonstrated.
Nothomyrmecia macrops (found rarely in the west of South Australia) appear largely unchanged in fossil records for about 200 million years (personal communication, R. Taylor) and predate many early dinosaurs.
The red imported fire ant
The red imported fire ant (S. invicta) is tiny (2 to 6 mm) and forms huge colonies. It originated from South America and later infested extensive areas of the southern states of the USA. It has been very difficult to eradicate and has caused destruction of farmlands and parks. Many people have incurred anaphylaxis from the stings and there have been fatalities. Red imported fire ant colonies were detected in south-east Queensland in the late 1990s. Eradication programs have been carried out. Two workers in the field developed anaphylaxis early in the program.28 However, although red imported fire ants have since been detected in New South Wales, Western Australia and (again) Queensland, incursions have been subject to subject to a nationally cost-shared eradication program and efforts to contain red imported fire ant colonies have been reasonably successful.29
Ticks
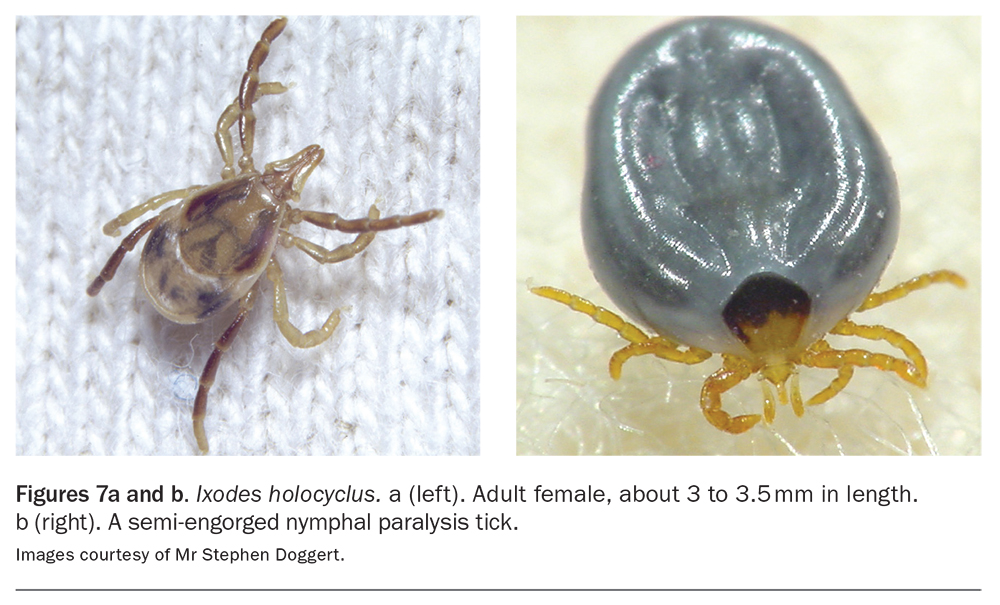
The paralysis tick (I. holocyclus; Figures 7a and b) infests almost the entire eastern seaboard of Australia. Anaphylaxis has resulted in many patients, with fatal outcomes in four cases.30 The most prevalent areas of infestation are the northern beaches of iSydney, the northern rivers of New South Wales and the hinterland of southern Queensland. The tick embeds its mouth parts in the skin and the allergic reaction occurs when the tick is disturbed in situ (i.e. if it is pulled out or even if it is scratched), which causes release of more saliva.
{kind=link}
Red meat allergy is quite rare but it has been described relatively commonly in people who have had previous tick bites, possibly even in those who have not had an adverse event. Further studies have shown that the tick’s saliva contains a carbohydrate, galactose-alpha-1,3-galactose (alpha-gal), that is found in almost all mammalian meats. This is a unique allergen because all other allergens are proteins.31,32
Diagnosis
Identification of the offending insect
Identification of the inciting insect needs to take account of the geographical location, circumstances of the sting and observations made at the time. Honey bees leave a ‘stinger’, which is not a feature of wasps or ants recorded in Australia. European wasps have ground nests and are attracted to sweet foods, so a person may be stung at a picnic by a wasp in a soft drink. Jumper ants have a very characteristic appearance, movement and aggression and can sting through even thick textiles. March flies typically stay at the site. Ticks are embedded in the skin.
Assessment of reaction severity
Assessment of the severity of the reaction should take account of the history and any objective observations, particularly vital signs after the event. Note that patients may recover spontaneously and that observations made on arrival at care may underestimate peak reaction severity. Alternatively, objective observations may show that a reaction was far more serious than the history would suggest.
Confirmatory objective tests
There are two types of tests to confirm an allergic reaction:
- in vivo skin tests
- in vitro serological tests for specific venom IgE antibodies.
In vitro tests are available only for the specific venoms of honey bees, some paper wasps, European wasps and M. pilosula (through SA Pathology) but not for the salivary allergens of March flies or ticks. The preponderance of asymptomatic sensitisation relative to clinical reactivity means that the testing of patients with no history of a systemic allergic reaction will result in many positives with very poor positive predictive ability for clinical reactivity.
If doubt exists as to the causative insect, serological testing for venoms of as many as possible of the locally prevalent insects should be performed. However, the level of reactivity on skin or in vitro testing does not predict the severity of the clinical reaction.16
Skin tests
Specific venom extracts from bees and wasps, not whole-body extracts, must be used. They are available as freeze-dried powders and reconstituted with a diluent of albumin-buffered saline.
Testing for allergy to the venom of the M. pilosula species complex is the same as for bees and wasps. However, it is only available under special conditions requiring TGA, local hospital and Royal Hobart Hospital Pharmacy approval.
Testing is preferably deferred for two weeks after an anaphylactic event because some patients have a short refractory period in which allergen-specific antibodies may not be detected.33
Venom skin testing requires expertise in terms of venom selection, performance and interpretation, and intradermal tests carry a risk of anaphylaxis. Although the risk of anaphylaxis is relatively low, testing should be performed by practitioners experienced in these areas and who are prepared to manage anaphylaxis, whether to the testing venom or subsequent venom immunotherapy.
In patients with severe clinical reactions, the initial test may be a skin prick test at 1.0 mcg/mL. If this is negative, intradermal testing should be performed, starting at 0.01 mcg/mL. If negative, further testing should be performed at 15-minute intervals using increasing concentrations (0.1 and finally 1.0 mcg/mL) until a positive response is found.
In vitro tests for specific IgE
In vitro tests for specific IgE (previously called RAST tests) detect unbound venom-specific IgE antibody in serum. There is generally a close correlation between skin test reactivity and circulating allergen-specific IgE, but discordant results may occur.
Positive results with poor correlation and clinical reactivity to vespid and honey bee venoms may occur in atopic patients with high total IgE levels from IgE antibodies to common carbohydrate found widely in plant materials, including pollen, as well as in bee and wasp venoms. If such a result is suspected, an immunology laboratory should be contacted for advice on further testing using recombinant allergens.
False-negative results also occur in both skin testing and in vitro tests, especially with wasp venoms. A patient who is negative in one test should be assessed by the other test and the test repeated one to two months later before being declared ‘negative’.33 If the tick-associated red meat allergy is suspected, a serological test for alpha-gal is usually positive.
Other tests for sting anaphylaxis
Mast cell tryptase
Mast cell tryptase, a relatively stable product of mast cells, is released at a steady rate and maintains a stable serum level throughout life unless there is widespread mast cell activation or a mast cell disorder. The level rises within 15 to 30 minutes of onset of a major systemic allergic reaction and typically remains elevated for about eight hours. However, failure of elevation does not exclude anaphylaxis (especially in food allergy).
The sensitivity and specificity of testing is increased by comparing the acute level with a convalescent level as increases of at least 20% over the individual baseline and at least 2 ng/mL (absolute value) appear to be a sensitive and specific marker for sting anaphylaxis.34,35 If the baseline tryptase level is raised and irrespective of whether classical urticaria pigmentosa is present, a mast cell disorder may be present, representing a special risk factor for sting anaphylaxis.36-38
Sting challenges
Sting challenges carry a significant risk of anaphylaxis and can give false-negative results, in part because venom delivery is highly variable.39 They are not recommended in routine practice.33
Minimisation of risk of envenomation
To minimise the risk of being stung or bitten by insects or ticks, people should:
- be aware of likely circumstances and localities of insects or ticks concerned
- maximise clothing protection
- avoid provoking insects or ticks.
Honey bees
People should be aware of the likely presence of honey bees, especially around water in hot dry conditions. If stung the stinger should be flicked out as soon as possible. If left in situ, the venom sac will deliver 90% of its contents within 30 seconds.39
Wasps
People should be aware of the presence and attraction of European wasps to food and sweet drinks. Some areas have effective Vespula control programs.
M. pilosula species
It is more difficult to protect against stings of M. pilosula, which is highly aggressive, able to leap from vegetation to humans and can sting through thick textiles. Moving is an option if a suitable area free of JJAs can be found but in South Australia this insect is being found in previously unsuspected locations. Although it is a protected native insect essential to pollination of some native orchids (Leporella fimbriata), insecticide treatment of nests close to homes is often chosen as a way of reducing the risk of being stung.
Ticks
Tick-infested areas should be avoided. If time is spent in these areas, clothing should be removed and placed in a hot dryer. Careful searches of the body, especially the scalp, should be performed because ticks may take up to two hours to attach. Some insect repellents containing N,N-diethyl-meta-toluamide (DEET) may discourage ticks.
If a tick is found embedded in the skin it should not be disturbed. Ideally it should not even be scratched, which of course may be difficult to do. It must not be pulled out, because forcible extraction causes more saliva to be released into the skin. The most effective method of reducing the risk of an allergic reaction is to kill it in situ. Ether has been shown to kill ticks rapidly.
Furthermore, once dead the tick will desiccate and may fall out by itself or can be easily scraped out with a credit card or a blunt knife without a reaction occurring. Products containing ether, including Aerostart, which is well known to mechanics, and sprays containing dimethyl ether used to freeze warts are recommended.
Treatment
Large local swellings
Large local swellings represent very intensive inflammatory events. Oral antihistamines and topical corticosteroids are often ineffective. An oral NSAID or single dose of oral corticosteroid will usually suppress the reaction rapidly.
Minor systemic reactions
An oral antihistamine should be sufficient for minor systemic reactions. It should be noted that this will not prevent a major systemic response.40
Rapid-onset systemic reactions
First aid treatment
First aid treatment of rapid-onset systemic reactions has been revolutionised by the ready availability of automated adrenaline injectors designed for lay use. Adrenaline is the only medication shown to work rapidly after onset of a systemic reaction.40,41 Even in patients with stable vascular disease, the risks of a small intramuscular dose of adrenaline through an automated adrenaline injector are likely to be far less stressful than hypotension and/or hypoxia.
All patients with a history of a rapid-onset systemic reaction to a sting or bite should have an automated adrenaline injector and an action plan (plans and e-training are available at www.allergy.org.au). In controlled sting studies, hypotension is the most common serious outcome.41,42
A patient experiencing anaphylaxis should be kept supine or supine with legs raised, and allowed to sit if breathless, but not allowed to stand.11,40 Once the autoinjector has been used, an ambulance should be called. After stabilisation following anaphylaxis, the patient should be held for medical observation so that appropriate treatment can be given if the reaction re-emerges as the effect of adrenaline diminishes. Rural patients need a prearranged plan for linking to emergency services.
Medical treatment
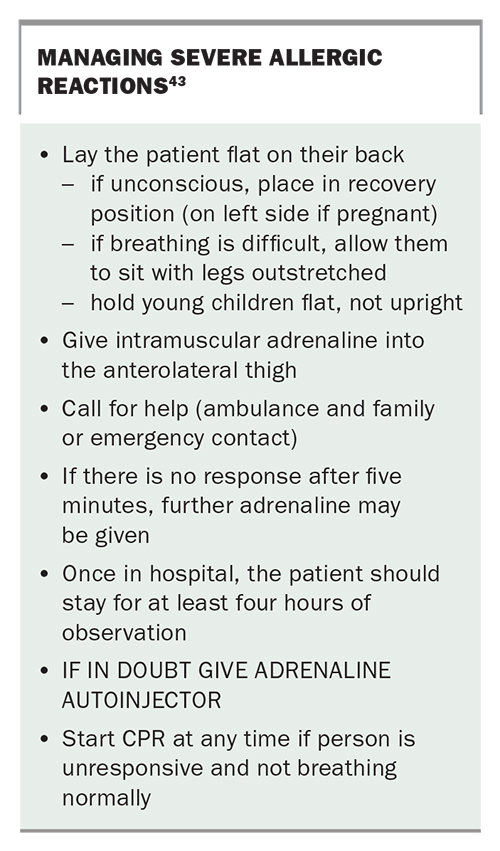
For an excellent practical review of the management of anaphylaxis, readers are referred to the Australasian Society of Clinical Immunology and Allergy (ASCIA) action plans for anaphylaxis (https://www.allergy.org.au/hp/anaphylaxis/ascia-action-plan-for-anaphylaxis). Key measures are summarised in the Box.43 Intramuscular adrenaline into the anterolateral thigh gives peak levels within a few minutes more reliably than subcutaneous administration.40 Intravenous adrenaline by infusion is a procedure that should only be performed by those with high-level resuscitative skills. In patients with hypotension, posture and fluid resuscitation with normal saline is important as massive fluid losses can occur in anaphylaxis through both redistribution and extravasation of fluid from the vascular system.32 Patients who have had a major reaction should be held for at least four hours after stabilisation and the last dose of adrenaline, in order that any re-emergent reaction can be dealt with appropriately. A patient who has required adrenaline to treat a reaction or who has been assessed by a clinical immunologist or allergist, respiratory physician or paediatrician as at risk of further anaphylaxis qualifies for a PBS-subsidised automated adrenaline injector, which must be given with an action plan. Medic Alert bracelets should be considered.
{kind=link}
Venom immunotherapy
Risk assessment
Venom immunotherapy is a long-term treatment requiring a significant commitment of time and having a significant comorbidity. Therefore, a careful assessment needs to occur.1 The risk of an anaphylactic reaction to a further sting can be estimated (Figure 2). Any adult with a history of an IGR, even if confined to the skin, and any child with a history of anaphylaxis should be considered at high risk of serious reaction to a future sting from that species.2 Exposure level and geographic location must be considered.4
Comorbidities and their treatments need careful assessment because there are several that may add to the risk of adverse outcomes from a further sting and to the potential difficulties of venom immunotherapy. Although signalling a need for caution and often expert assessment of the comorbidity and its treatment, such comorbidities add to the case for venom immunotherapy in expert hands because the risks of graded doses of venom given in carefully controlled conditions are likely to be substantially less than a sting away from medical care.36
Comorbidities thought to contribute to risk are mast cell disorders, often presenting as hypotension without rash, disorders that involve vascular or respiratory compromise.36,38 The use of some antihypertensives (such as beta-blockers and ACE inhibitors) is no longer considered a generic risk factor for more frequent or severe anaphylaxis to venom stings or immunotherapy, although whether they still pose a risk for specific individuals is subject to debate.36-38,44,45 Judgement and often co-management are required in assessing the risk and benefit of, and alternatives to, these agents.
Giving venom immunotherapy
The principle of venom immunotherapy is that by giving carefully graded doses of the relevant venom subcutaneously, clinical reactivity is greatly reduced. Diverse mechanisms account for this effect, which is venom specific, but controlled studies have involved honey bees, wasps and JJAs. Trials of venom immunotherapy with honey bee, vespid or JJA venom leave no doubt that such therapy is effective in reducing (by about 90%) the probability of having a rapid-onset systemic allergic reaction to another sting from the same species.25,46,47 Even the ‘failures’ are almost always milder than the index reaction.47 The specificity of the therapy, morbidity (including risks of anaphylaxis, especially with the more convenient accelerated regimens and venom type) and duration of therapy required for long-term benefit mean that such therapy should be selected, initiated and guided by a trained allergist or clinical immunologist.37,48
Adults who have experienced rapid-onset generalised allergic reaction, even if confined to the skin, and children who have had such a reaction extending beyond the skin qualify for venom immunotherapy, provided that there is evidence of specific IgE (by venom skin testing or in vitro testing) to the relevant available venom and informed consent acknowledging the duration and side effects of the therapy. In general, children with reactions limited to the skin and adults with large local reactions or asymptomatic sensitisation do not qualify for therapy because the risk of future anaphylaxis to sting in such patients is small (<10%; Figure 2).14
Until maintenance doses of venom are reached, venom immunotherapy carries a risk of rapid-onset allergic reactions sufficient that a specialist most appropriately carries this out. The risk varies with insect venom, being higher for honey bees, paper wasps and JJAs than ‘European’ wasps (Vespula sp.), and with regimen. It is nevertheless always significant.25,37,47,49
Stopping venom immunotherapy is problematic. Patients who have tolerated five years of maintenance venom immunotherapy without systemic adverse reaction appear to have protection that usually persists for many years, even when some IgE to venom remains detectable. However, it has been estimated that after stopping venom immunotherapy, there is about a 10% chance of loss of protection with each subsequent sting.16 Patients who have experienced reactions that were life-threatening with hypotension and/or hypoxia (rather than reactions that might have evolved to that stage), cardiorespiratory compromise at baseline, a mast cell disorder, frequent stings or redevelopment of allergy following a previous adequate-duration course of venom immunotherapy should be continued on indefinite venom immunotherapy. Clearly, the decision to stop venom immunotherapy is nuanced, and should involve the clinical immunologist or allergist.
Honey bee and European and paper wasp extracts are available through the PBS. JJA venom is only available under special conditions requiring TGA, local hospital and Royal Hobart Hospital Pharmacy approval (contact Jenny Gudden, Operations Manager, Jack Jumper Ant Allergy Program, Royal Hobart Hospital). JJA venom immunotherapy in Australia and red imported fire ant venom immunotherapy in North America are the only ant allergies with established desensitisation treatment protocols. There are no March fly or tick extracts available for immunotherapy.
Conclusion
Anaphylactic events are common. In some, the cause may be obscure; thus stinging insects and ticks should be considered among the many possible causes. A careful history must be taken and if insect or tick allergy is likely, it would be useful to do a preliminary serological test for allergy to the specific venom. If the patient has experienced a systemic reaction, a major or minor, and even if the blood test is negative, a referral to an allergist or immunologist is necessary. In addition, an automated adrenaline injector and action plan should be promptly provided on an authority prescription. Patients should be made aware that it is possible in some cases to suppress the allergy by specific venom immunotherapy. MT