Recombinant zoster vaccine for immunocompromised people

People who are aged 50 years and older or who are immunocompromised are at increased risk of herpes zoster and are recommended to receive zoster vaccine. The live attenuated zoster vaccine recommended for immunocompetent adults is contraindicated in severely immunocompromised populations, who are instead recommended to receive the recombinant zoster vaccine (RZV). The indication for RZV in Australia has been recently extended to immunocompromised patients aged 18 years and older, and RZV is now recommended as the safer and more efficacious vaccine in at-risk populations.
Herpes zoster (HZ) is caused by reactivation of the varicella zoster virus (VZV) from the dorsal root or trigeminal nerve ganglia, resulting in a characteristic papulovesicular dermatomal rash and moderate to severe neuritic pain. This pain may persist as postherpetic neuralgia (PHN), defined as pain beyond 90 days after onset of the rash. Reactivation is controlled by specific immunity, especially T-cell mediated immunity, which declines with age in the phenomenon of ‘immunosenescence’.
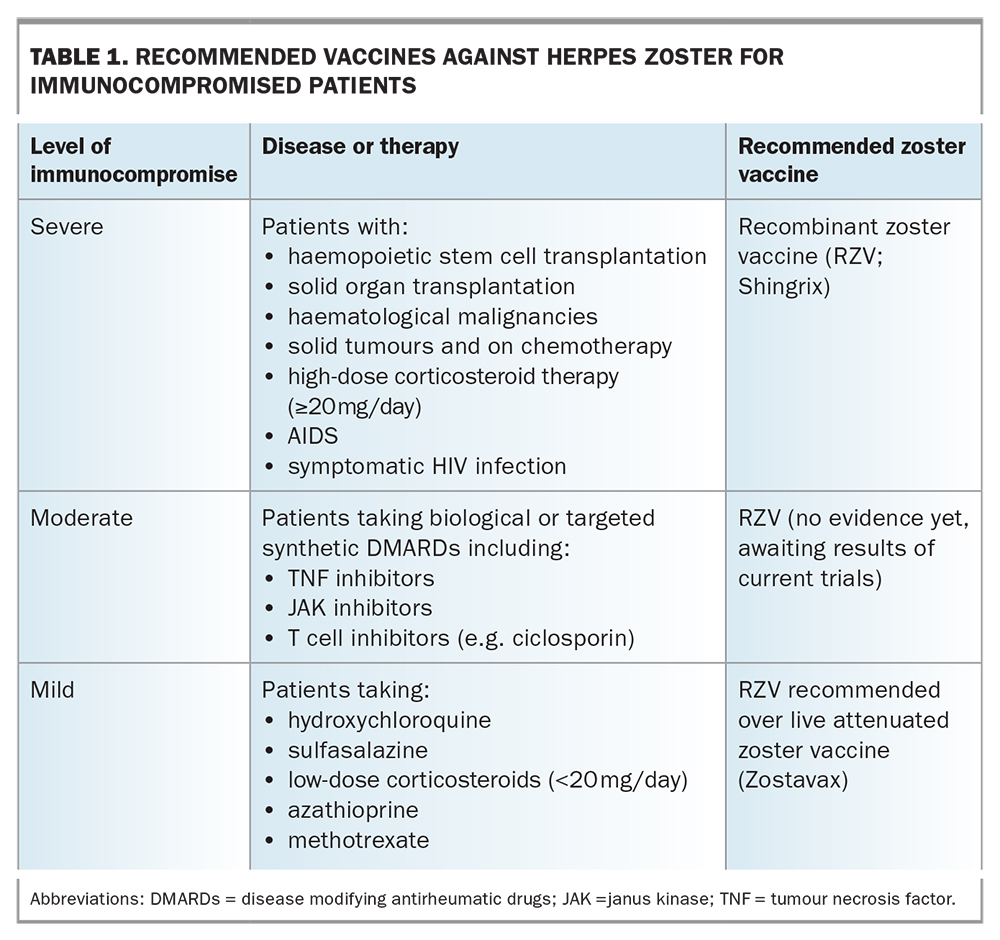
One in three people will experience HZ over their lifetime, rising to one in two over the age of 85 years. Indeed, the risk of HZ increases markedly with age, from 3 to 5 per 1000 person years for the general adult population to above 10 per 1000 person years for those aged over 70 years in almost all countries surveyed.1,2 People who are moderately to severely immunocompromised are also at increased risk of HZ, including those with haematological or other malignancies, HIV infection or AIDS, those undergoing solid organ transplantation (SOT) or haemopoietic stem cell transplantation (HSCT) and those receiving immunosuppressive drugs such as 20 mg/day or more of prednisolone or equivalent for over two weeks (Table 1).
{kind=link}
Herpes zoster in immunocompromised patients
In immunocompromised patients, the incidence and severity of HZ increases proportionately with the degree of immunosuppression. Highly immunocompromised patients receiving allogeneic or autologous HSCT have an HZ incidence of 8 to 28% in the first year after HSCT and are at increased risk of visceral dissemination. HZ incidence is reported as 22 to 32 per 1000 person years in SOT recipients and up to 14 per 1000 person years in patients with a solid tumour receiving chemotherapy. Before the advent of antiretroviral therapy, the risk of HZ in people with HIV infection was 10-fold higher (32 per 1000 person years) than in the age-matched population, and it is still two- to threefold higher than the age-matched population, especially in people with CD4+ T cell counts below 200 cells/mcL and HZ complications, including recurrent episodes are still threefold higher than in the age-matched population.1,3
Immunisation against herpes zoster
Immunisation against HZ in people older than 50 years can prevent VZV reactivation by restimulating waning VZV-specific T cells and antibodies. In Australia, the live attenuated zoster vaccine (Zostavax) is licensed for immunocompetent people aged 50 years and older and funded under the National Immunisation Program for those aged 70 to 79 years. The Australian Immunisation Handbook recommends a single dose of Zostavax for people aged 60 years older, especially those aged 70 to 79 years, and for those aged 50 years and older who are household contacts of a person who is, or is expected to become, immunocompromised.4 Zostavax is not routinely recommended for immunocompetent people aged 50 to 59 years.4 Zostavax consists of varicella vaccine concentrated 14-fold. However, as a live attenuated vaccine, it is contraindicated in moderately to severely immunocompromised people, leaving a major gap in HZ prevention for this vulnerable population.5
The recombinant zoster vaccine (RZV)Shingrix has been available for people aged 50 years and older, whether immunocompromised or not, since June 2021 and is now preferred over Zostavax.6 Although no head-to-head comparisons between the two vaccines have been done, RZV had an efficacy against HZ of more than 90% in clinical trials, even in people aged over 80 years, and this efficacy persisted at 84% for up to seven years.7-9 The trials of the live attenuated zoster vaccine showed an overall efficacy of 51% against HZ, declining to 38% in those aged over 70 years, and to 4 to 32% over eight years.10-12 Interestingly, the efficacy against PHN was greater, at 66.5%, and longer lasting.
A new indication for the recombinant zoster vaccine
In line with recommendations in other countries such as the USA, Canada and Europe, the availability of RZV has been recently extended in Australia to patients aged 18 years and older who are at increased risk of HZ – that is, to those who are moderately to severely immunocompromised. The suitability of RZV for at-risk populations is summarised in Table 1.
RZV consists of only a single highly immunogenic VZV surface protein, glycoprotein E, which is produced efficiently using recombinant technology. The glycoprotein is combined with immunostimulants, an adjuvant system (AS01) consisting of the toll-like receptor 4 agonist monophosphoryl lipid A and the saponin QS-21, all encased within a liposome. After intramuscular injection, RZV drains rapidly to the axillary lymph nodes and initiates a marked immune cascade involving many cell types and molecules to stimulate antiglycoprotein E (gE) specific antibodies and T cells. The adjuvant is crucial for the vaccine’s marked efficacy and responsible for increasing T-cell responses from 10 to 90% in people over the age of 70 years. As RZV is not a live vaccine, it is safe for immunocompromised patients.2
RZV efficacy and immunogenicity in immunocompromised people
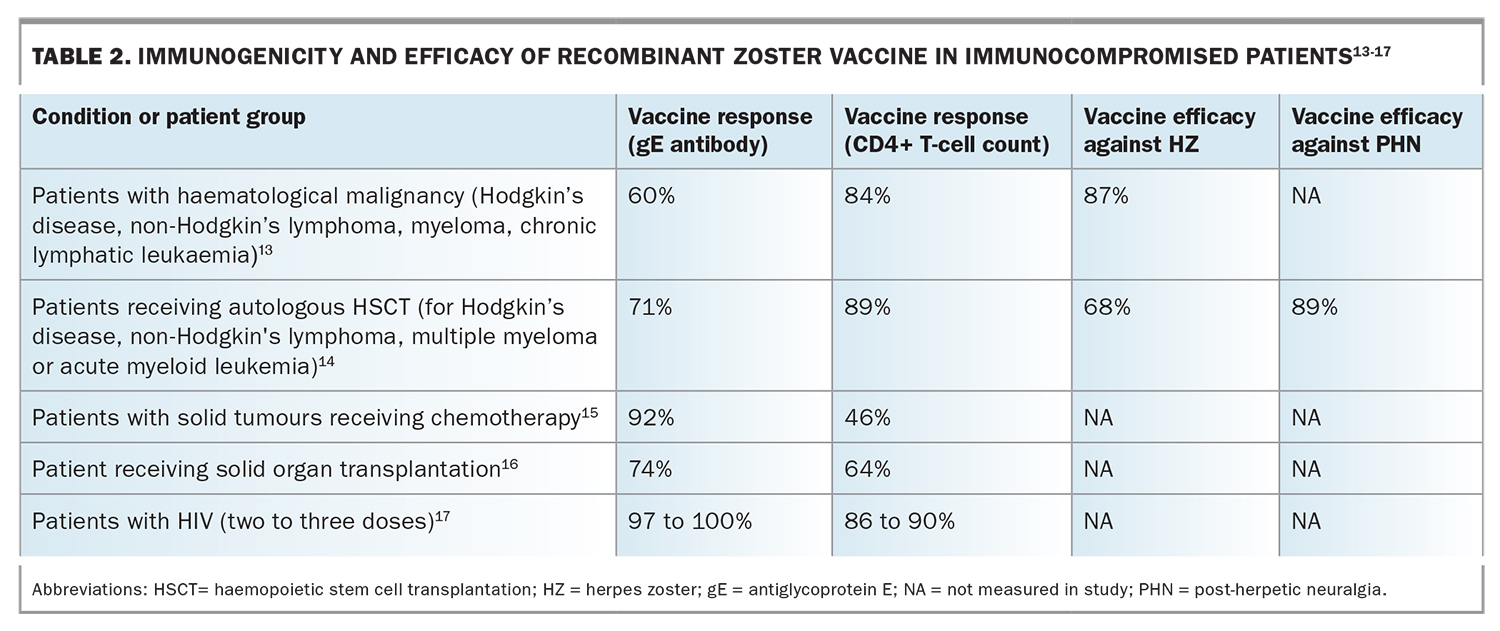
Evidence for the immunogenicity, reactogenicity, safety and efficacy of RZV in moderately to severely immunocompromised patients has been obtained from five key phase II and III clinical trials, summarised in Table 2.13-17 The vaccine was administered at zero, two and six months in patients with HIV infection and at zero and one to two months for four other patient groups (patients receiving autologous HSCT or SOT and those with haematologic malignancy or solid tumours with chemotherapy). Follow up was at 18 months for the HIV group and 12 months for the others.
{kind=link}
In patients aged 18 years and older (of whom 73% were aged over 50 years) with haematological malignancies (Hodgkin’s disease, non-Hodgkin’s lymphoma, myeloma, chronic lymphatic leukaemia), RZV was administered before or after chemotherapy. Significant vaccine responses were seen in this patient group (T cell in 84% and gE antibody in 60%). Post hoc analysis showed vaccine efficacy against HZ was excellent at 87%.13
In the largest trial, patients were immunised 50 to 70 days after receiving autologous HSCT for Hodgkin’s disease, non-Hodgkin's lymphoma, multiple myeloma or acute myeloid leukaemia. This patient group showed excellent vaccine responses (T cell in 89% and gE antibody in 71%), very good efficacy against HZ (68%), and excellent efficacy against PHN (89.3%), other complications (77.8%) and hospitalisation (84.7%). Patients receiving rituximab for B-cell lymphomas and chronic lymphocytic leukaemia had lower antibody levels but unchanged vaccine efficacy.14
RZV was immunogenic for more than a year among all patient groups. In those with SOT, the T-cell response was 64% and gE antibody response was 74%.16 Immunogenicity was lowest in patients with solid tumours receiving chemotherapy, with a T-cell response of 46% and a gE antibody response of 92%.15
In the HIV trial, patients were stratified into three subgroups according to CD4+ T-cell count. In patients with HIV infection, the vaccine induced strong gE antibody and T-cell responses that persisted until the end of the 18-month study, irrespective of CD4+ T-cell level or whether patients were on antiretroviral therapy. The third dose did not add to immunogenicity.3,17
RZV reactogenicity and safety in immunocompromised people
In the above trials, reactogenicity was similar to that seen in immunocompetent patients and there were no vaccination-related severe adverse effects.13-17 Reactogenicity (or adverse effects) at the injection site for immunocompromised patients in all five of these trials was only moderately increased (75 to 85%) compared with immunocompetent patients aged over 50 years and over 70 years (84% and 79%, respectively).7,8 Systemic reactogenicity was markedly increased in all five immunocompromised patient groups (67 to 83%) but was offset by the marked increase in recipients receiving placebo (46 to 79%). Severe or ‘grade 3’ local or systemic reactions were relatively mildly elevated at 10 to 20%.13-18
Future research
More research on RZV in immunocompromised patients is still needed, including the completion of phase III trials in patients receiving SOTs and those with solid tumours receiving chemotherapy. Also, the durability of immunogenicity and vaccine efficacy beyond 12 to 18 months is still to be determined for all five groups.
When patients cannot immediately receive RZV, such as after HSCT, antiviral prophylaxis for HZ with valaciclovir or famciclovir should be continued until peak immunogenicity is attained. For example, in the trials in patients with HSCT, RZV was administered in two doses: 50 to 70 days after receiving HSCT and one to two months thereafter.14 Peak immunogenicity was seen one month after the second dose.
The US Centres for Disease Control and Prevention recommend patients receive RZV at least three to 12 months after HSCT and, if possible, before transplantation or chemotherapy. If this is not possible then RZV is recommended when immunosuppression is reduced.19
Currently, there are few data on the safety and efficacy of RZV in patients with autoimmune diseases who are being treated with biological and synthetic disease modifying drugs (DMARDs), especially agents with an immunosuppressive effect on T-cell responses, such as mycophenolate; however, trials are in progress. Studies of RZV coadministration with COVID-19 vaccines are also urgently needed. Future research on the mechanism of action of RZV may lead to the development of RZV-like vaccines with reduced reactogenicity but retention of immunogenicity and efficacy, as there is only a weak correlation between the two effects.
Conclusion
The incidence of HZ increases in immunocompromised patients, with severity proportional to the degree of immunosuppression. Immunisation with RZV can help protect against HZ. The live attenuated zoster vaccine, which is recommended for immunocompetent adults, is not suitable for those who are moderately or severely immunocompromised. Instead, at-risk populations are recommended to receive RZV, which has been shown to be safe and effective against HZ. Recently, the indication for RZV has been extended in Australia to include immunocompromised adults aged over 18 years. MT
COMPETING INTERESTS: Professor Cunningham has received honoraria for consultancies from GSK, Seqirus and Merck, paid to his institution.