Finding the cause of sudden leg weakness
Neurological diseases
Sudden weakness of the legs is a presenting symptom which requires urgent attention. ‘Sudden weakness’ not only refers to weakness that is acutely obvious over seconds, hours or days. In some cases, weakness may have been coming on over weeks, discounted by the patient, who then presents with ‘apparently sudden weakness’.
- ‘Sudden’ weakness can be interpreted to mean weakness that becomes obvious over seconds, hours, days or weeks.
- Important diagnostic clues, such as localised spinal tenderness or an extensor plantar response, can be revealed during a brief physical examination.
- A thorough neurological examination will also evaluate the appearance, tone, power and sensation of the face, neck, trunk, arms as well as the legs.
- Rapid progression of weakness, ascending from legs to the arms and face, or leg weakness with back pain and urinary retention, are indications for urgent referral.
- An acute lesion of the spinal cord may be accompanied by ‘spinal shock’ which may obscure the distinction between an upper and a lower motor neuron lesion.
- Common causes of sudden leg weakness include drop attacks, the Guillain–Barr syndrome and nontraumatic spinal cord compression due to metastatic tumour or an epidural abscess.
Reaching a neurological diagnosis involves answering the questions: ‘Where is the problem?’ and ‘What is the cause of the problem?’. To answer these questions, a working knowledge of the nervous system’s gross anatomical structures, its physiology, and some common patterns of disease and symptom presentation is necessary. A careful history and physical examination as described below often gives the diagnosis which points to appropriate management pathways (Flowchart). Initial investigations should not delay urgent referral for neurologist or emergency department review, particularly if leg weakness or bladder involvement are rapidly evolving (see Box, Indications for urgent referral). If weakness is caused by acute spinal cord compression, rapid neurosurgical decompression to preserve function is usually required. Other causes of acute ascending paralysis (e.g. from postinfectious neuropathy or a metabolic disorder such as hypokalaemia) require cause-specific intervention.
History
The presenting illness
The approach to analysing sudden leg weakness is based on answering the following questions:
- What is the temporal profile of this weakness? Has it occurred over seconds to minutes, over hours to a day or two, or progressed over weeks? (Table 1)
- How and when has the weakness affected walking or running, going up and down stairs, and getting up from a squatting position or a chair?
- Has there been a previous episode of similar weakness?
- Is the weakness symmetrical? Did it begin in one or both legs?
- Is there any associated sensory disturbance or ‘level’ which can help localise the lesion?
- Is there back or leg pain? (Local back pain may indicate infection or compression; however, back pain can also occur with transverse myelitis, Guillain–Barré syndrome, and diabetic radiculopathy or plexopathy.)
- Is there any associated bladder or bowel dysfunction?
- Does neck flexion cause weakness or tingling into the legs?
- Is the problem stable, progressing or improving?
Other systems
Other questions related to general systems enquiry are also important, with an emphasis on recent illness, particularly infections, vaccinations, vascular disease, possible malignancy and collagen vascular disease.
Drug history
A history of drug use – for example, of heparin or neurotoxic drugs (such as chloroquine, colchicine, cytotoxics), muscle toxic drugs (such as heroin, alcohol) and exposure to chemical toxins such as arsenic, thallium and herbal cathartics containing podophyllin, may be relevant.
Family history
A family history may be crucial – for example, in cases of familial hypokalaemic periodic paralysis. Hypokalaemic periodic parlaysis is not always familial (Case Study 1).
Examination
General examination
An initial brief general examination can yield important clues:
- an irregular pulse, suggesting a risk of embolism to the cerebral or spinal arteries
- stigmata, of malignancy or collagen vascular disease
- localised spinal tenderness to percussion, suggesting an epidural abscess or local osteomyelitis
- a tick hidden in the posterior neck hairline.
Neurological examination
Specific neurological examination is guided by hypotheses generated from the history with an emphasis on early examination of the legs (see below).
Head and neck
- Leg paraesthesia or weakness on neck flexion can point to cervical cord demyelination or canal stenosis (and spinal cord compression) as a cause of leg weakness.
- Weakness of the face is present in 50% of Guillain–Barré syndrome patients during the disease course and may be evident on presentation, so test carefully for facial muscle weakness (especially eye and lip closure power).
- Abnormal eye movement or evolving ophthalmoplegia may point to Guillain-Barré syndrome or a multifocal central nervous system process such as multiple sclerosis.
- Tongue movement and power may be weak in Guillain-Barré syndrome.
Trunk and upper limbs
- In examining the trunk, note whether superficial abdominal reflexes are present or absent, and test for abdominal muscle weakness on attempting to sit from lying in the supine position. A change to light touch or pinprick sensation may permit localisation to a thoracic spinal cord level.
- Are the arms completely normal? Signs of increased muscle tone, weakness, reflex or sensory abnormality can point to a cervical level or lead to suspicion of a more generalised neuropathy.
Lower limbs
- Are light touch, pinprick, position and vibration sensation abnormal? Include examination of the buttocks and perianal area as well as the trunk. If abnormal, is there a sensory level?
- Is there a pattern of weakness? There may be a proximal myopathy, with graded distal to proximal weakness, flexor more than extensor muscle weakness of an upper motor neuron disorder, the reduced reflexes of a polyneuropathy, or the fatiguable weakness of a neuromuscular junction disease. In a patient with variable weakness against resistance and normal reflexes, consider hysterical conversion disorder.
- Are there upper or lower motor neuron signs? (Table 2)
- Could spinal shock be present? (Box, Spinal shock).
Investigations
Imaging
Plain x-rays
Plain x-rays of the spine may help by showing a destructive bony lesion or severe degenerative spinal disease; however, generally, they have little part to play in the investigation of sudden leg weakness.
Computed tomography
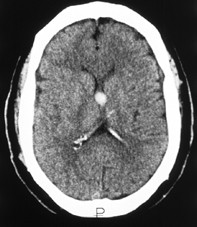
In practice, CT scans are easier to obtain than MRI scans when a patient presents with a suspected spinal cord lesion. Figure 1 shows a colloid cyst of the third ventricle, which can be associated with sudden bilateral leg weakness (Flowchart).
Magnetic resonance imaging
MRI has superior resolution to CT scans, and can display the spinal cord in both transverse and sagittal planes. MRI can also detect parenchymal spinal cord disease and extramedullary infection or haemorrhage. Figures 2a and b show demyelination of the thoracic spinal cord in transverse and sagittal section, respectively.
Neurophysiology
Nerve conduction studies
Nerve conduction studies may be required urgently to help confirm the diagnosis of Guillain-Barré syndrome – the usual findings are significant slowing of conduction velocity and conduction block.
Electromyography
EMG may aid in anatomical localisation of the pathology to the level of the nerve root, plexus, peripheral nerve, neuromuscular junction or muscle.
Lumbar puncture
Cerebrospinal fluid examination will be required if an acute spinal subarachnoid haemorrhage or infection is being considered as a possible diagnosis. It is desirable, but not necessary for the diagnosis of Guillain-Barré syndrome, and the characteristic rise in protein levels may not be seen early in the disease.
Common conditions
Drop attacks
A drop attack is a sudden fall without warning and without obvious loss of consciousness (Case Study 2). Injury may occur, but the subject can usually get up straight away.
Drop attacks have traditionally been ascribed to epilepsy, vertebrobasilar insufficiency, or midline cerebral lesions with acute intermittent hydrocephalus (such as a colloid cyst of the third ventricle as depicted in Figure 1). Other causes and associations of drop attacks include quadriceps weakness, presyncope, multiple sclerosis and whiplash. In clinical practice, most cases of drop attack occur in women who are otherwise normal (‘cryptogenic drop attacks’). In these cases, the cause is speculative and may relate in some way to different postural control mechanisms in men and women.
Guillain-Barré syndrome
Guillain-Barré syndrome is the most common form of acute polyneuropathy. Early diagnosis is important because of the potential for rapid deterioration and need for ventilatory support.
The initial symptoms in most patients are muscle weakness (up to 99%), paraesthesia (70%) and myalgia (30%). Weakness is noticed first in the legs (85%), arms (10%) or face (5%). The condition may be preceded by a bacterial or viral infection (Case Study 3).
The differential diagnosis of Guillain-Barré syndrome includes botulism, tick paralysis (in eastern Australia), severe acute hypokalaemia, meningeal carcinomatosis and acute transverse myelitis with ascending weakness and sensory disturbance.
Most cases of Guillain-Barré syndrome will benefit from intravenous immunoglobulin or plasma exchange. Supportive treatment includes admission to an intensive care unit if respiration is impaired and prevention of the complications of immobility. The prognosis is good, but up to 5 to 10% of patients still die, and 15 to 25% have persistent functional deficit.
Nontraumatic spinal cord compression
The clinical features of spinal cord compression vary, depending on the site of the compression and the speed of onset. In acute lesions, the loss of motor power is associated with reduced muscle tone, variable weakness and sensory loss. Bladder disturbance tends to occur later, except in acute cauda equina compression where it is an early feature. Spinal pain virtually always predates or accompanies the onset of neurological symptoms in spinal cord compression.
The two most common pathologies causing acute nontraumatic spinal cord compression are metastatic tumour and infection (epidural abscess). Their main differential diagnoses are transverse myelitis and spinal stroke. Other rare causes of acute cord compression include epidural and subdural haemorrhage.
When investigating possible acute spinal cord compression, imaging and treatment must be carried out urgently if neurological function is to be preserved. Spinal MRI is the definitive investigation of choice, giving morphological information about the site of compression and the presence of tumour or infection (Case Study 4). If MRI is not available, myelography combined with CT scanning provides similar information, although this carries a small risk of neurological deterioration. Remember, urgent investigation, diagnosis and decompression can preserve function.
Conclusion
‘Sudden’ weakness of the legs may develop over seconds, hours, days or weeks, and requires urgent attention.
A careful history will reveal the nature and duration of the symptoms, how they have affected the patient and whether or not there have been similar episodes previously.
A brief general physical examination – with an emphasis on early examination of the legs – can yield important diagnostic clues.
Rapidly evolving weakness of the legs, with unusual back pain and bladder involvement are indications for urgent referral. A delay in making the correct diagnosis could lead to serious consequences. MT