Common breast problems. A systematic approach to diagnosis and treatment

Women's health
A sound approach to diagnosing and treating breast problems can reduce anxiety for both patients and doctors. This involves careful history-taking, a thorough clinical examination, appropriate investigations and specialist referral if appropriate.
- Common breast-related presentations include breast pain, infections, lumps and nipple discharge.
- A sound approach to diagnosing and treating breast problems involves thorough history-taking, including a hormone and family cancer history, a comprehensive physical examination, appropriate imaging with or without tissue diagnosis and specialist referral if appropriate.
- Breast pain is rarely a symptom of cancer; it can be cyclical or noncyclical and a common cause is musculoskeletal.
- Breast infections require early treatment with appropriate antibiotics to avoid abscess formation.
- Benign breast lesions can be categorised within a spectrum of breast changes with some lesions requiring close follow up.
- Breast lumps should be worked up with triple test management.
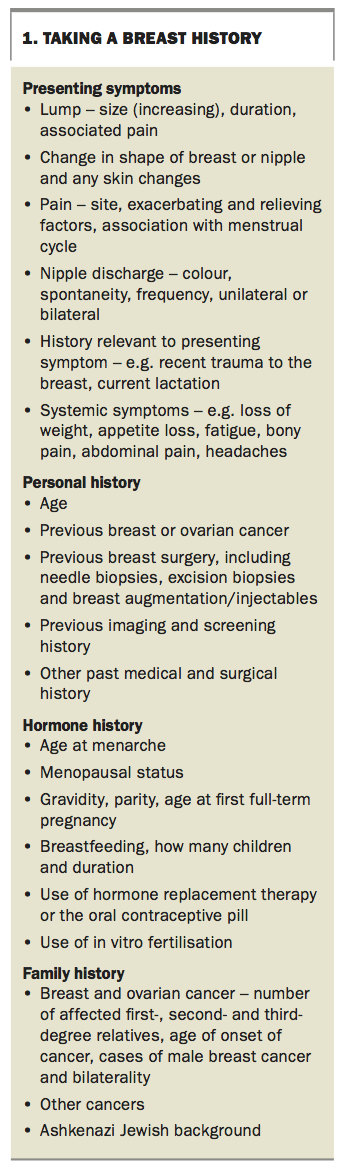
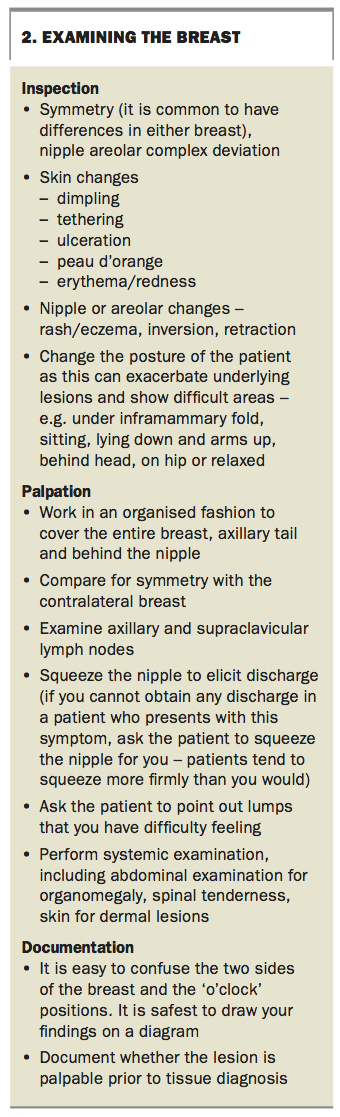
GPs often see patients with breast problems. Most of these patients are women and their complaints range from obviously benign conditions to more serious lesions requiring specialist referral and management. This article describes four common breast presentations – breast pain, infections, lumps and nipple issues. A sound approach to these breast problems is required, including thorough history-taking (Box 1), a comprehensive physical examination of the breast (Box 2), appropriate imaging and understanding when specialist referral is required.
{kind=link}
{kind=link}
Breast pain
Breast pain is one of the most common breast-related reasons for presentation. Patients often believe the cause is sinister. However, breast pain is rarely a symptom of cancer and can be self-limiting in nature. The vast majority of cases of breast pain represent normal physiological changes. Nevertheless, as a general rule, unless the cause of the pain is very clear, imaging should be performed to exclude an underlying breast lesion, especially if the pain is a new symptom.
True breast pain can be cyclical (varying over the menstrual cycle) or noncyclical. However, in many women who present with breast pain, the pain is actually chest wall related. Other nonbreast-related causes of apparent breast pain include cardiac, lung and gallbladder disease and shingles.
Cyclical mastalgia
Cyclical mastalgia refers to breast pain that occurs in relation to a woman’s menstrual cycle. It usually affects women in their 30s, although it can occur at any age during the premenopausal period. It tends to affect both breasts in a symmetrical distribution, and is usually worse just before menstruation and relieved with the onset of menstruation. The cause of cyclical mastalgia is not certain, but it may be related to overproduction of prolactin and oestrogen or underproduction of progesterone.
Cyclical mastalgia may spontaneously resolve without intervention in up to 20 to 30% of affected women.1 Lifestyle modifications can be of benefit including simple measures such as a supportive bra that is fitted by a professional bra-fitting specialist.2,3 Patients should be advised to avoid manual manipulation of the area to allow the area to settle, and topical NSAIDs can help in 70 to 92% of affected women.2
Some studies (albeit not high quality) suggest that reducing salt, caffeine and fatty foods (<15% of calories) in the diet, use of the herbal medicines phytoestrogens, Vitex agnus-castus (fruit extract) and chamomile extract, and reducing smoking may be useful in alleviating this pain.4 Vitamin B1, vitamin B6 (side effects may occur) and even vitamin E may also help, although the evidence is not conclusive. Bromocriptine has been studied but not proven to be effective and there may be side effects that require observation. Evening primrose oil may be helpful but has yet to be studied rigorously.3 It should be given at a dose of 1 g three times daily and, if there is a benefit after three months, it should be continued for a total of six months. It is wise to warn the patient that this dose may cause nausea.
If the pain is persistent and significant and affects quality of life, referral of the patient to a breast specialist is indicated. The specialist may prescribe drugs (e.g. tamoxifen and danazol), although these drugs are rarely used.
Noncyclical mastalgia
Noncyclical mastalgia is not as well characterised as cyclical mastalgia and has few associated factors. Some degree of noncyclical pain is present at puberty and during pregnancy, related to changes in hormone levels, but usually this pain occurs in older women. Other causes include periductal mastitis, diabetic mastopathy or use of medications such as digoxin, frusemide, spironolactone and antipsychotic medications. Cessation of these medications could be considered, and simple analgesia may be useful. Again modification of lifestyle factors as aforementioned may benefit. Acupuncture is currently being studied for this problem.5
Chest wall pain
Chest wall pain is one of the most common causes of perceived breast pain. It often arises from intercostal muscles, ligaments, ribs or even nerves. It often occurs in women with desk jobs who use a computer for long periods. The side of the pain is unrelated to the dominant arm.
A simple way to distinguish chest wall pain from true mastalgia is to roll the patient so the breast drops away from the site of the pain and to palpate the chest wall without the breast overlying it. Patients with chest wall pain will continue to have tenderness in that location but not in the actual breast tissue. It can be helpful to get the patient to look down at the position of your fingers during the examination to illustrate that the tenderness does not arise from their breast.
It is important to exclude other causes of chest wall pain, and importantly to reassure the patient. Treatments for chest wall pain include a well-fitting bra (it may help if this is worn when sleeping), simple analgesia, topical anti-inflammatories (to the chest wall rather than the breast tissue) and gentle stretching exercises (e.g. swimming). Referral of the patient to a physiotherapist may help facilitate posture advice or treat muscular causes of pain.
Breast infection
Breast infection can be lactational or nonlactational. Early treatment is essential to prevent tissue loss, and if the patient is systemically unwell, a referral to the hospital or breast specialist is recommended.
Lactational infection
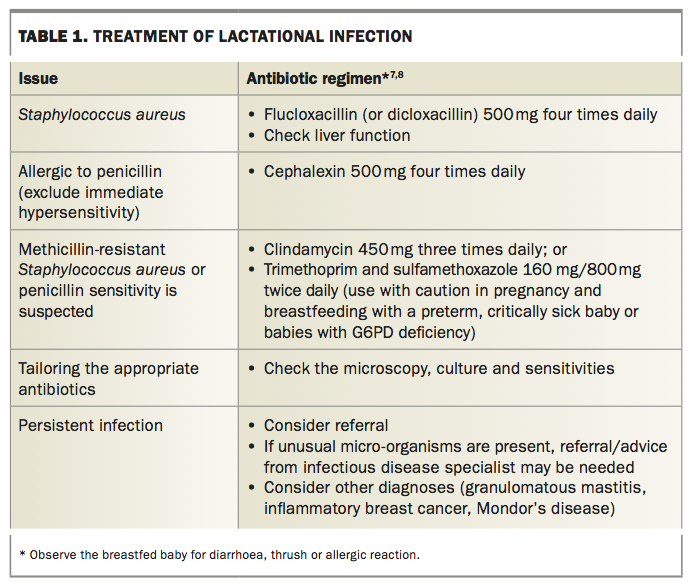
Infection during lactation is most common in the first six weeks of breastfeeding, usually as a result of Staphylococcus aureus entering a cracked nipple or skin abrasion.6 Effective and early antibiotic use is recommended to prevent progressive infection or abscess formation (Table 1).7,8 Women who wish to continue breastfeeding should be encouraged to continue feeding from the affected breast or to express from that breast. Efficient and frequent milk removal has been shown to prevent progressive infection and involving a lactation consultant is useful in treatment.9
{kind=link}
Women who are lactating often have dense breast tissue that makes mammograms difficult to interpret. In these women, ultrasound imaging is therefore the preferred method and should be performed to exclude abscess formation. Lactational abscesses can often be treated by repeated percutaneous aspiration under ultrasound guidance. The patient may continue to feed from the treated breast after aspiration. If the infection does not improve or there are large amounts of fluid (>50 mL) aspirated each time, referral is indicated.
Open drainage is usually not required unless the abscess is very superficial with a potential for skin or tissue loss (Figure 1), in which case the patient should be referred to a specialist. A small incision under local anaesthesia may be an option for the GP if the area does not involve deep tissue and is localised with minimal induration from cellulitis. The abscess contents should be sent for microscopy and culture to ensure the antibiotic treatment is appropriate. Culturing breast milk can be misleading and often contaminated, therefore, when possible, culturing the source is more useful.7,9 If there is a lack of improvement after early commencement of antibiotics, it is important to refer the patient while considering other diagnoses, including inflammatory breast cancer, Mondor’s disease and granulomatous mastitis.
{kind=link}
After the acute infection has settled, a repeat ultrasound examination in three months is advisable to check whether any mass remains. Tissue sampling before the infection has settled can lead to spurious results.
Nonlactational infection
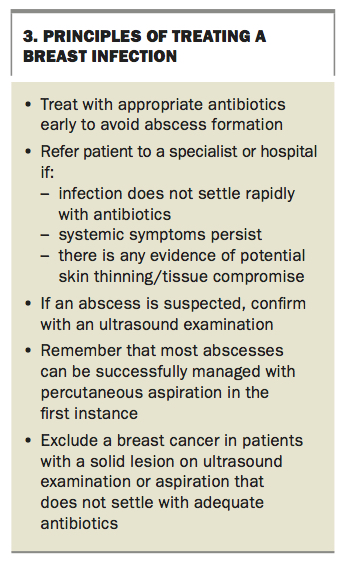
Nonlactational infection can occur as a spontaneous event or after trauma/intervention. Nonlactational breast infection is classified by the area of the breast affected – central, peripheral or skin-associated. The principles of treating a breast infection are outlined in Box 3.
{kind=link}
Central breast infection
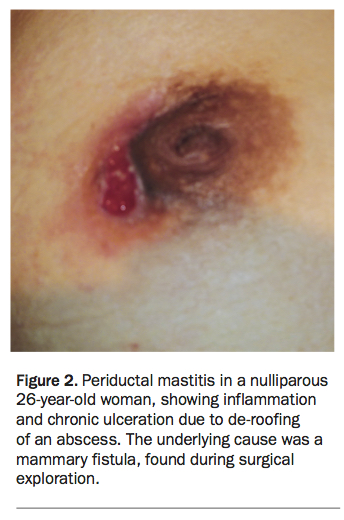
Central infection occurs as a result of periductal inflammation in the areolar region of the nipple and is sometimes called periductal mastitis. It often presents as an abscess in this area (Figure 2). On clinical examination, ensure there is no nipple discharge associated with palpation of this region, which might indicate a mammary duct fistula. It is thought that duct ectasia (dilation of the subareolar breast ducts) predisposes to this type of infection. Smoking has also been shown to be an important factor, and recurrent infection is common in smokers.10
{kind=link}
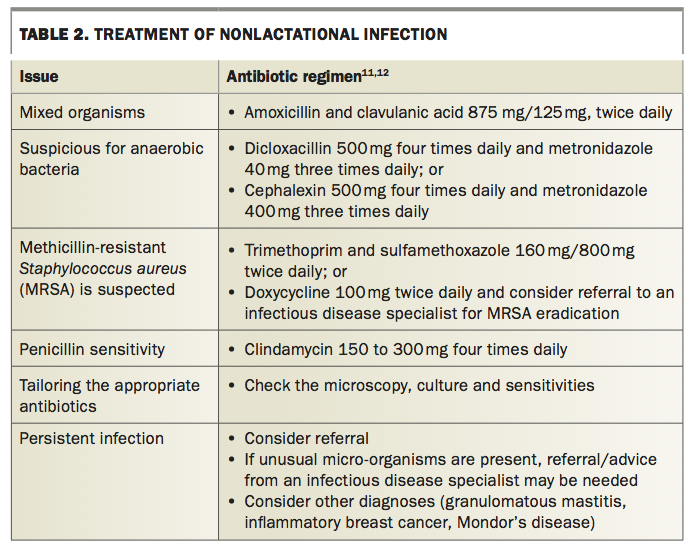
An ultrasound examination should be performed to exclude an abscess or other mass. As the infecting organisms in this type of infection are usually mixed, cover against Gram-negative and anaerobic bacteria is needed; amoxicillin and clavulanic acid is usually sufficient, however, other regimens are also useful (Table 2).11,12 Smoking cessation is essential. Abscesses in this area should be managed with aspiration or surgically as for lactational infection, with any aspirate sent for microscopy. If the patient is systemically unwell, or there is no improvement, referral of the patient for consideration of hospital management is advised. If a mammary fistula is present, the patient should be referred to a specialist, as surgery may be needed. Occasionally the only way to manage chronic periductal infection is with duct excision.
{kind=link}
Peripheral breast infection
Peripheral breast infection is not as common as central breast infection. It may be associated with underlying illnesses such as diabetes, corticosteroid treatment and granulomatous mastitis (a condition affecting young parous women, with multiple peripheral breast abscesses). Treatment principles are the same as for other breast infections – give appropriate antibiotics and treat abscesses with aspiration or incision/drainage, with repeat imaging showing improvement. After the infection resolves, exclude underlying malignancy (you may want to liaise with the breast specialist). For persistent or recurrent breast infections, specialist referral may be required.
Skin-associated breast infection
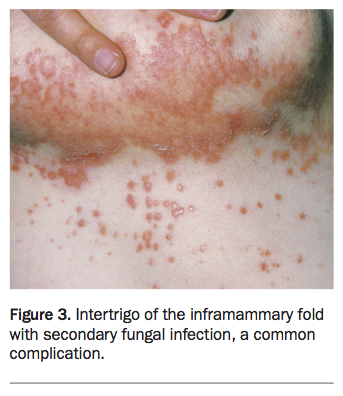
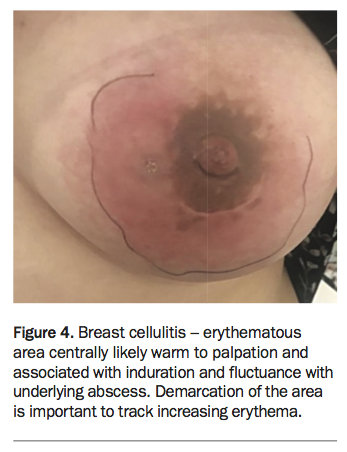
Infection of the skin of the breast is very common. It tends to occur in women with large breasts and usually affects the lower half of the breast. A common presentation is infection as a result of excoriation of the inframammary skin fold, leading to intertrigo or fungal infection – a problem exacerbated by hot weather and sweating (Figure 3). This can provide a portal for entry of bacteria, usually S. aureus. Other predisposing factors include recent surgery, radiotherapy and pre-existing lesions, such as a sebaceous cyst or hidradenitis suppurativa (Figure 4).
{kind=link}
{kind=link}
Treat as for any cellulitis or abscess, with appropriate antibiotics and drainage of purulent exudate. For patients with recurring inframammary skin fold problems, a simple tip is to wear a cotton handkerchief or garment (even a cotton breast pad) between the skin and the bra, to absorb excess moisture. Good hygiene and keeping the underside of the breast dry after washing are also important; using a hairdryer on a cool setting after patting the area dry is the best way to achieve complete dryness of this difficult area. Antifungals and emollients are often unnecessary if the patient complies with this regimen.
Postintervention infections, after a breast biopsy or surgery, is a mode of direct skin breach and is an entry site for bacteria. Postoperative infections can occur in the acute phase (less than one month from surgery) or be delayed (more than one month) and often present in the context of radiotherapy or chemotherapy. With these infections it is important to elicit whether a prosthesis is present as this requires immediate referral to the specialist or hospital unit to prevent the loss of the implant. Early direct discussion with the operating surgeon regarding management can result in better outcomes for the patient.
Nipple piercings can also be a source for infection, especially piercings that interrupt the nipple duct tissue. If infection occurs, it is advised that the woman remove her nipple piercing until the infection has completely settled and advised that recurrence may be a risk if the piercing is reinserted in the same position.
Breast lumps
Common causes of a palpable breast lump include prominent fibroglandular tissue (normal breast tissue), a cyst, fibroadenoma, abscess, lipoma, fat necrosis, haematoma and breast cancer. Any lesion that is increasing in size requires a specialist review and use of available guides is helpful for determining a management plan.13
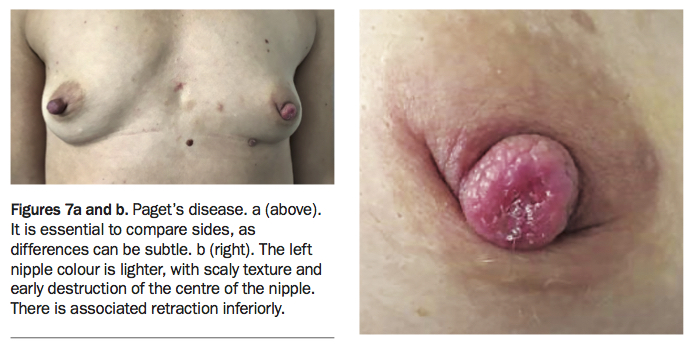
Benign breast lesions are categorised as nonproliferative, proliferative with no atypia and proliferative with atypia (Table 3).14,15 Lesions diagnosed as atypical lobular hyperplasia, atypical ductal hyperplasia and lobular carcinoma in situ are all marker lesions and confer an increased risk of developing a cancer.15 They require close surveillance that can often be directed by the referred specialist.
{kind=link}
Breast cancer affects one in eight women and can present at any age. It usually presents as a firm unilateral, nontender lesion in the breast. There may be skin or nipple changes associated with the lesion. All lesions require specialist management, which is usually multidisciplinary. With the advent of screening, we have been able to diagnose patients before the lesion is palpable. Most breast cancers (about 80%) will be invasive ductal breast cancer, 10% will be invasive lobular carcinoma and about 10% will be inherited.16,17 Ductal carcinoma in situ is a preinvasive lesion that requires formal excision and treatment. Rarely, a breast lump might be a metastasis from a different type of cancer.
The management of breast cancer depends on the circumstance and can include local treatment including surgery with or without radiotherapy and/or systemic therapies such as hormone therapy or immunotherapy/chemotherapy.
Women with breast lumps require careful assessment in the clinic to determine the forward management. In patients presenting with a breast lump, the role of the GP is to:
- determine whether there is a true mass
- ascertain the patient’s risk factors for breast cancer
- organise the appropriate imaging, including mammography and ultrasound
- obtain a tissue diagnosis with radiology-guided core biopsy for solid lesions or fine needle aspiration with or without cytology for simple symptomatic cysts, if necessary
- refer patients to a breast surgery specialist to determine the management of suspicious lesions.
GPs should use the triple test approach to diagnosis, which involves three components:
If any component of the triple test is indeterminate, suspicious or malignant, the test is positive and requires specialist referral.13,18
Breast imaging
Breast imaging is a crucial component of the triple test. It is essential to order the correct investigation(s) and to communicate effectively with the radiologist to ensure the correct diagnosis is made in a timely fashion.
Mammography and ultrasound examination are the most frequently used modalities for imaging breast lumps. In women over 40 years of age, mammography is the primary modality used but all women presenting with a palpable lump should also have an ultrasound examination. Ultrasound is acceptable as the investigation of first choice for women under 35 years of age and may be used as the only imaging modality for young women and those who are lactating, but is often used as an adjunct to mammography.4,19
When requesting imaging, it is useful to draw a diagram showing the location of the lump of concern. If the patient will undergo the imaging investigation on the same day as your clinical examination, another useful tip is to draw the location of the lump on her skin, with her arm behind her head – the standard position used by most breast sonographers. This is especially helpful for lumps that are difficult to feel or located in generally nodular areas of the breast.
Locally advanced cancers are defined as more than 5 cm, involving skin or chest wall or have axillary nodal disease. Inflammatory breast cancer is an important subclass and presents with persistent erythema and skin oedema with the appearance of peau d’orange (orange peel), a history of less than six months and occupying at least one-third of the breast.20 This can sometimes be confused with breast infection – it is vitally important to be wary of the breast infection that persists despite antibiotic treatment. It is important to examine the breast for lesion mobility from the chest wall and skin, and also examine the lymph node basins in the axilla and supraclavicular fossa. Imaging and sampling may be required of the axilla. History and examination need to be extended to determine any symptoms of distant disease. Formal systemic staging is required if there is locally advanced disease or if distant disease is suspected. Standard staging for breast cancer includes a CT chest, abdomen, pelvis and whole body bone scan.
Women from the age of 40 years are able to participate in BreastScreen Australia, a national breast cancer screening program, free of charge for asymptomatic women. Women over the age of 50 years are recalled every two years. Women who have previously been diagnosed with breast cancer are able to rejoin the BreastScreen program for annual screening.
MRI is useful in certain circumstances. Women under 50 years of age with a strong family history or inherited gene mutation may be eligible for MRI screening.21 Women who fit these criteria may require genetics review or referral to a familial cancer clinic. To refer a patient for an MRI, a specialist review is required to determine whether the woman’s risk is consistent with being eligible for a Medicare rebate. MRI can also be used in the context of breast cancer assessment and planning or a persistent breast lump that cannot be seen on mammogram or ultrasound (although this is not a rebatable investigation). If a persistent lump is present, despite normal imaging, a specialist review is required and a clinical biopsy may need to be performed.
Nonexcision biopsy
There is often confusion about which biopsy technique to use – fine needle aspiration cytology (FNAC) or core biopsy – to investigate a breast lesion.
The benefits of FNAC include a shorter procedure, quick results (possibly even on the same day) and a decreased risk of haematoma. FNAC is suitable for small lesions if there is concern that a core biopsy may remove too much tissue for the lesion to be located later, but these lumps are usually impalpable. The difficulty with FNAC is that it yields indeterminate or insufficient results more often than a core biopsy, and the patient may therefore require a further procedure.
Core biopsy, on the other hand, requires local anaesthesia, results take longer to obtain and it causes more discomfort and postprocedure complications. However, unlike FNAC, core biopsy frequently enables characterisation of the lesion, for example, invasive cancer to be distinguished from ductal carcinoma in situ, and it has a higher sensitivity and specificity. The core biopsy can also be the basis for upfront treatment decisions as the tissue can be tested upfront for receptors to plan therapy and allows for an informed discussion regarding the potential prognosis for the patient. If there is uncertainty about which investigation would be best, contact or refer the patient to a breast specialist.22
It is wise to thoroughly document your physical assessment findings before biopsy, as a haematoma may alter the breast examination afterwards. A breast surgeon attempting to remove a perceived palpable lesion may discover it has resolved by the time of surgery, and localisation techniques may need to be arranged.
For a nonpalpable lesion or very small lesions, a localisation clip should be considered for deployment at the time of biopsy and usually the radiologist can advise the need for this. Some lesions are only visible using one mode of imaging. When possible, ultrasound-guided clip insertion is preferred; however, when sonographically the lesion is occult, a stereoguided clip insertion is required. The clip allows the lesion to be localised for surgery. Another situation where the clip insertion may be required is to determine the site of a large or locally advanced lesion before upfront chemotherapy in case of complete response to treatment. It is useful to discuss the individual case with your preferred specialist for impalpable lesions as it can alter the management plan significantly.
If the results of breast imaging and biopsy are normal but there is a persistent worrying lump or change in the breast, do not hesitate to refer the patient to a specialist, as some cancers can present with negative tests.
Nipple problems
There is a wide range of nipple changes that are within normal range. It is essential to be able to distinguish between the normal spectrum of breast development and benign nipple changes from more sinister changes including nipple retraction and Paget’s disease.23
Nipple inversion and retraction
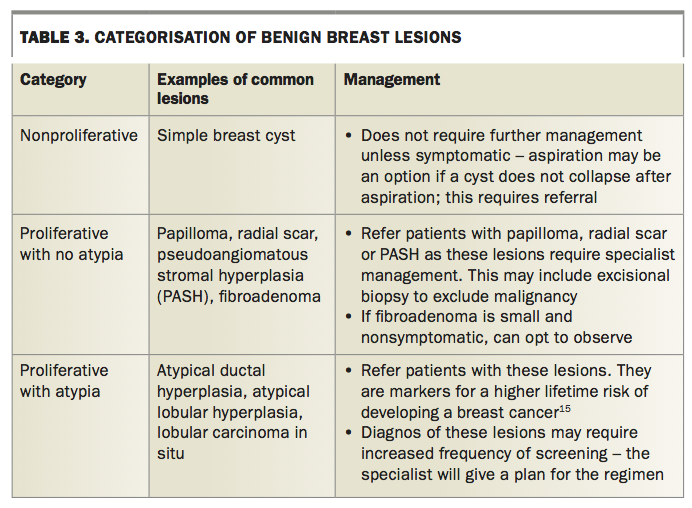
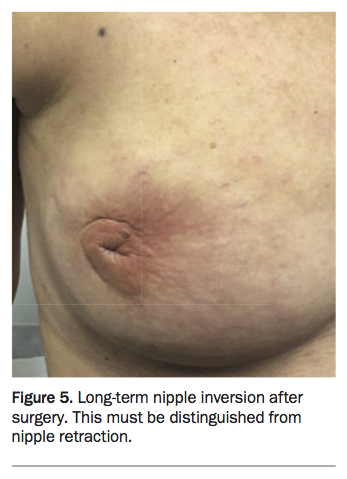
Nipple inversion occurs in 15 to 20% of women and presents as a slit-like invagination of the nipple. The most common cause of nipple inversion is duct ectasia. Other causes of nipple inversion can include breastfeeding, trauma resulting in fat necrosis or surgery, ptosis, breast cancer or breast infections. Nipple inversion (Figure 5) must be distinguished from nipple retraction (Figure 6), a sign that may be related to an underlying malignant lesion. If there is nipple retraction present, imaging with mammogram and ultrasound is required to rule out underlying malignancy.13
{kind=link}
{kind=link}
Nipple excoriation
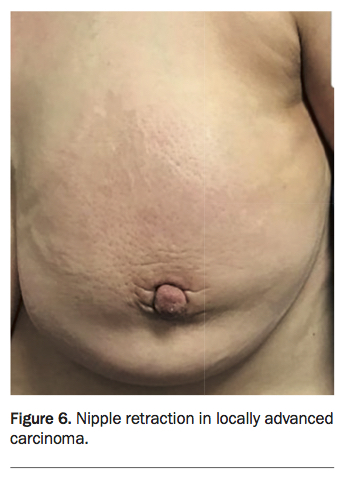
Nipple excoriation can be traumatic in nature or skin related including eczema/dermatitis or fungal infections. It can present with scaly, itchy nipples and differentiation from Paget’s disease is essential (Figure 7). Eczema usually involves the areola first, whereas Paget’s disease always involves the nipple itself, including destruction of the nipple. If the symptoms are unilateral, persistent and progressive, further investigations should be performed including a mammogram, ultrasound and a punch biopsy. The presence of Paget’s disease is often associated with ductal carcinoma in situ or invasive breast cancer (82 to 94%).22,24
{kind=link}
Nipple lesions
The nipple areolar complex is composed of sebaceous and modified sebaceous glands (Montgomery tubercles), apocrine glands and hair follicles. Any of these skin appendages may result in blockage and subsequent lesions can form (e.g. sebaceous cyst).
Fibroepithelial growths can also occur, and a simple excision can take place without disruption to the nipple complex. Nipple adenomas are benign papillomatous growths of the lactiferous ducts, and can present with nipple nodules, erosion, nipple discharge and ulcerations, and can mimic Paget’s disease. This area is difficult to image, and referral may be required. It is also important to remember that skin cancers can also affect the nipple.
Nipple discharge
Twenty per cent of women have a physiological discharge that can be elicited by squeezing the nipple. Discharge can vary in colour from yellow to green to black. Galactorrhoea causes a bilateral milky discharge, and a careful drug history should be taken (especially for psychotropic agents) and prolactin levels checked – true galactorrhoea is a rare condition. Key points in taking a history for a nipple discharge are listed in Box 4.
{kind=link}
Significant nipple discharge that requires further investigation includes spontaneous, single duct, unilateral, bloody or haemoserous in character. A simple test in the clinic is to use a urinalysis stick to test the discharge for blood. Mammography and ultrasound examination should be performed to exclude a mass lesion such as a papilloma. Even if imaging does not find anything suspicious, patients with this type of discharge should be referred to a specialist as duct excision may be required. Patients who have persistent multiduct discharge that appears physiological should also be referred if their symptoms are distressing enough to warrant surgery.
Women presenting with a physiological discharge should also undergo routine imaging to exclude pathology. If no abnormality is found, they should avoid manual manipulation of the nipple for three months and then return for follow up to check whether the discharge has settled.13
Conclusion
A systematic approach is required to diagnose and treat common breast problems. Conveying confidence, listening carefully to the patient’s concerns and giving measured reassurance will reduce patient anxiety. If any features of concern are noted, prompt referral of the patient to a breast specialist is indicated. MT