Type 1 diabetes – towards a national childhood screening program

Ten new cases of type 1 diabetes are diagnosed every day in Australia, three of which are diagnosed too late, resulting in traumatic diabetic ketoacidosis requiring intensive care. However, formal recognition of two early presymptomatic stages allows for early identification and an opportunity to prevent, or at least delay type 1 diabetes. Launching in early 2022, a new pilot study will assess the feasibility, acceptability and cost-effectiveness of a routine national screening program for type 1 diabetes in children.
Type 1 diabetes results from immune-mediated destruction of insulin-producing pancreatic beta cells. Over 125,000 Australians have type 1 diabetes, with over 3,700 diagnosed in 2020 (10 new cases per day).1 It is frequently diagnosed in children and young adults, with the peak incidence between 10 and 14 years of age.2 Management is complex and burdensome, both for the individual and their family, requiring lifelong insulin therapy to maintain blood glucose levels within the narrow limits of normoglycaemia and to avoid acute, hypo- and hyperglycaemia. Suboptimal glycaemic control is closely associated with serious acute and chronic diabetes complications, such as severe hypoglycaemia, recurrent diabetic ketoacidosis (DKA), diabetic eye disease (retinopathy, macular oedema, blindness), nephropathy/chronic kidney disease, neuropathy (which can lead to amputation), reduced lifespan and significant psychological morbidity.
Diagnosis of type 1 diabetes is often delayed and traumatic
Three in every 10 Australian children with type 1 diabetes are diagnosed too late, presenting to emergency departments with DKA, a life-threatening condition that, if left untreated, can cause coma and death.3 These numbers are even more alarming in regional Australia, with up to 80% of young people with type 1 diabetes initially presenting with DKA.4 Treatment of DKA requires admission to intensive care, necessitating expensive high-level medical care and causing significant post-traumatic stress for families.5
Diagnosis is often delayed, as the warning signs and symptoms of type 1 diabetes are vague and often missed by families and healthcare professionals. Collectively known as the 4 Ts, symptoms include increased thirst, frequent urination (toilet), excessive tiredness and weight loss (thin). Almost all children present with at least two of these key symptoms and over half have symptoms for over three weeks, but they are frequently missed or easily attributed to other causes or behaviours.6 Even when families do seek medical care, GPs also find it difficult to recognise the symptoms of type 1 diabetes, with almost a quarter of families having multiple healthcare contacts in the weeks before diagnosis.7-9 Public awareness campaigns to increase awareness of the signs and symptoms of type 1 diabetes have had minimal impact or resulted in short-term awareness but lacked sustained outcomes.10,11
DKA at diagnosis has lifelong implications
Australian children presenting with DKA at diagnosis are more likely than those without DKA at diagnosis to be readmitted to hospital with DKA.3 Furthermore, DKA at diagnosis impacts long-term glycaemic control, with glycated haemoglobin (HbA1c) levels consistently higher for children with severe and mild/moderate DKA (1.4% and 0.9% higher, respectively) compared with those without DKA, independent of demographic or socioeconomic factors.12 HbA1c levels in childhood are a predictor of glycaemic control in adulthood and suboptimal metabolic control increases the risk of serious diabetes-related complications.13,14 There is also evidence that DKA at diagnosis of diabetes negatively affects cognitive function.15,16 Given these lifelong health consequences, this traumatic start to disease has serious and long-lasting implications.
Recognising presymptomatic type 1 diabetes
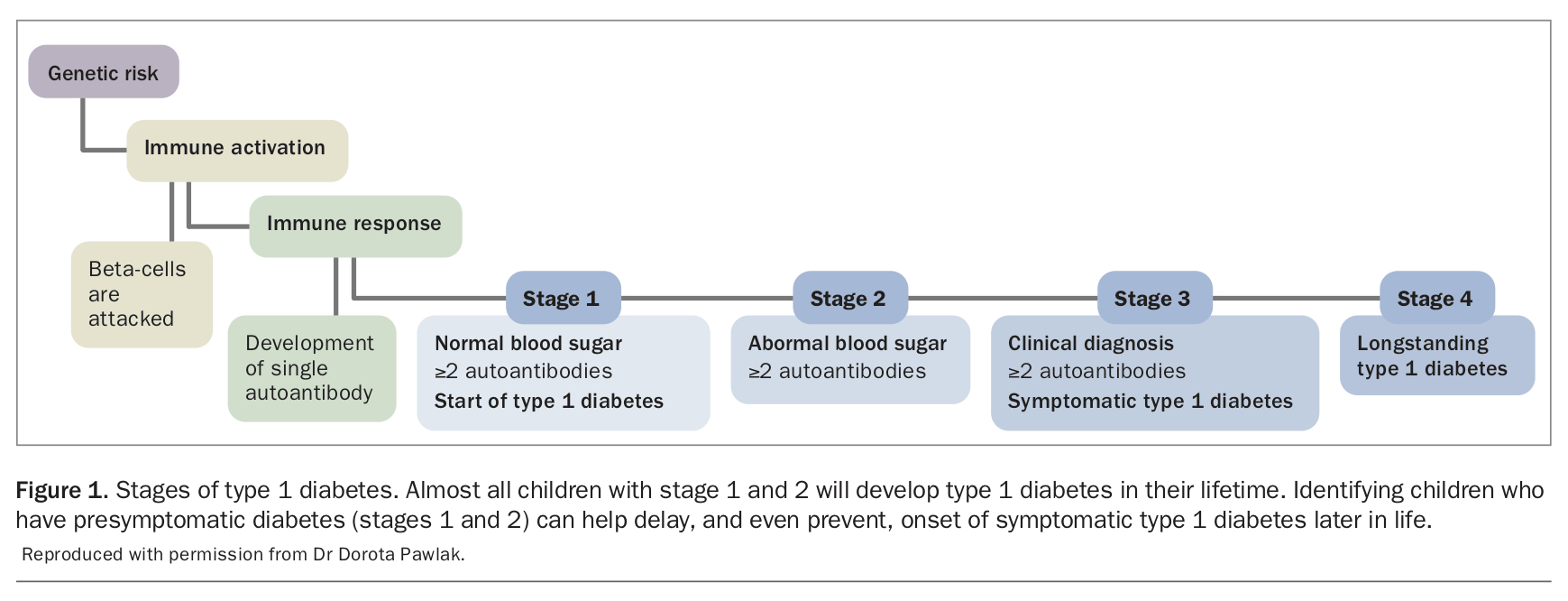
A new staging classification system identifies two early presymptomatic stages of type 1 diabetes (stages 1 and 2), which now mark its onset rather than the traditional late symptomatic clinical diagnosis (stage 3) (Figure 1). These two early stages are characterised by the appearance of persistent circulating islet autoantibodies (IAA, GAD, IA-2 and ZnT8), which are readily detected in serum in standard clinical tests. During stage 1, blood glucose levels remain normal, whereas in stage 2, blood glucose levels are elevated (a similar range to that seen with impaired fasting glucose or impaired glucose tolerance in prediabetes) but do not meet the diagnostic criteria for diabetes. Stage 1 may begin in early life, with birth cohort studies demonstrating that the peak time for appearance of islet autoantibodies is between the ages of nine months and 2 years.17 A diagnosis of stage 1 or 2 type 1 diabetes is a precursor to stage 3 symptomatic disease, with most children developing type 1 diabetes by adulthood.18 Around 70% of children with stage 1 diabetes progress to stage 3 clinical type 1 diabetes within 10 years and 75% of children with stage 2 diabetes progress within five years.18 Both stages 1 and 2 can be present for months or years before clinical diagnosis, and represent a valuable opportunity to intervene in the autoimmune process and prevent, or at least delay, beta-cell loss.
{kind=link}
General population screening is needed to identify children early and improve outcomes
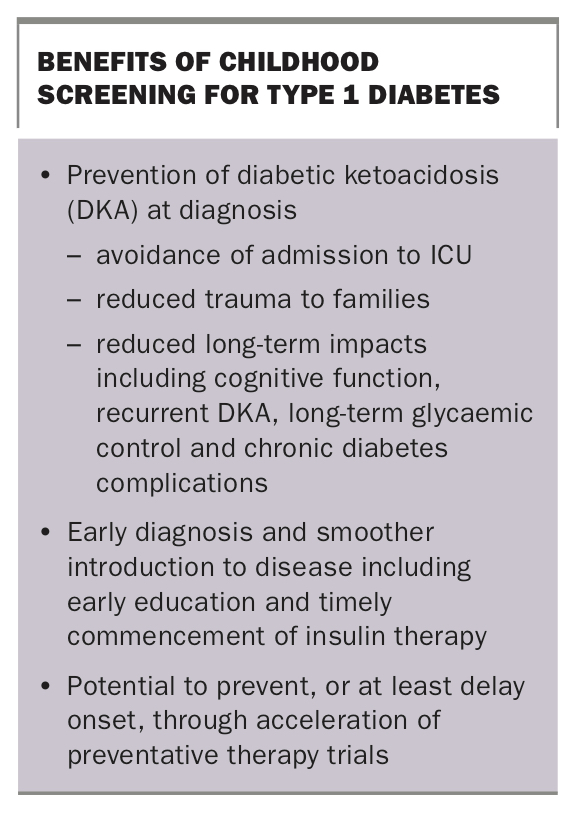
Screening for presymptomatic (stages 1 and 2) type 1 diabetes provides the opportunity for early diagnosis and prevention of DKA and its sequelae (Box). Screening of first-degree relatives (sharing around 50% of their genes) in clinical trials has been underway for 20 years in Australia; however, 90% of those who develop type 1 diabetes have no family history of the condition.19 Therefore, screening young children in the general population is the only way to identify most children in the presymptomatic stage and allow for timely treatment to prevent DKA, reduce trauma to the family at diagnosis, improve long-term health outcomes and, potentially, preserve beta-cell reserves. Given the lifelong impacts of DKA at diagnosis on long-term glycaemic control, cognitive function and risk of recurrent DKA and long-term complications, early diagnosis through screening can deliver enduring health benefits beyond diagnosis.3,13-16 International screening and follow-up programs have reduced the rates of DKA at diagnosis to less than 5%.20 This has the potential to translate into cost savings for health systems through reduced ICU admissions and the protective effect on long-term glycaemic control. Screening also offers the potential to accelerate preventative therapies by identifying potential presymptomatic participants for clinical trials.21
{kind=link}
Screening in Australia – an implementation pilot study
The first step towards implementing a routine screening program in Australia is to identify the most appropriate screening model. International long-term trials have already demonstrated the clinical efficacy of screening for type 1 diabetes.20 However, it is not clear how screening should best be conducted, particularly within different local contexts. Trials have explored different models of screening (principally either genetic screening with islet autoantibody follow up or islet autoantibody-only screening), with advantages and limitations to each. For example, genetic screening has the advantage of being a one-off population-wide test (with follow up of just the subset of children with a higher genetic risk), whereas autoantibody screening requires population-wide rescreening (similar to the rescreening approach for bowel, breast and cervical cancers) because of the unpredictability in the timing of the appearance of autoantibodies. However, autoantibody screening will identify fewer false positive results as it screens for the presence of presymptomatic disease rather than a risk of disease.
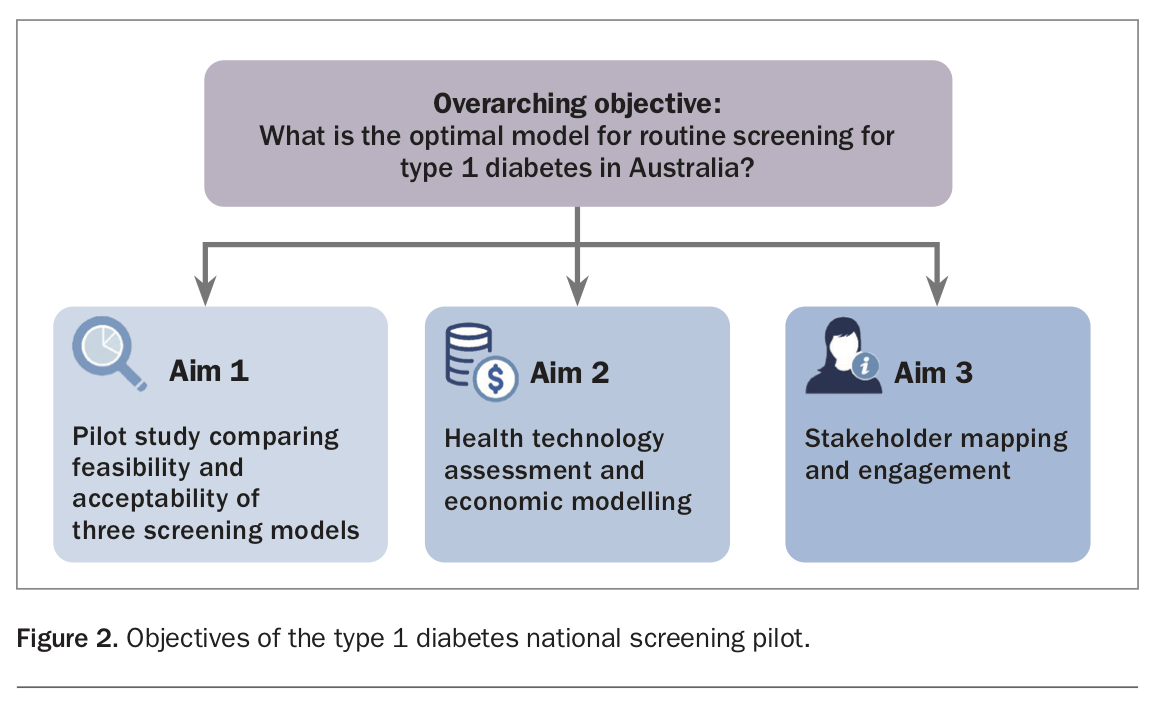
This Australian pilot clinical research program, funded by JDRF Australia, is therefore seeking to compare the feasibility, acceptability and cost-effectiveness of three screening models for type 1 diabetes in infants and children across Australia (Figure 2). Launching in early 2022, localised catchment areas across Australia will pilot one of three screening models. Each model is designed to feature at-home saliva or dried bloodspot testing as part of a future-focused program that is readily scalable to a population-wide roll-out aligned with existing infrastructure and workflows and provides equitable access for all children in Australia. The goal is to invite every eligible child in each catchment area to participate in screening to assess the feasibility and acceptability of screening to families and health professionals.
{kind=link}
As illustrated in Figure 2, this implementation pilot will be supported by: a health technology assessment and modelled economic evaluation to formally review the international evidence base and model the cost-effectiveness of a screening program in Australia using local costs and incidence rates with pilot uptake rates and international clinical efficacy data; and a broader stakeholder mapping and communication plan to better understand the wider perspectives on screening across health, industry, government and diverse community groups including Aboriginal and Torres Strait Islander people, culturally and linguistically diverse communities and those in regional and remote areas.
This pilot is the first crucial step towards a national, routine screening program to improve the health outcomes for Australian children across the country.
Conclusion
Symptoms of type 1 diabetes in childhood are often missed by parents and healthcare professionals. Late diagnosis can result in DKA, a life-threatening condition that is associated with poor long-term glycaemic control and other lifelong comorbidities. Early diagnosis through screening can alleviate the risk of DKA and thereby improve immediate and long-term impacts. An Australian pilot clinical research program investigating the implementation of a national childhood screening program will be launched in early 2022. MT