Recognition and management of depression in men

Dr Seidler is a Clinical Psychologist and Research Fellow at Orygen in the Centre for Youth Mental Health, University of Melbourne; and Director of Mental Health Training at Movember.
Associate Professor Rice is a Clinical Psychologist and Principal Research Fellow at Orygen in the Centre for Youth Mental Health, University of Melbourne, Melbourne, Vic.
Depression
Men's health

Although men have apparently lower rates of depression than women, their high rates of suicide, substance misuse and physical violence point to an undercurrent of distress. GPs can help their male patients with depression by recognising externalising symptoms such as anger, substance misuse and risk-taking, leveraging men's strengths, broadening their mental health literacy and building a collaborative therapeutic relationship.
- Although prevalence rates indicate men are less likely than women to experience depression, the difficulty of reaching, recognising and retaining men with depression in treatment may explain much of this difference.
- Given men may experience and express depression through externalising symptoms (e.g. anger, substance use, risk-taking), detecting, discussing and normalising these manifestations of distress may be useful.
- Building collaborative, trusting and transparent doctor-patient relationships may help men to understand and communicate their mental health difficulties.
- Clarifying and demystifying mental health treatment pathways and men’s expectations may further catalyse recovery from depression.
Depression is the most common mental disorder and a leading cause of disability worldwide.1 In Australia, major depressive disorder is reported to affect about one in eight men across their lifetimes, compared with about one in six women.2 Although these statistics suggest men have greater resilience against depression than women, the vast majority of suicide deaths in Australia are in men (76%), and men have high rates of substance misuse and physical violence.3,4 This suggests an undercurrent of distress requiring intervention in men.
In the common narrative, the discrepancy between men’s reported depression rates and negative outcomes is due to men not seeking help. However, no single factor appears responsible; rather, a complex interplay of factors related to men’s help-seeking pathways is implicated.5 Importantly, many of these factors are ripe for targeted intervention by GPs.
This article discusses barriers to care for men with depression and how to overcome them. It presents resources and tips to help GPs identify and manage male patients with depression, including improving their mental health literacy and building a collaborative therapeutic relationship with men with depression or suicidality.
Men's help-seeking
If we are to intervene effectively in men’s depression, we must first be able to detect it. Even when men manage to overcome barriers to care, there is often a lengthy delay in their help-seeking.6 Some adopt a ‘wait and see’ approach and reach out only when their symptoms are severe, risk is high and crisis intervention becomes necessary.7 The ramifications of undetected and untreated depression among men are long term. Increasing hopelessness and withdrawal negatively impact on work productivity and attendance, social functioning and family wellbeing.8
The role of masculinity
The experience of depression fundamentally contradicts many core elements of ‘traditional’ masculinity.7,9 Some men view and interpret depressive symptoms as signs of personal weakness and failure, and as in direct opposition to socialised attitudes that men should remain stoic, invulnerable and emotionally restricted.10 As a result, the act of seeking help for depression presents internal conflicts for many men, where admitting to their experience of psychological distress is akin to relinquishing control, self-reliance and independence.11 By contrast, refusal, avoidance or denial of the need for treatment is often aligned with a perceived strength of masculine character.7
Leveraging men’s strengths
The reframing of mental health help-seeking as a courageous and honourable act is often needed to improve men’s willingness to access services.12-14 Men themselves often describe the act of redefining strength by figuratively ‘fighting’ their depression and drawing on a sense of personal responsibility to reshape their help-seeking narrative.7,15,16 As such, the masculine traits that in one context can be harmful to men can be used to their advantage through tailored intervention.12,17 Some support groups that ‘go to where men are’, building on male-oriented activities and language, are listed in Box 1.
{kind=link}
Mental health literacy
If we want to help men accept that depression is an issue worthy of intervention, it is essential to build up their ability to understand, recognise and communicate their mental health problems, known as mental health literacy.18 Men are reliably found to have poorer overall health literacy than women, with a lack of practice and feelings of fear or mistrust, stigma and shame all potentially playing a role.19,20 This manifests in some men presenting with nonspecific symptoms and brief, indirect descriptions of their internalised experience.
Importantly, gender differences in mental health literacy are not due to an emotional deficiency in men. Rather, mental health literacy requires time and effort to cultivate in a safe and trusted space.21,22 Global movements such as Movember aim to bring mental health conversations into men’s lives and show how and why having these conversations with friends and family can be life-saving.23
Some strategies to encourage your male patients to think differently about their mental health are shown in Box 2. Resources to suggest to your male patients to improve their mental health literacy and understanding and communicating about their mental health are listed in Box 3.
{kind=link}
{kind=link}
Setting expectations
As more men present to their GP seeking mental health advice or specialist referral for ongoing treatment, there is potential that they will not be fully engaged by care from a mental health practitioner. Our recent study of 1907 Australian men who sought mental health help found that 45% dropped out of treatment prematurely without communicating with their clinician, and 27% of these men accessed therapy once and did not return.24 Importantly, therapy dropout typically occurs after the first or second session of psychological treatment. An unsatisfying experience can have detrimental ramifications for future disclosure of distress, as the patient may lose trust in the health system and see this outcome as confirming their own prognostic pessimism or ingrained doubt in help-seeking.25,26
For GPs, setting expectations so that your male patient enters treatment prepared is key. Never overestimate men’s knowledge of the mental health system, which is foreign and uncomfortable for many. The basics to cover include:
- cost (e.g. how the Medicare rebate works)
- duration (e.g. psychological treatment can vary significantly in length depending on the presenting problem and severity)
- the mechanics of therapy and treatment options (e.g. the difference between cognitive behavioural therapy [CBT] and acceptance and commitment therapy [ACT])
- questions they can and should ask their therapist (e.g. how will I know if I am making progress?).
Follow up
Finding opportunities to check in with patients early in the treatment process, and reassuring them of their options if the chosen therapist does not meet their expectations, may help prevent negative outcomes. If a male patient navigates all the barriers to seeing their GP, from initially disclosing their distress to gaining a referral and attending a session with a therapist, this effort and openness for change should be leveraged for therapeutic advantage.
The importance of the GP-patient relationship
GPs are often termed ‘gatekeepers’ when it comes to men’s mental health: the initial and often instrumental point of contact where men might disclose their concerns for the first time. A recent study of over 2000 help-seeking men showed that about half found a mental health practitioner (e.g. a psychologist) through their GP.27 The stereotype that men do not seek help is gradually being disproven, with recent research highlighting that almost half of men studied who were experiencing severe depressive symptoms saw their GP five or more times in the past year, with over 90% of all men in the study seeing their GP once in the year.28
Connecting with suicidal men
There is a unique opportunity for GPs to connect with, understand and effectively transition men who seek help into the broader mental health system. Nonetheless, pressure remains for GPs to act as a ‘one stop shop’ for mental health care, even though this often exceeds the time and resources available. Worryingly, but not unexpectedly, studies have shown that GPs are often the last help-seeking service that people visit before suicide.29 A possible explanation is the finding that men do not volunteer suicidal thoughts to GPs if not directly asked, again reinforcing the need for an open, honest and trusting relationship.30
We encourage GPs to practice having frank conversations with patients about potential suicidal thoughts and also to avoid assuming that help-seeking men will offer up the full extent of their distress voluntarily. In addition, although distress remains the leading risk factor for suicidality in women, common situational stressors are uniquely important to suicidality in men, including relationship breakdown, financial insecurity and job loss. These events often interact with a male patient’s identity, self-worth and purpose, and may trigger suicidality even in those with no history of mental health difficulties.
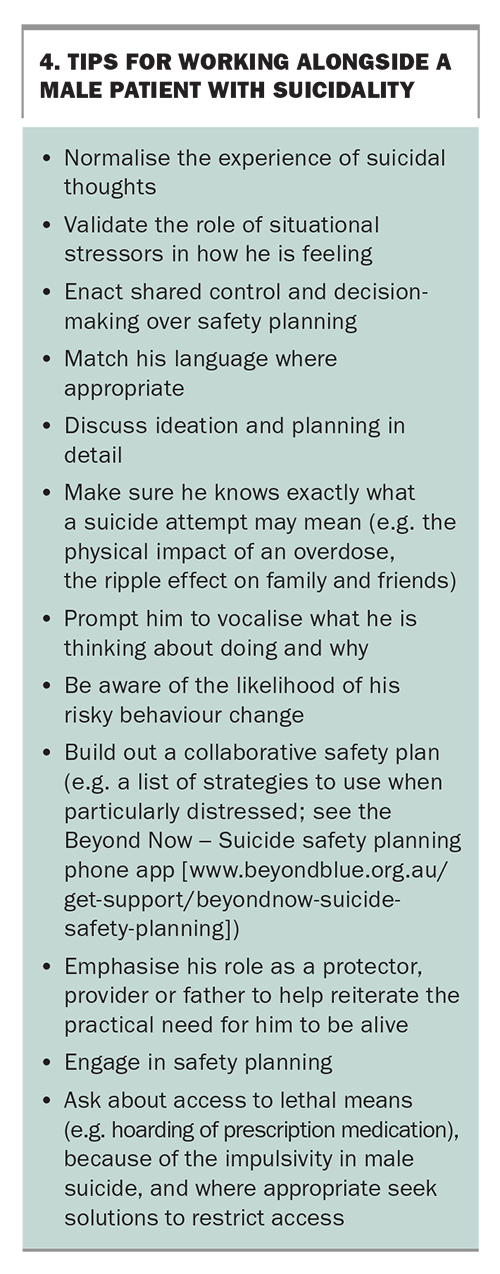
Tips for working alongside a male patient with suicidality are shown in Box 4. Having a conversation about suicidal thoughts or behaviours with your male patients may be helped by a robust doctor-patient relationship. A shared understanding and openness have specific importance in the context of men’s mental health, given the possible challenges surrounding mistrust. Research suggests that the more a man feels that their GP cares for and understands them, the more motivated they will be to pursue treatment for depression, whether pharmacotherapy or talk therapy.31
{kind=link}
Your gender, your practice
A factor that is often overlooked when considering the therapeutic relationship with male patients is the role of a practitioner’s gendered attitudes and beliefs. The way GPs interact with a male patient’s unique version of masculinity, based on their own ideas of what a man can and should be, may have implications for what eventuates in a consultation. Importantly, these beliefs are not fixed but often stem from the GP’s own gender development and generational and cultural context. We suggest these may require purposeful consideration and discussion. In a study of GPs, practitioners were found to be complicit in inadvertently reinforcing traditional masculinity norms among help-seeking men.32 Men who presented as stoic or emotionally detached were found to garner more respect from doctors, which by extension served to reinforce these qualities as typical and expected of men.
Beliefs and biases held by some practitioners about masculinity and appropriate gendered behaviours may impact on the way they approach male patients. For instance, if a young man presents with depressive symptoms, it is imperative that the practitioner does not accidentally perpetuate any of the patient’s underlying beliefs or stereotypes that help-seeking reflects weakness, dependence and powerlessness and is incompatible with masculinity, in an attempt to align with him. Practitioners are encouraged to forward the narrative of help-seeking as indicating strength and self-betterment, and to normalise and reinforce this health-seeking.
Assessment and diagnosis
For men who make it into a GP’s surgery, evidence suggests that the way they experience and express their distress may make it difficult for practitioners to detect and diagnose depression.33,34
Male-type depression
Men may express their symptoms of depression through externalising symptoms. These include:
- emotion suppression
- anger or aggression
- drug and alcohol use
- risk-taking and impulsivity
- somatic symptoms (e.g. sleep disturbance, headaches and sexual concerns).
These responses to distress can be socially condoned and understood as traditionally masculine coping behaviours, in the sense that men are thought to be socialised to take risks and resolve conflict through anger or aggression.35 The term ‘male-type depression syndrome’ has been used to describe this range of depression symptoms among men incorporating an externalising phenotype, although debate regarding a specific male depression phenotype continues.36
However, others suggest that perceived pressures on men to rigidly restrict emotional expression, or to ‘act in’ and try to resolve their issues alone, can build over time, labelled ‘the big build’.9 Depletion of the resources to suppress emotion and negative affect can then trigger externalising expression or acting out.
Screening and diagnostic criteria
Diagnostic criteria or generic screening measures for depression fail to capture the externalising symptoms described above.37,38 For instance, the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) incorporates irritability and outbursts of anger as potential criteria for major depressive disorder in children. However, the DSM-5 inexplicably drops these symptoms from the criteria for depression in adults, despite evidence for the co-occurrence of anger in men experiencing mood problems.5
Additionally, the presence of externalising symptoms such as anger, substance misuse and risk-taking in some men is coupled with a lower frequency and intensity of typical depressive symptoms such as depressed mood, appetite or sleep disturbance.39 This increases the risk of a missed diagnosis or misdiagnosis. Consequently, researchers have questioned the sensitivity of screening measures for depression in male populations.
A large representative US study found that gender discrepancies in depression symptoms are much less pronounced when externalising markers are considered, in turn suggesting we may be underestimating men’s difficulties with depression.38 Externalising symptoms such as irritability, excessive drinking, drug taking or aggression have been found to have direct links with both current suicidal risk and past suicide attempt.4 This makes them worthy of attention and assessment when working with men, above and beyond typical expressions of distress.40
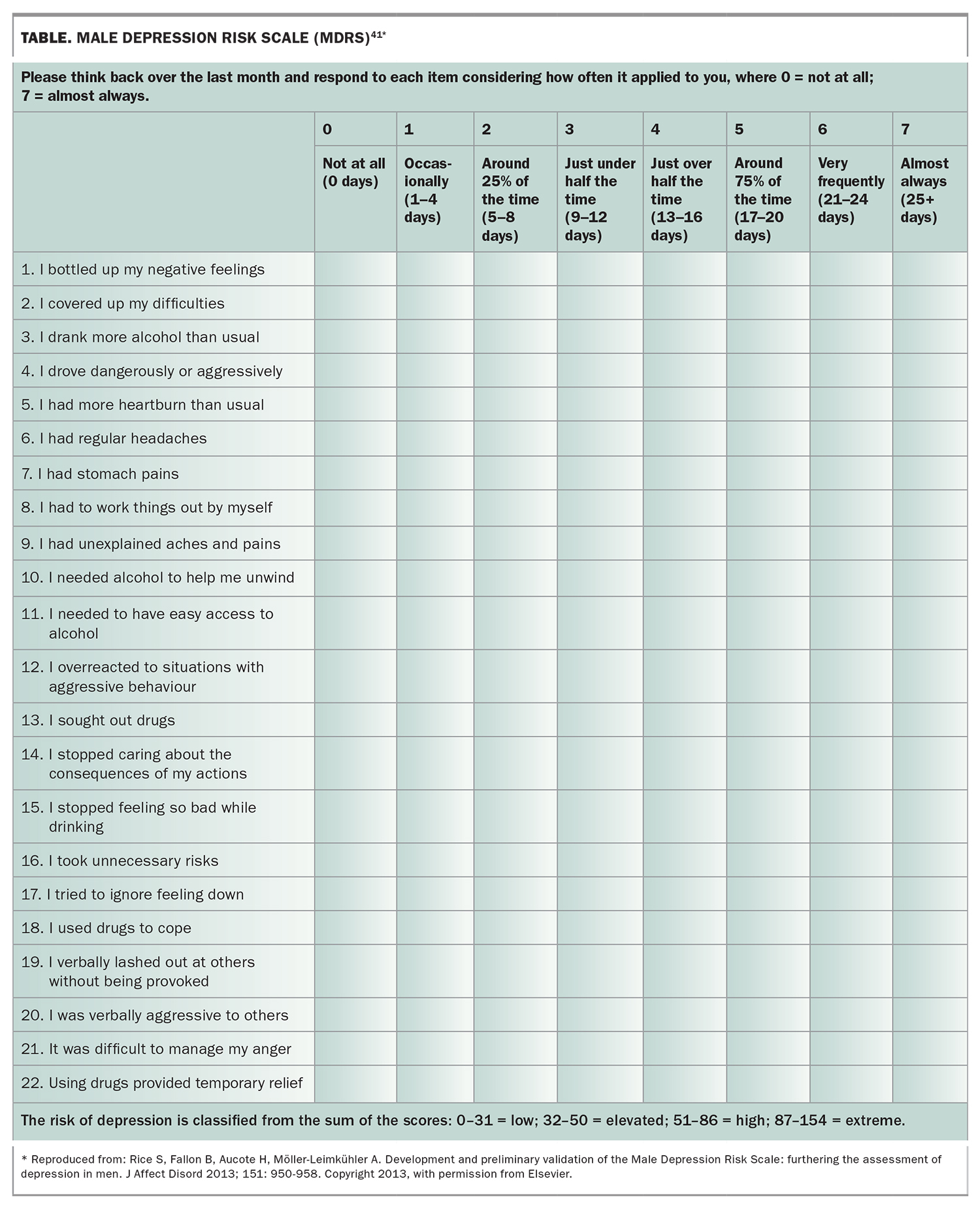
The Australian-developed Male Depression Risk Scale (MDRS) is a 22-item screening tool designed to assess externalising mood problems in men (Table).41 The MDRS has good sensitivity and specificity for identifying men reporting past two-week suicide ideation and has been validated in both younger and older men.41-44 A seven-item short form of the MDRS is forthcoming. Additionally, a prompt list has been developed for use with men in mental health discussions specifically in a general practice.45,46 Alongside a formal measure such as the MDRS, this prompt list could provide useful insight into the male patient’s experience.
{kind=link}
Treatment
As the gatekeepers for treatment of depression in men, GPs have a role that can, and should, extend beyond prescribing antidepressants as an automatic or premature response, albeit necessary in some situations. Indeed, if a male patient is at the beginning of their mental health journey, and is yet to comprehend fully their internal experience, where their symptoms stem from and how to best manage them, then less intensive psychological or lifestyle-based intervention may be more acceptable and useful.
Alongside validation, active listening and basic psychoeducation, GPs should seek out and lean on the male patient’s strengths and interests to collaboratively build a plan of action. GPs who refer a patient to a mental health clinician should ensure that the patient can openly voice to them any uncertainty or anxiety about the process, and clarify that there are always multiple treatment avenues to try. Promising to follow up with external providers will communicate to the patient that his GP is an ally with an open ear.
Conclusion
Depression may be more common in men than prevalence rates currently suggest. GPs are highly influential in driving improvement in the detection, diagnosis and treatment of men’s mental health concerns. GPs continue to confront the stresses and strains of this complex and time-consuming work to provide their male patients with the best care possible. Seeking ongoing opportunities to improve clinical engagement is essential for men with depression. Although men have historically been reluctant to reach out and engage in help-seeking for their mental health, the next generation of young men appear more open to help-seeking, making them more able and willing to grapple with mental health concerns. MT