Timing of therapy in osteoporosis: does it matter?

Osteoporosis is a common condition encountered in general practice and is significantly undertreated. Tailoring the type and timing of treatment to the individual patient is important to improve outcomes and minimise potential side effects. Many patients with osteoporosis will need indefinite treatment. Lower-risk patients who respond well to treatment may be considered for a break from treatment after five to 10 years of therapy.
- Osteoporosis causes significant morbidity and mortality but is markedly undertreated in Australia.
- All patients who have a minimal trauma hip or vertebral fracture should receive osteoporosis therapy.
- Treatment should be considered in patients with other minimal trauma fractures or with osteoporosis diagnosed by bone mineral density who have not yet fractured.
- Bisphosphonates, denosumab and hormonal therapies are effective in decreasing hip, vertebral and nonvertebral fractures.
- First-line treatment selection depends on individual patient factors and preferences.
- Breaks from drug therapy decrease the risk of rare side effects and can be considered after 5 to 10 years of continuous treatment in patients who have not had further fractures if their T-score improves to above −2.5.
- Cessation of denosumab results in rapid loss of bone mineral density and patients should transition to bisphosphonates for one to two years after its cessation.
Over 50% of postmenopausal women and 30% of older men will suffer at least one osteoporotic fracture during their lifetime. Annually, osteoporosis directly costs the Australian healthcare system over two billion dollars.1 Minimal trauma fractures of the hip, vertebrae and other ‘major’, (i.e. proximal), fractures are associated with increased mortality and this risk persists five to 10 years after the event. Treatment with intravenous bisphosphonates after hip fracture has been shown to decrease mortality by 28% and subsequent fracture of any type by 35%.2
Despite the morbidity and mortality associated with osteoporosis and availability of highly efficacious treatments, less than 20% of patients receive appropriate pharmacological management after a minimal trauma fracture.3 The burden of osteoporosis increases with population aging. The 2019 National Strategic Action Plan for Osteoporosis was created to improve prevention and management of the condition. One of the Plan’s key priorities was earlier diagnosis and therapy initiation. This article summarises therapy initiation, including the role of and relationship between the type and timing of pharmacological treatment. Review of the evidence for lifestyle intervention and dietary supplements is beyond the scope of this article.
Who to screen for osteoporosis
All patients aged over 70 years and most people aged over 50 years with a minimal trauma fracture should have a bone mineral density (BMD) scan. People aged over 50 years with multiple risk factors for osteoporosis should also be considered for a screening BMD scan. Major risk factors for osteoporosis and the risk factors for which patients receive a reimbursement for a BMD scan from the Medicare Benefits Schedule are listed in the Box.
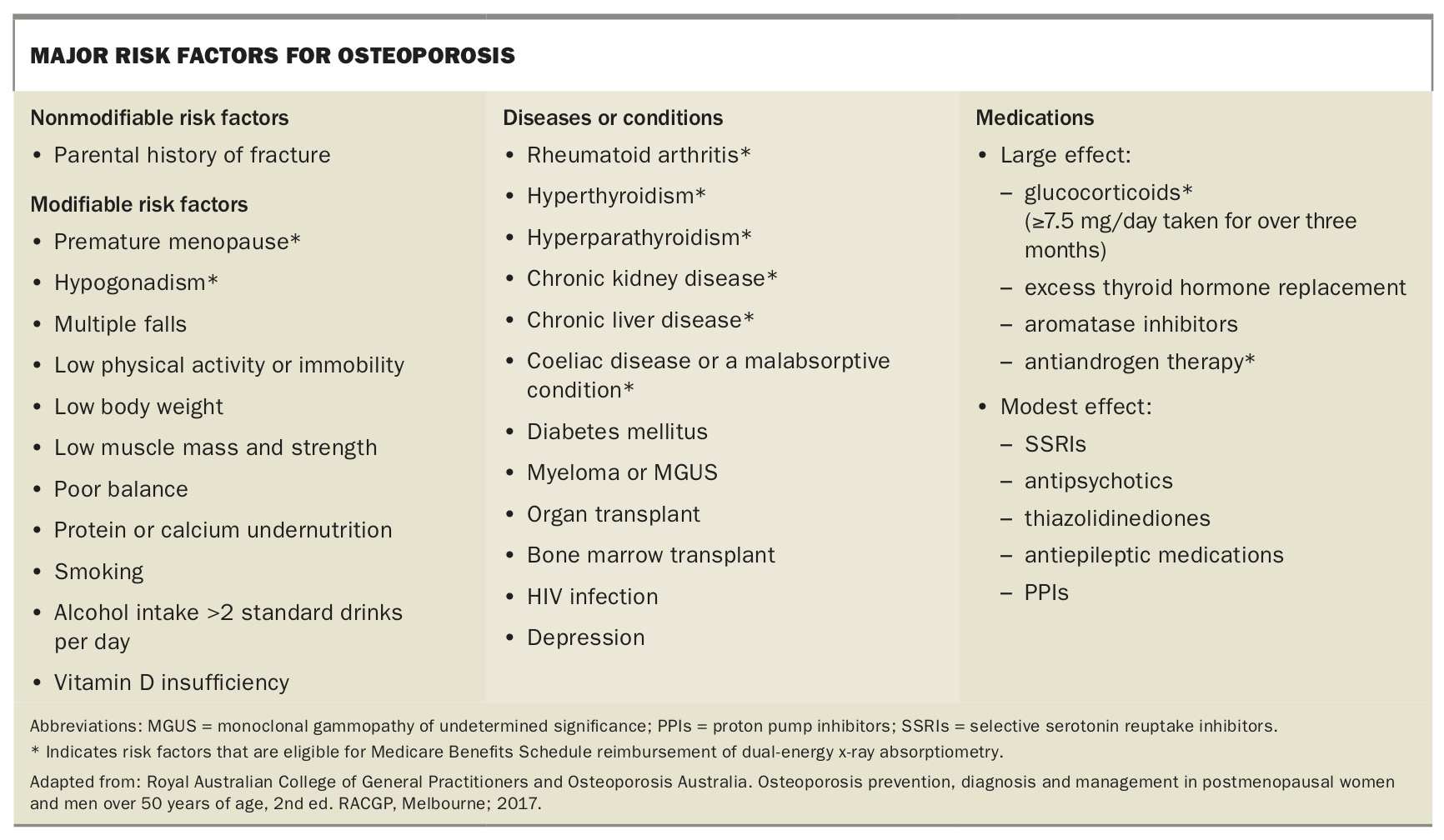{kind=link}
The diagnosis of osteoporosis is defined as a T-score of −2.5 or lower. If a classic minimal trauma osteoporotic fracture has occurred (e.g. neck of femur, vertebral compression, distal radius or other ‘proximal’ fractures), the diagnosis and treatment initiation should be made at less severe T-scores.
Types of treatment
There are two broad categories of osteoporosis medications: antiresorptive and anabolic treatments. Hormonal treatments in perimenopausal or postmenopausal women also have a place in management. The Table provides an overview of the main osteoporosis treatment options.4-10
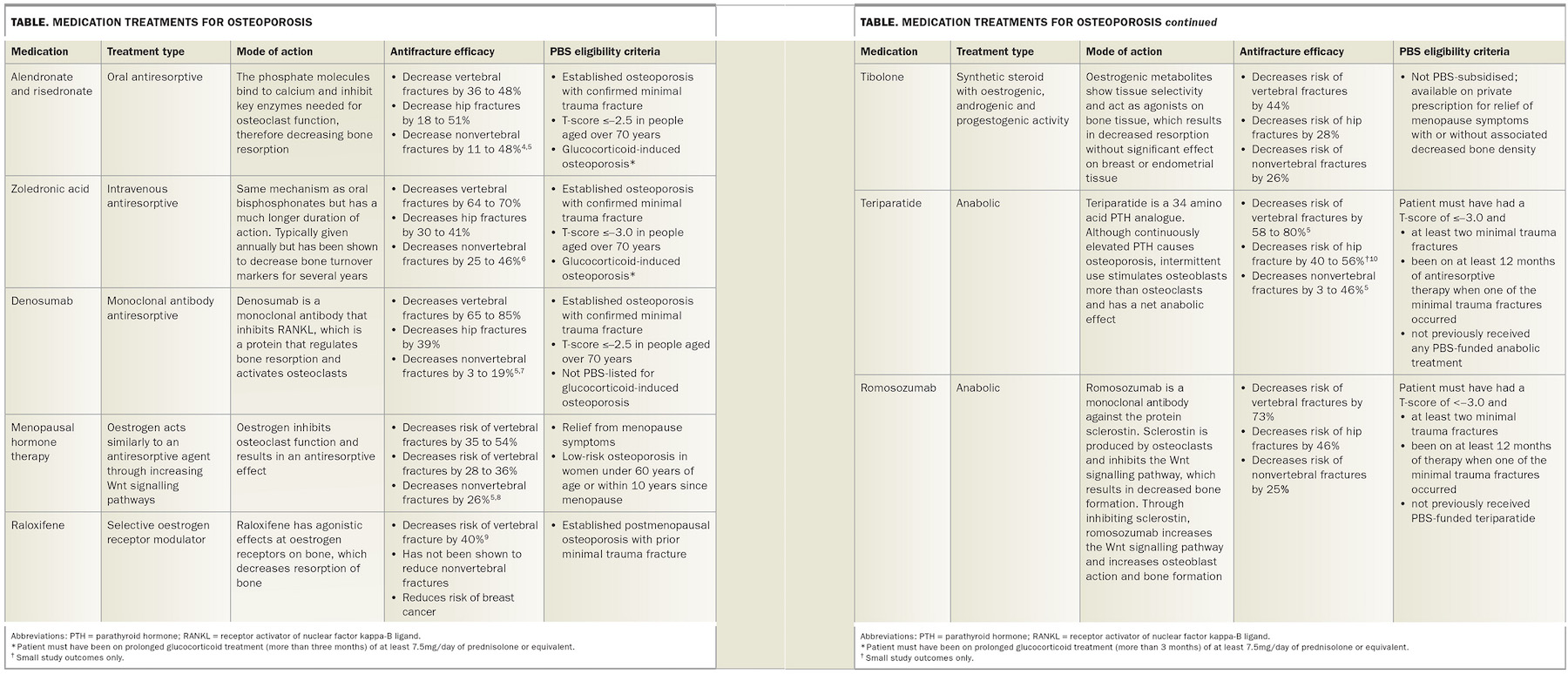{kind=link}
Antiresorptive or, in lower risk younger female patients, hormonal treatments should be first-line for most people with osteoporosis. PBS-listed antiresorptive medications include bisphosphonates or the receptor activator of nuclear factor kappa B ligand (RANKL) inhibitor, denosumab. Available bisphosphonates include oral alendronate and risedronate or intravenous zoledronic acid.
The two anabolic agents available in Australia are the parathyroid hormone analogue teriparatide and the recently added anti-sclerostin monoclonal antibody romosozumab. Both treatments are only PBS funded in the setting of recurrent fracture after at least 12 months of antiresorptive treatment and a T-score of −3.0 or lower.
Bisphosphonates bind to calcium and consequently accumulate in bone. They exhibit their antifracture efficacy through disrupting the enzymatic pathways needed for bone resorption and cause osteoclast apoptosis. Owing to their affinity for calcium, bisphosphonates remain in bone for months to years. Consequently, BMD loss after cessation, for example during a monitored treatment break, is slow.
All bisphosphonates available in Australia improve BMD and decrease fracture risk. Zoledronic acid has been shown to decrease vertebral fractures in postmenopausal women by 70% and hip fractures by 40%.4 Both oral bisphosphonates decrease hip and vertebral fractures by around 30 to 50% and reduce non-vertebral fractures by 20 to 30%.5
Denosumab is a monoclonal antibody that inhibits RANKL. RANKL is a protein that is pivotal in regulation of bone resorption through activation and action of osteoclasts. The Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months (FREEDOM) trial showed that denosumab reduced vertebral fractures in postmenopausal women by 68%, hip fractures by 40% and nonvertebral fractures by 20%.7 The FREEDOM extension trial showed that BMD continued to increase over 10 years of therapy: however, fracture risk reduction plateaued between a T-score of −2 and −1.5.11
BMD gains on denosumab are rapidly lost with cessation of treatment. Three months after cessation (nine months from the last dose), bone turnover markers rise markedly and rapid bone loss occurs. During this rapid loss, increased fracture risk has been reported. In patients stopping denosumab, using an alternative antiresorptive treatment for 12 to 18 months can ameliorate the rapid bone loss.12
Menopause is associated with a rapid increase in fracture risk due to the loss of oestrogen’s inhibitory action on osteoclasts and bone resorption. Consequently, menopausal hormone therapy (MHT), tibolone or selective oestrogen receptor modulators (SERMs) are management options for those with perimenopausal or postmenopausal osteoporosis. MHT has been shown to decrease the incidence of osteoporotic fractures by 40% for vertebral fractures, 30% for hip fractures and 20 to 30% for all osteoporotic fractures. Compared with other osteoporosis agents, MHT has a unique antifracture profile as it decreases the risk of fractures regardless of baseline BMD, even in low-risk patients.8
Tibolone may be particularly useful in women closer to menopause as it decreases hot flashes, improves vaginal lubrication and reduces breast cancer risk (in breast cancer naïve women). However, in women with a history of breast cancer, it has been associated with an increased risk of recurrence, and in older postmenopausal women was reported to increase stroke risk.13,14
SERMs may be particularly useful in postmenopausal women at risk of vertebral fracture, especially those with a personal or family history of breast cancer. However, they have not been shown to reduce hip fracture risk.15
Who to treat
There is consensus that any patient older than 50 years who experiences a minimal trauma hip or vertebral fracture should receive an osteoporosis drug treatment. For other fragility fractures, society guidelines differ, with some advocating that any minimal-trauma fracture warrants osteoporosis treatment. Guidelines also suggest the treatment decision can be based on BMD results and calculated 10-year fracture risk, rather than ‘waiting’ for a fracture to occur.
Absolute fracture risk is determined by multiple factors, including BMD, age, bone microarchitecture and the presence of other clinical risk factors. Fracture risk increases significantly with age, and in some younger patients with bone mineral densities of −2.5 or less, the risk of fracture may not exceed the threshold to start treatment, but these patients require ongoing monitoring.
Fracture risk can be calculated with the Garvan Institute of Medical Research Fracture Risk Calculator (https://www.garvan.org.au/promotions/bone-fracture-risk/calculator/) or the Fracture Risk Assessment Tool (FRAX) (https://www.sheffield.ac.uk/FRAX). Treatment is generally indicated for patients with a 10-year fracture risk of at least 3% for hip fractures or at least 20% for other fractures.16 The Garvan Institute of Medical Research Fracture Risk Calculator is simpler and, although validated in other countries, is based on Australian data.
Which treatment
Once the decision to commence treatment is made, it is imperative clinicians consider that osteoporosis is a chronic condition, and the first treatment should be made in context of a comprehensive long-term strategy that considers the patient’s personal preferences and goals.
For men and women older than 60 years, or higher-risk younger female patients, antiresorptive agents should generally be the first-line treatment. Delaying commencement of antiresorptive therapy over concern of the rare side effects, atypical femoral fracture (AFF) or medication-related osteonecrosis of the jaw (MRONJ) will result in further bone loss that is difficult to regain.
Bisphosphonates, denosumab and MHT have evidence for decreasing the incidence of vertebral, hip and non-vertebral fractures.5 Deciding which of these is the most appropriate first-line management option depends on the patient’s age and individual patient and medication factors. Specifically, the likely duration of treatment and the potential need for sequential treatment should be considered.
MHT is no longer considered a first-line therapy for osteoporosis. It may be considered in younger women with menopausal symptoms who have concomitant osteoporosis. Following the Women’s Health Initiative publication in 2002, there was an abrupt decrease in MHT prescription due to concerns of increased breast cancer, cardiovascular and cerebrovascular disease risk. This was followed by an increased incidence of fractures, especially in women who were 10 to 15 years after the onset of menopause. Individual risks will vary depending on patient and treatment factors. However in post-hoc analysis of women younger than 60 years or less than 10 years from menopause, MHT was associated with decreased cardiac and cerebral events and had a positive risk-benefit balance. Topical oestrogen is not associated with increased thromboembolic complications. In women who do not have an intact uterus and receive unopposed oestrogen, oestrogen alone has not been shown to increase the risk of breast cancer.17
Once started on MHT, BMD generally increases during the first and second year of treatment. Thereafter, if MHT is continued, BMD remains stable. When MHT is discontinued, it is appropriate to reassess the risk of osteoporotic fractures and consider transitioning to alternative antiresorptive therapy.
Denosumab requires strict adherence to the six-monthly administration and therefore should only be prescribed in patients in whom there is minimal concern regarding adherence. Hypocalcaemia can occur after administration, but adequate calcium intake and vitamin D sufficiency can reduce the risk of this occurring. The risk of hypocalcaemia is increased in secondary hyperparathyroidism and can occur with all antiresorptive agents. Consequently, secondary hyperparathyroidism should be excluded before starting treatment, particularly in patients with chronic renal disease, who are at greatest risk and thus warrant specialist management.
Cessation of denosumab results in a rapid increase in bone resorption and a return to baseline of BMD within 12 to 24 months. Fracture risk also returns to baseline, although, if a vertebral fracture had already occurred, there is increased likelihood of multiple vertebral fractures.18 Consequently, denosumab should not be stopped unless alternative therapy is initiated, generally bisphosphonates, for at least 12 to 18 months. Even with subsequent bisphosphonates, there is still loss of BMD and the best method of implementing a break from treatment on denosumab is currently a topic of contention and research. Safety data for at least 10 years of continuous denosumab treatment suggests that for older patients the medication could be continued lifelong.11
Given the concerns around bone resporption with denosumab cessation and the comparable efficacy of bisphosphonates there is no compelling reason for a patient to be started on denosumab rather than bisphosphonates for first-line osteoporosis management. When prescribing bisphosphonates, the choice of either an oral agent or intravenous zoledronic acid will depend on patient factors and preference. Their efficacy for hip and nonvertebral fractures are similar, but zoledronic acid showed a greater reduction in vertebral fractures.5
Real world data shows that adherence and persistence to oral bisphosphonates are poor, likely due to gastrointestinal side effects and the requirements of an empty stomach and to stay upright for 30 minutes afterwards.19 The enteric-coated formulation of risedronate, which can be taken with food, alleviates most of these issues. Provided the patient receives the infusion, annual zoledronic acid reduces potential issues with adherence. There is also evidence for longer treatment intervals being effective.20
All bisphosphonates can cause temporary mild myalgias and arthralgias. With zoledronic acid, 10 to 15% of patients will experience a flu-like acute phase reaction after their first infusion. Symptoms may include fever, chills, muscle aches and other flu-like symptoms. The reaction is self-limited and usually resolves within 24 to 48 hours; supportive treatment includes paracetamol and ibuprofen. It is important that patients are informed of this potential reaction and that it rarely occurs after subsequent infusions. Adequate hydration before and after the infusion is recommended to reduce the risk of kidney injury. Bisphosphonates are not generally recommended if a patient’s creatinine clearance is less than 30 mL/minute. Osteoporosis in patients with Stage IV or V kidney disease is best managed by a specialist.
Treatment duration
Osteoporosis is a chronic disease with significant morbidity and mortality risk, and treatment is generally lifelong. Indefinite treatment is often appropriate for patients who are at higher risk and need secondary prevention, as well as most people starting therapy over the age of 70 years. Antiresorptive agents are well tolerated and the benefits of treatment far outweigh the risks for most patients with osteoporosis. The Flowchart provides an approach to the primary and secondary prevention of fractures and when to reassess therapy.
The International Task Force on Osteonecrosis of the Jaw recommends that antiresorptive therapy is not a contraindication to elective dentoalveolar oral surgery but, if possible, identification and treatment of dental disease should occur before starting treatment.21 The guidelines are available online at: https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/osteoporosis/recommendations/special-issues/medication-related-osteonecrosis-of-the-jaw.
The incidence of AFFs and MRONJ for both denosumab and bisphosphonates is exceedingly low, at less than 10 per 10,000 patient years and is only marginally higher than the general population. The incidence increases with duration of treatment, especially in patients who have received more than five to 10 years of treatment. Both complications are primarily because of suppression of bone remodelling and, consequently, the main rationale for considering a monitored treatment-free period is to allow for an increase in bone resorption and absorption. Treatment-free periods are estimated to decrease the risk of atypical femoral fractures by 70% per year, but evidence for a decreased risk of MRONJ is less clear.22
It has been recommended to reconsider the need for ongoing therapy after five to 10 years of treatment. A treatment break may be appropriate for patients who have responded well to treatment (T-score above –2.5 and without any recent fractures, i.e. during the period of treatment). Treatment should generally be continued in higher-risk patients who have T-scores below –2.5 or have had any further fractures. Recurrent fracture warrants consideration of a change to an alternative agent, including anabolic therapies (teriparatide or romosozumab).
It is important to continue to monitor patients who are having a monitored treatment break with a repeat BMD scan after 12 to 24 months. Treatment should be reinitiated if a significant decrease in bone density or a fracture occurs. Patients on denosumab should have at least 12 to 18 months of alternative treatment, generally with oral or intravenous bisphosphonates, before a monitored treatment-free period can be considered. Patients who fracture on treatment or suffer an AFF or MRONJ may benefit from an anabolic agent and referral to an osteoporosis specialist is recommended.
Conclusion
Osteoporosis is a debilitating chronic condition and generally needs lifelong treatment and monitoring. Treatment should be tailored to the individual, with patient preference and clinical factors considered, as well as the potential need for sequential therapy with different agents. Denosumab has become increasingly popular in Australia, but there is some concern regarding the risk of rapid BMD loss associated with treatment cessation. Denosumab should not be prescribed in patients if there is concern of potential nonadherence and must be followed by 12 to 18 months of an alternative treatment, such as a bisphosphonate, before any break from treatment. Hormonal treatments are likely underused in younger women, and have a favourable risk–benefit profile in many women under 60 years of age. Bisphosphonates are efficacious and safe agents, and are appropriate first-line management in many patients with osteoporosis aged 50 years or older. Anabolic agents require prescription from a specialist physician and should be considered in the setting of fractures despite treatment with a bisphosphonate or denosumab. MT