Type 2 diabetes: tailoring a treatment approach


Diabetes type 2
Diabetes medicines
The past decade has seen major advances in therapies for type 2 diabetes, leading to a wide array of treatment options. Management should involve a patient-centred approach with individualised glycaemic targets and selection of medications based on comorbidities, cost and patient preference.
- Early and optimal glycaemic control in patients with type 2 diabetes is imperative for reducing microvascular and potentially macrovascular complications.
- Glycated haemoglobin (HbA1c) remains the key focus of glycaemic management although targets should be individualised based on age, comorbidities and life expectancy.
- There is a vast array of therapies available and treatment algorithms provided by the Australian Diabetes Society offer guidance on treatment selection.
- Treatment choice should be guided by patient comorbidities, adverse effect profile, acceptability of the method of administration and cost (PBS subsidy).
- Metformin remains first-line treatment unless contraindicated. Insulin may be considered at any stage, particularly where control is poor (HbA1c above 75 mmol/mol [9%]).
- Patients with pre-existing cardiovascular disease can be safely managed with new agents, including some DPP4-inhibitors, GLP-1 receptor agonists and SGLT-2 inhibitors, and some therapies may offer cardiovascular mortality benefit.
Picture credit: Fertnig/iStockphoto.com Model used for illustrative purposes only
Type 2 diabetes represents a significant challenge to public health in Australia. With the emergence of the obesity epidemic there has been a steady increase in the prevalence of type 2 diabetes and it has been forecast that between 2000 and 2050 the number of cases in Australia will increase by more than threefold.1 Furthermore, type 2 diabetes is becoming increasingly common in younger patients, and now accounts for 31% of new diagnoses of diabetes in young adults aged 15 to 19 years.2 Research has shown that in 2000, the total estimated annual healthcare cost attributed directly to type 2 diabetes was over $630 million.1
The rapid rise in new diagnoses demands clinicians are well educated in the management of this condition. Additionally, potential micro- and macrovascular complications reinforce the need for early control, not only to improve health outcomes for individual patients, but also to mitigate the impact of the disease burden on the Australian economy.
HbA1c targets and individualising goals
Glycaemic control remains the principal focus of diabetes management, with glycated haemoglobin (HbA1c) targets dictating most treatment decisions. It is well established that control of blood glucose levels is associated with reductions in the rates of microvascular complications and possibly also the macrovascular complications of myocardial infarction (MI), stroke and all-cause mortality.
Several seminal trials have emerged over the past 25 years that have informed clinicians about the ideal targets for HbA1c. It is now accepted that the targets should be individualised based on factors including age, other comorbidities and life expectancy.
Key trials on glycaemic targets
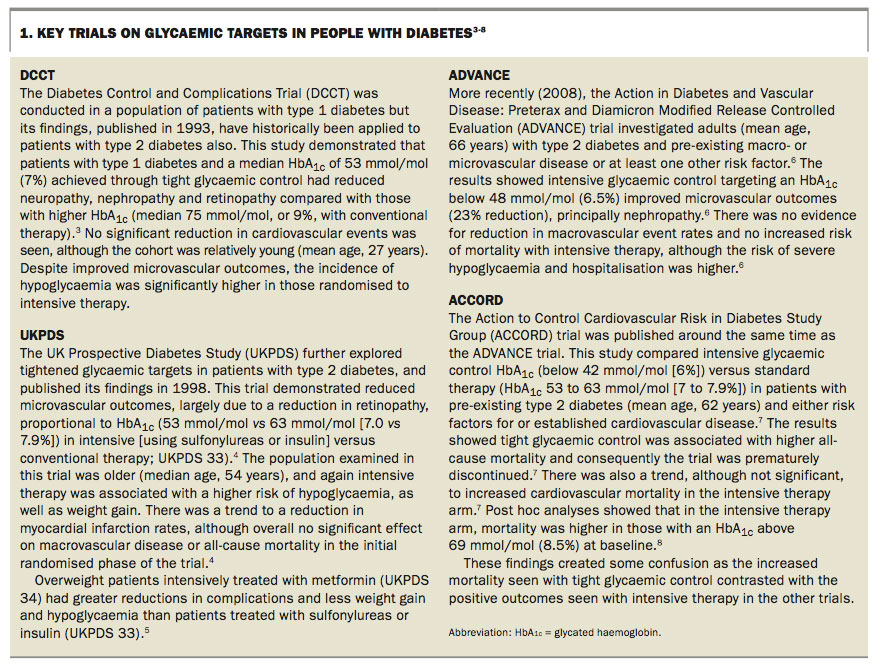
Among the wealth of research in the area of reducing diabetes-related end points through achieving HbA1c targets, four key randomised controlled trials have contributed significantly to the current diabetes management principles. These trials are discussed in Box 1.3-8
{kind=link}
The legacy effect of the glycaemic target trials
Long-term follow up of the four key large clinical trials has shown that tight control in the period following diabetes diagnosis can have a sustained effect for years to come, even if glycaemic control is later relaxed. Results from the UKPDS 10-year follow up found early glycaemic control (HbA1c below 53 mmol/mol [7%]) mitigated long-term risk of any diabetes-related end point and microvascular disease.9 The risk of diabetes-related death, MI and death from any cause was also lower in those who received intensive therapy early despite later merging of HbA1c from the two arms (sulfonylurea–insulin group and metformin group).9 This concept was termed the ‘legacy effect’, and supports optimal glycaemic control in the early stages of disease.8 It emphasises the importance of considering duration of type 2 diabetes when tailoring treatment.
Recommended glycaemic targets
Based on the body of evidence, the Australian Diabetes Society has developed guidelines to assist clinicians in decision-making in this area, the position statement Individualisation of Glycated Haemoglobin Targets for Adults with Diabetes Mellitus.10These recommendations are endorsed by the Royal Australian College of General Practitioners (RACGP) and are available in their and Diabetes Australia’s current guidelines, General Practice Management of Type 2 Diabetes: 2016–18.11
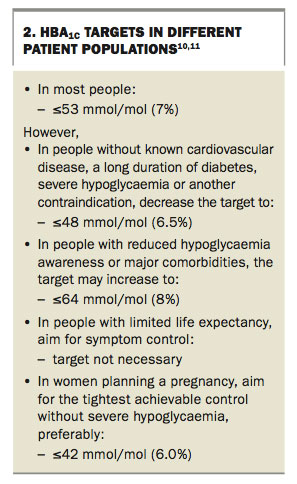
It is generally accepted that an HbA1c target of 53 mmol/mol (7%) should be aimed for in most cases, with recommended targets tightened (≤ 48 mmol/mol, or 6.5%) or relaxed (≤ 64 mmol/mol, or 8%) in some individuals (Box 2).10,11
{kind=link}
Cardiovascular risk of glucose-lowering agents
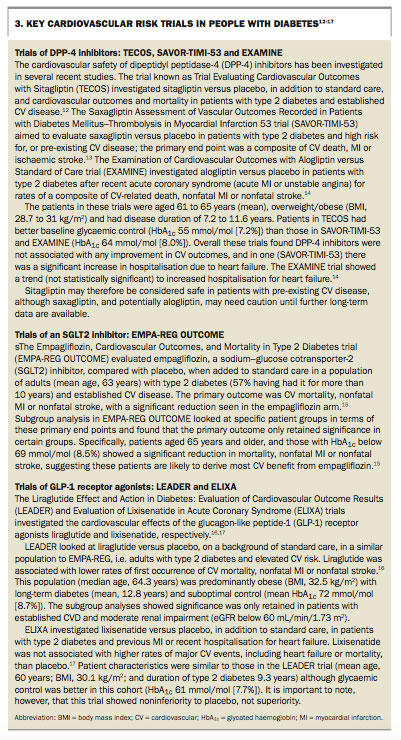
The link between type 2 diabetes, cardiovascular disease (CVD) and related mortality is well established. Recently a few major trials have investigated the cardiovascular risk of glucose-lowering agents, because of concerns about a lack of long-term safety data in this area. The results of these trials may assist clinicians in choosing agents for patients with both of these issues. The trials are discussed in Box 3.12-17
{kind=link}
Interpreting the key cardiovascular risk trials
To date the evidence from these major cardiovascular risk trials of various glucose- lowering agents suggests the relative safety of DPP-4 inhibitors in type 2 diabetes and CVD, albeit a higher risk of heart failure with saxagliptin and possibly alogliptin. SGLT2 inhibitors, specifically empagliflozin, and GLP-1 receptor agonists, specifically liraglutide, appear to confer a CV benefit patients with established CVD. Several key trials investigating other agents within these classes are currently under way.
The findings from these trials, however, need to be interpreted in the context of the populations in which they were conducted. Important points to consider include the age and sex of the patients, the duration of pre-existing diabetes, the presence of comorbidities including microvascular and cardiovascular disease, the initial HbA1c and the use of concomitant therapies. The risk of hypoglycaemia also needs consideration. Furthermore, the results could possibly apply only to the agent trialled, and not necessarily be a class effect.
Treatment options
The past decade has witnessed major advances in treatment options for type 2 diabetes, leading to a shift in the management paradigm. With the rise in prevalence of this condition, there are still a significant number of patients who do not meet current recommendations for glycaemic targets. Analysis of medical records in primary care in Australia from 2005 to 2013 found that 40% of patients had elevated HbA1c.18 This is in part due to treatment inertia. Health practitioners now have a range of choices in therapy aimed at regulating blood glucose control with concomitant focus on reducing the incidence of specific comorbidities such as obesity and limiting adverse effects. Inevitably, with disease progression, many patients will require insulin therapy, although in the interim there are many available options for glycaemic control.
Most patients with type 2 diabetes are managed in the primary care setting with specialist involvement where necessary. The first step in management should be establishing the goals of therapy. An individualised glycaemic target should be identified based on patient age, comorbidities and life expectancy.19 This target should be regularly reviewed and adjusted, as necessary, to match the patient’s specific characteristics and their current health status.
Lifestyle modification with dietary advice and an exercise plan should be the first prescription, with particular attention to weight management. An ideal body weight should be recommended, with a plan to achieve this. Although weight loss to target is recognised as challenging, and is not often achieved in practice, any improvement in body weight should be encouraged. Initial goals may focus on small improvements in weight, with both short- and long-term goals set and reviewed at each appointment. Beyond these recommendations, depending on initial glycaemic control at diagnosis or where glycaemic targets are not met, a proactive approach should be exercised with escalation of combination therapy as needed.
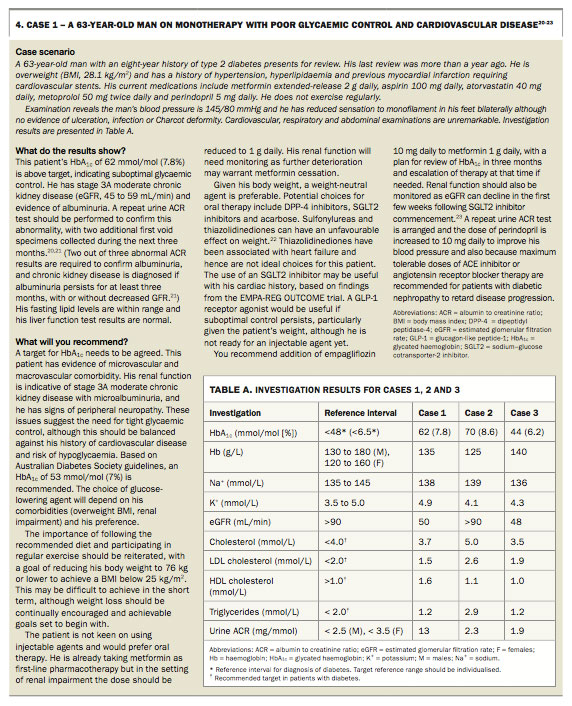
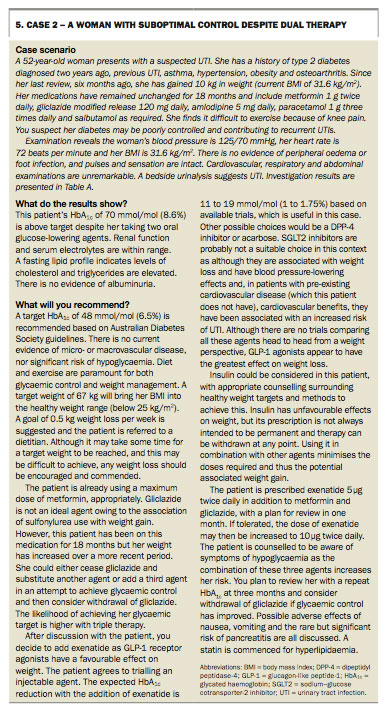
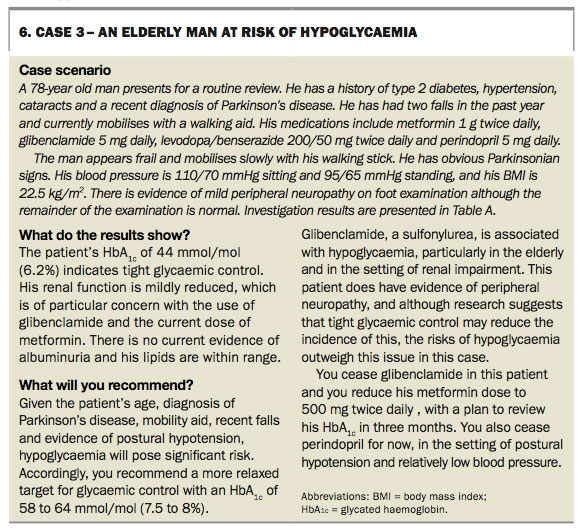
The case studies in Boxes 4 to 6 illustrate the tailoring of treatment to individuals.20-23
{kind=link}
{kind=link}
{kind=link}
Choice of therapy and specific considerations
With an increasing array of treatment options, decisions in therapy may not be simple. Overall the fundamental principle of management is a patient-centred individualised approach. In recognition of the complexity of such decision-making, the Australian Diabetes Society has published a treatment algorithm to assist medical practitioners in both medicine selection and recommendations for glycaemic targets (Figure; algorithm available online at http://t2d.diabetessociety.com.au).10,11,19
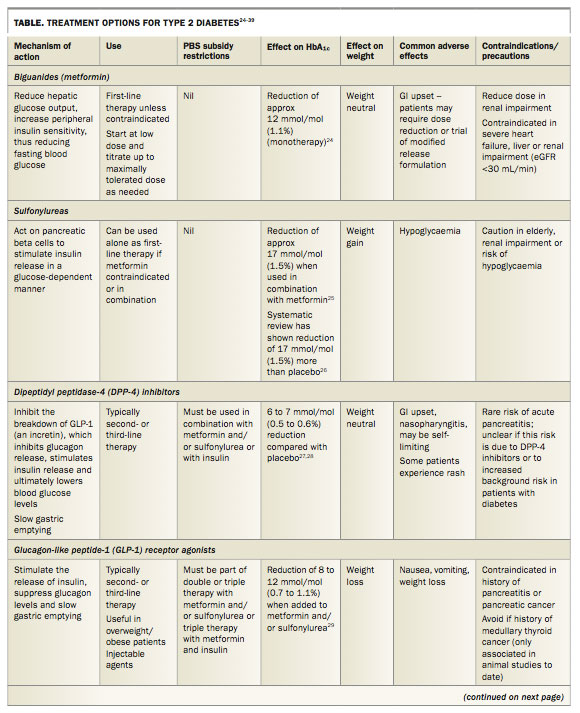
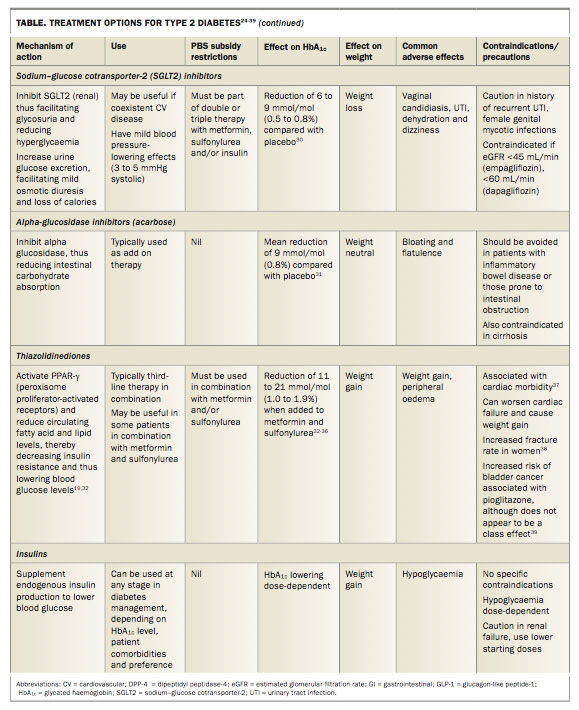
Specific drug classes currently available include biguanides (metformin), sulfonylureas, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, thiazolidinediones, alpha-glucosidase inhibitors (acarbose) and sodium–glucose cotransporter-2 (SGLT2) inhibitors, as well as different insulins with various lengths of action. A summary of available treatment options is presented in the Table.24-39
{kind=link}
{kind=link}
First-line therapies
Metformin remains the first-line treatment, unless contraindicated. Its suitability as primary therapy is supported by the UKPDS data showing an association with reduced all-cause mortality.5 This finding has been repeated in a recent large meta-analysis.40
Second- and third-line therapies
Although the choice of second- and third-line agents is less prescriptive than that of a first-line agent, it should be guided by patient comorbidities, adverse effect profile and acceptability of the method of administration. Government subsidy (PBS) is also an important consideration, as cost plays a significant role, particularly where multiple agents are necessary.
Common choices for second-line therapies include sulfonylureas, DPP-4 inhibitors and SGLT2 inhibitors. GLP-1 receptor agonists can also be used second line, although they may be less favoured by patients because they are administered by injection. Specific comorbidities may influence the choice of agent. For example, where weight is a concern, GLP-1 receptor agonists and SGLT2 inhibitors may have a favourable role. If patients have established CVD, sitagliptin will be safe, although the SGLT2 inhibitor empagliflozin may provide benefit. If the risk of hypoglycaemia is of particular concern, sulfonylureas should be dose-reduced, particularly in combination therapy, or avoided. Unless contraindicated or poorly tolerated, metformin should be continued; it should be noted that many agents are available in combination form with metformin. PBS restrictions may stipulate certain combinations must be trialled before other agents can be introduced.
There are now many approved combinations, containing triple oral or combined oral and injectable agents, for use as third-line therapies. Again, metformin should be continued wherever possible.
Insulin may be considered at any stage in therapy, particularly where glycaemic control is significantly poor (HbA1c > 75 mmol/mol [9%]). Insulin has often been used in combination therapy with metformin, although more recently has been approved for use in combination with DPP-4 inhibitors, GLP-1 receptor agonists and SGLT2 inhibitors. Weight gain is a recognised side effect of insulin, although this should not necessarily deter its prescription. In combination with other agents, insulin can be used at lower doses, thus minimising weight gain. Additionally it can be withdrawn at any point depending on the individual patient, and thus does not need to be used in an ongoing sense if effects are unfavourable.
Treatment of specific patient groups
Renal failure
The choice of treatment for patients with type 2 diabetes and renal failure is limited because of altered drug metabolism and associated risks of adverse effects, including hypoglycaemia. Such considerations become more important with advancing chronic kidney disease (CKD), particularly when estimated glomerular filtration rate (eGFR) is below 30 mL/min (stages 4 and 5 CKD), and medications may require dose reduction or cessation if contraindicated.
Metformin is contraindicated if eGFR falls below 30 mL/min because of a risk of lactic acidosis. Sulfonylureas have a higher risk of hypoglycaemia with renal impairment. SGLT2 inhibitors rely on renal function for their mechanism of action and should be avoided if eGFR is below 45 to 60 mL/min, depending on the agent. Within the class of DPP-4 inhibitors, sitagliptin can be used up until stage 4 CKD with dose reduction and linagliptin can be used regardless of eGFR and can be used in patients on dialysis.19 Insulin is safe to use, but downtitration of dose may be necessary.
Elderly patients
In elderly patients, glycaemic control should be individualised based on life expectancy, polypharmacy and the risk of hypoglycaemia. In many cases, symptom control should be the sole focus of therapy. A decline in renal function, often seen in this age group, requires caution or dose reduction with multiple therapies.
Conclusion
The key principle in managing type 2 diabetes is individualised treatment. Metformin remains the first-line recommended therapy, unless contraindicated, and insulin may be commenced at any stage in therapy. Beyond these recommendations, clinicians have a wide choice in management options. Targets for HbA1c and treatment choices should be guided by patient comorbidities, life expectancy, acceptability of administration, cost and patient preference. MT
References