Nonmelanoma skin cancer. Symptoms, signs and treatment

Skin cancer
GPs are at the forefront of the detection and early management of nonmelanoma skin cancers, which are the most common skin cancers encountered in general practice.
- Australia has one of the highest rates of skin cancer in the world.
- GPs play a vital role in the detection and early management of nonmelanoma skin cancer.
- Actinic keratoses can develop into squamous cell carcinomas.
- Squamous cell carcinomas can metastasise and lesions with histological margins less than 1mm require further treatment.
- Basal cell carcinomas are the most common nonmelanoma skin cancer in Australia; their treatment is determined by site and subtype.
Picture credit: © Evgeniy Kalinovskiy/adobe.stock.com
Australia has one of the highest rates of skin cancer in the world, with nonmelanoma skin cancers (NMSCs) the most common types encountered. Cancer registries do not routinely report NMSC, but the latest age-standardised incidence rates (from 2002) were estimated to be 884 per 100,000 people for basal cell carcinoma (BCC) and 387 per 100,000 for squamous cell carcinoma (SCC). These rates are expected to be increasing.1 This translates to an estimated cost to Medicare of more than $700 million annually.2
GPs are at the forefront of managing this burden. Skin conditions account for 15.9% of GP consultations, and skin cancers are the most common reason for specialist referral.3 This high consultation rate also presents GPs with the opportunity to educate patients on sun-safe behaviour and to detect skin cancers at the earliest opportunity. Patient education should include information on ultraviolet (UV) light exposure risks and sun protection measures.
This article summarises the presentation and treatment of actinic keratosis (AK), which is the most common type of precancerous skin lesion, and the two most common types of NMSC – BCC and SCC.
Actinic keratosis
Presentation and diagnosis
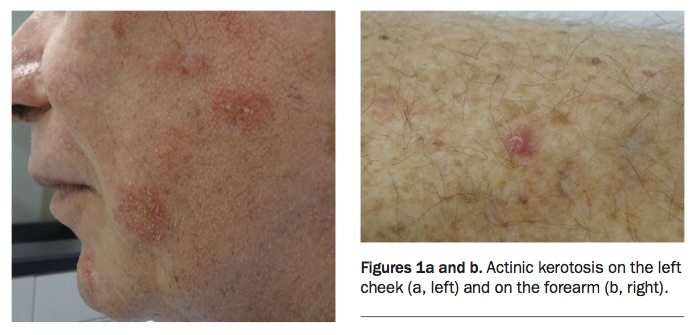
AK, also known as solar keratosis, is one of the most common lesions GPs encounter. AKs are precancerous lesions that are often found on sun-exposed areas, such as the face, scalp, ears and back of the hands (Figures 1a and b). AK and SCC are distinguishable by the extent of keratinocyte atypia; in AK, it is confined to the lower portion of the epidermis, but in SCC it occupies the entire epidermis and infiltrates through to the dermis. The reported rate of development from AK to SCC varies widely, between 0.025% and 16%.4
{kind=link}
AK has varied clinical presentations, with a lesion classically described as a scaly macule or papule on an erythematous base that is 3 to 6mm in diameter, often with rough yellow or white scale. However, AK can also present as hyperkeratotic, pigmented, lichenoid or atrophic lesions. The lesions are often asymptomatic but may sting or itch.
In addition to the concern about its possible progression to SCC, the clinical significance of AK is that the presence of multiple lesions is an indication of significant UV light exposure. This exposure is a risk factor for other nonmelanoma (and indeed melanoma) skin cancers, which should be considered during a patient’s consultation and treatment. A full skin check should be regularly undertaken for patients with multiple AK lesions.
The diagnosis of AK is predominantly clinical. The use of palpation is particularly of benefit because of the rough nature of the lesions. A biopsy should be considered if there is concern that the lesion may be an early SCC. Hallmark signs of concern include tenderness, bleeding, inflammation and thickness of the lesion.
Treatment
Treatment of AK may comprise localised treatment or field therapy. To determine the most appropriate treatment, consider the number of lesions, their size and location, and patient factors such as age and compliance with therapy. Lesions may spontaneously regress, especially if strict sun protection measures are followed, but the clinical course is nevertheless difficult to predict.
Liquid nitrogen cryotherapy is usually the first-line localised treatment for AK. The application of liquid nitrogen (stored at -196°C) to the affected area, which causes superficial cellular damage, can be performed using a cryospray or cryoprobe device. The duration of therapy varies depending on lesion size and location, but a freeze of about three to five seconds is usually recommended.5 Other lesions, such as seborrhoeic keratoses and superficial BCCs, can also be treated with cryotherapy, but may require longer freeze times due to factors such as the thickness of the lesion. Curettage and shave treatments can also be considered for AK, although these are often reserved for larger and thicker lesions.
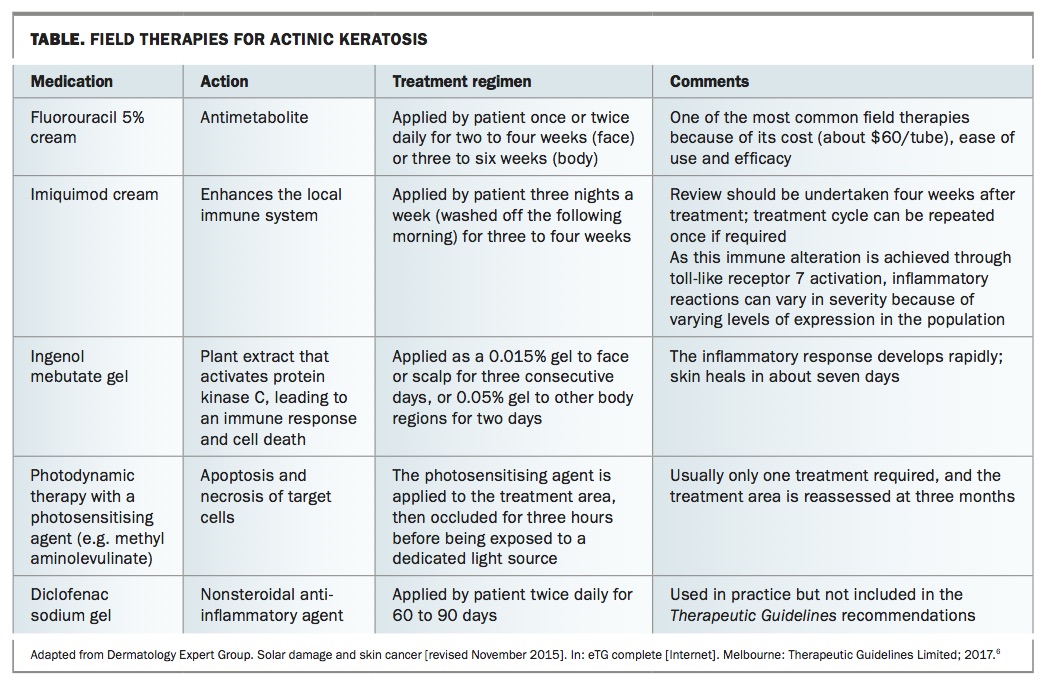
Field therapies should be considered for areas that contain multiple AKs. The main field therapies are fluorouracil 5% cream (5-fluorouracil), imiquimod cream, ingenol mebutate gel, photodynamic therapy and diclofenac sodium gel (Table).6 As these therapies work by inducing an inflammatory reaction, including redness, soreness and crusting, counselling patients, including showing them pictures of expected reactions, is recommended before starting therapy.
{kind=link}
Squamous cell carcinoma
Presentation and diagnosis
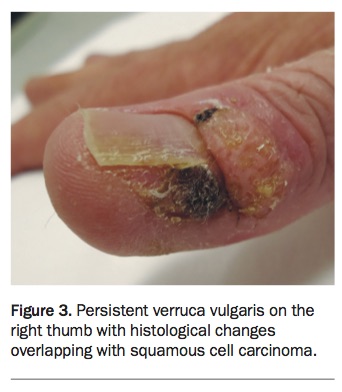
SCC is the second most common skin cancer in Australia, behind BCC (Figures 2a and b). It can arise de novo, develop from AK or be associated with infection (oncogenic subtypes of human papillomavirus), sites of chronic inflammation or previous trauma (Figure 3). The two main risk factors for SCC are cumulative UV light exposure, which damages the keratinocyte DNA and impairs the immune system, and Fitzpatrick skin type, which alters susceptibility to UV effects due to the level of melanin present (types I to III are the most susceptible). The primary concern with SCC is its ability to metastasise, which accounts for about 20% of deaths from skin cancer.7
{kind=link}
{kind=link}
SCCs can be described across a spectrum that starts with in situ SCC (Bowen’s disease), then further defined using the TNM (tumour, nodal, metastasis) staging system. Clinically, Bowen’s disease presents as an erythematous patch or plaque with scale. It can also be pigmented. The histopathological definition of Bowen’s disease is full-thickness epidermal keratinocyte atypia. Once there is involvement of the dermis, the lesion has become an invasive SCC. Without treatment, Bowen’s disease progresses to invasive SCC in 2 to 5% of cases. Invasive SCC presents as an erythematous, keratotic papule or nodule, which is often tender.
There is debate about the inclusion of keratoacanthoma in the SCC spectrum, but guidelines from the Cancer Council Australia state that it is likely a form of SCC.1 Keratoacanthomas have traditionally been thought of as relatively benign squamoproliferative lesions that do not have the ability to metastasise. However, they grow very quickly and are often of concern to patients. Keratoacanthomas present as erythematous crateriform nodules with a central keratin core. Although they can spontaneously resolve within six to 12 weeks, early excision is nevertheless recommended because of their clinical appearance and, more importantly, to definitively rule out an SCC, which can be difficult to do without histological analysis of the entire lesion.
Diagnosis of SCC is confirmed with a biopsy. If invasive SCC is suspected, it is important that the biopsy sample is taken from deep enough to determine the extent of dermal invasion. It is also important to examine regional lymph nodes, with suspected metastases confirmed by fine-needle aspiration. Poor prognostic factors include immunosuppression and lesions arising in scar tissue and ear, lip, mucosal, anogenital, head and neck sites. The four main histological signs for poor prognosis are lesion size greater than 2cm, poorly differentiated histology, invasion beyond subcutaneous fat and perineurial involvement.
Treatment
Treatment of SCC is by margin-controlled surgical excision, with the margins varying between 2 and 10mm depending on lesion characteristics. Favourable lesions (e.g. those that are well differentiated and less than 2cm in diameter) are adequately cleared with a margin of 4mm in 95% of cases.1 As incomplete excision carries up to a 50% risk of recurrence, lesions with histological margins of less than 1mm must be considered for further therapy. Mohs surgery can be undertaken at sites where tissue conservation is paramount, such as the nasal tip, and for high-risk lesions. Radiation therapy can be used when there is greater surgical risk (e.g. due to patient comorbidities or lesion site) and as adjuvant treatment for high-risk lesions.
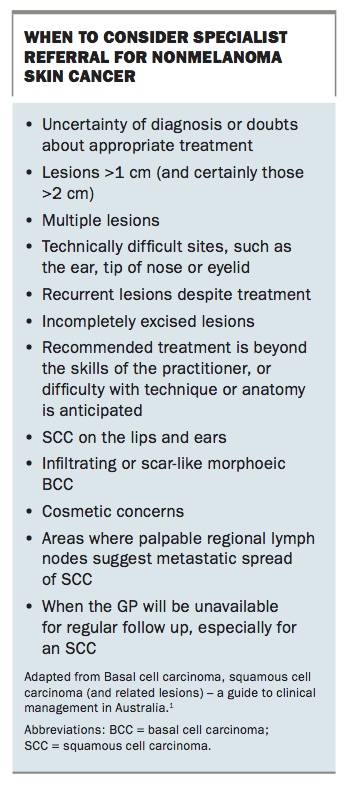
Topical therapies, such as cryotherapy, imiquimod cream, 5-fluorouracil and photodynamic therapy, can also be used to treat Bowen’s disease when surgery is not advised. Further details on therapy duration and high-risk definitions are given in the Cancer Council Australia guidelines.1 Recommendations on when to refer patients to specialist care are shown in the Box.
{kind=link}
Basal cell carcinoma
Presentation and diagnosis
BCC is the most common skin cancer in Australia. As with SCC, Fitzpatrick skin type and UV radiation exposure are the biggest risk factors; however, unlike SCC, risk is associated with intense episodes of burning, not cumulative exposure. BCCs rarely metastasise and the main clinical concern is local destruction.
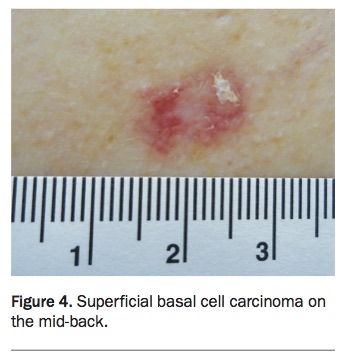
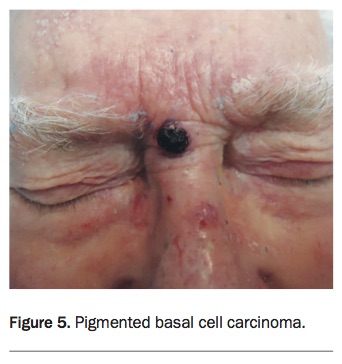
BCC has multiple clinical presentations, with the most common being nodular BCCs. These are pearly papules or nodules with evident telangiectasia and/or umbilication. They may ulcerate and are most often seen on the head and neck, including areas with little sun exposure, such as the inner canthus or behind the ears. Superficial BCCs present as erythematous patches or plaques, often on the trunk or extremities (Figure 4). BCCs may also be pigmented (Figure 5), leading to a clinical differential diagnosis of melanoma, but an evident pearly edge and vascularity, seen clinically or through the dermatoscope, can aid in the distinction. Less common variations include morphoeic or sclerosing (scar-like), micronodular and basosquamous BCC. Diagnosis of BCC is confirmed with a biopsy.
{kind=link}
{kind=link}
Treatment
Treatment is determined by the subtype and site of BCC. Superficial BCCs can be treated with topical therapies, including imiquimod cream, cryotherapy, curettage and cautery and photodynamic therapy.6 Imiquimod treatment for BCC is more intensive than for AKs, with therapy applied by the patient five nights a week for six weeks. It can be used in low-risk sites, such as the trunk and facial areas including cheeks and forehead. Cryotherapy for BCC is performed with a double freeze–thaw cycle of 20 to 30 seconds. This causes a significant blister and can leave hypopigmentation, so it is important to counsel patients before starting treatment. Cryotherapy is not recommended for use on areas where healing is a concern, such as the lower legs. Curettage and cautery can be undertaken for well demarcated lesions, on suitable patients and sites. Photodynamic therapy can be used for superficial and thin nodular BCCs. It usually requires two treatment sessions, one week apart, with lesions first descaled or debulked, and the sensitising agent applied to a thickness of 1mm, with a margin of 5mm.1
Surgical treatment is usually first-line therapy for nonsuperficial BCCs, although radiation therapy is an option if surgery is contraindicated. High-risk lesions should be excised with clinical margins of 3 to 4mm. Histological margins less than 1mm require further evaluation and potentially further treatment. Favourable BCCs should be excised with 2 to 3mm margins, and histological clearance of 0.5mm. Where neither surgery nor curative radiation therapy is an option, oral therapy (e.g. vismodegib) targeting the hedgehog signalling pathway is available on the PBS with authority. Patients requiring this treatment should be under specialist care.
New therapies
Studies and clinical trials are underway to improve treatment options and outcomes for patients with NMSC. Areas of research are focusing on immune pathways, new oral and topical treatments and advances in radiation therapy.
Researchers at the University of Sydney are exploring photoimmunology – the role UV radiation has on altering the immune system. Although at a relatively early stage, the aim of this research is to explore how photoimmunology can be manipulated to treat SCC.8 Further development of drugs targeting the hedgehog pathway is an area of interest in advanced or metastatic BCC, and therapies targeting the epidermal growth factor receptor are being explored for use with SCC.9
Two oral therapies that have begun to be adopted for preventing NMSC in people at high risk are retinoid therapy and nicotinamide (vitamin B3). Oral retinoid therapy is already recommended for renal transplant patients,10 and its benefit in reducing the risk of NMSC has been shown in trials. For example, in an Australian crossover study of 23 patients, treatment with the retinoid acitretin reduced SCC development by 144%.11 Nicotinamide, a cheaper medication with fewer side effects, has shown significant and promising results in reducing the number of new NMSCs and AKs. A recent phase III study in Australia showed a 23% decrease in new NMSCs in high-risk patients taking daily nicotinamide supplements, compared with placebo.12
Both these oral therapies are only effective during active treatment and should be considered in consultation with a specialist. Topical therapy with combination low-dose fluorouracil (0.5%) and 10% salicylic acid has been shown to be effective in treating hyperkeratotic AKs.13 Fluorouracil–salicylic acid is available overseas but not in Australia.
Advances in radiation therapy have led to new treatment modalities that allow for shallower treatment zones, protecting deeper tissues and resulting in fewer side effects and better cosmesis.14
Conclusion
NMSC is the most common skin cancer encountered in Australia, and GPs are at the forefront of patient interaction for these conditions. Prevention (through sun-safe education), early detection and appropriate treatment help reduce the impact these cancers have on patients’ lives and the healthcare system. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.