Keeping your patients healthy on a cruise

On a cruise ship, a confined community of people from around the world travels to exotic locations, increasing the risk of contagious diseases such as influenza and norovirus infections. The pre-cruise travel health consultation should include risk assessment, appropriate immunisation and advice on a personal medical kit and on preventing and treating common problems.
The number of people going on cruises is growing around the world, with Australian cruise passengers increasing by about 20% annually for the past 10 years.1 In 2016, almost one in every 18 Australians went on a cruise.2
This article discusses common health risks on cruises and medical care likely to be available. It outlines the issues to cover in a pre-travel health consultation for prospective cruise passengers and management of common conditions, including seasickness and norovirus gastroenteritis.
Health risks on cruise ships
The modern cruise ship is larger than an aircraft carrier and may carry more than 6000 passengers and 2000 crew. Cruise ships are semi-closed communities, where large numbers of passengers and crew from around the world are confined in a relatively small space, consume the same sources of food and water and travel to exotic and remote locations. All these factors increase the risk of contagious diseases. In addition, cruise ships offer a wide range of onboard activities that may lead to injury, particularly in inexperienced, unfit passengers, including rock climbing, roller skating, ice skating, watersliding, flowriding and skydiving simulators.
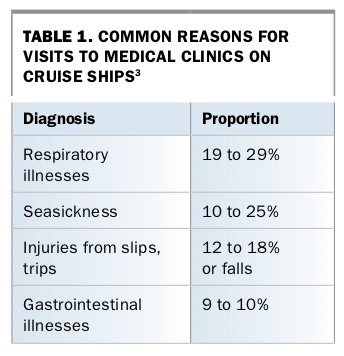
Most visits to medical clinics on cruise ships are due to acute illnesses, including dental problems.3 Almost all patients are managed onboard, with only 5% requiring medical evacuation or transfer to land-based health facilities.3 Urgent or emergency treatment is required by 3 to 11% of patients. The most common diagnoses are respiratory illnesses, seasickness, injuries and gastrointestinal illness (Table 1).3
{kind=link}
Influenza is the most common vaccine-preventable illness on cruise ships. As crews and passengers come from all over the world, influenza outbreaks occur year-round, caused by strains circulating in different regions. Legionnaire’s disease, although not common on cruise ships, has caused intermittent outbreaks. Norovirus is responsible for more than 90% of outbreaks of gastroenteritis with a confirmed diagnosis on cruise ships. Between 2010 and 2015, eight to 16 outbreaks of norovirus infection occurred on cruise ships annually.3
Many crew members on cruise ships come from developing countries with low immunisation rates. Despite health screening of crews, outbreaks of measles, rubella, meningococcal disease and varicella have been reported on cruise ships.3
About 50% of passengers who seek medical care on cruise ships are older than 65 years.3 Death rates for cruise ship passengers range from 0.6 to 9.8 deaths per million passenger-nights, mostly from cardiovascular events.3
Pre-cruise travel health consultation
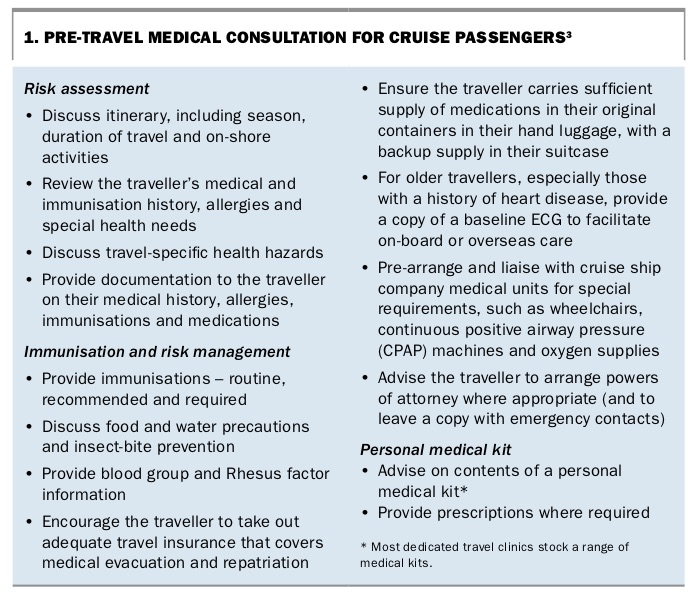
As for other travellers, the pre-travel medical consultation for prospective cruise passengers should take place well before departure. Medical expertise, vaccines and malaria chemoprophylaxis may not be available on cruise ships, and vaccination may require time to become effective. Points to cover in the pre-travel consultation are outlined in Box 1.
{kind=link}
Personal experience of cruise ships and the medical facilities on board is valuable when advising travellers. During a cruise, the ship,s medical staff are usually happy to take passengers who are fellow medical practitioners on a guided tour of the medical centre.1
Vaccinations
Cruise passengers should be up to date with the following vaccinations:
- routine vaccinations (depending on age)
– tetanus/diphtheria/whooping cough
– poliomyelitis
– measles, mumps, rubella
– chickenpox
- recommended vaccinations
– influenza (perhaps the single most important vaccination for cruise passengers)
– hepatitis A (generally indicated if visiting developing countries)
– typhoid (destination specific, often optional)
- required vaccinations for specific destinations
– yellow fever
– poliomyelitis.
Other vaccinations may be indicated depending on the patient’s itinerary, specific medical conditions and personal preferences. These include hepatitis B, meningococcal, pneumococcal, Japanese encephalitis and rabies vaccinations.
Regular medications
Passengers should take with them an adequate supply of their usual medications for the entire cruise. The specific medication (or an appropriate substitute) may not be available on board or in ports. Generally, ship’s doctors do not have prescription authority in local ports. It is almost impossible to obtain controlled medication on cruises. Passengers should carry in their hand luggage all medications in the original containers, along with a copy (ideally both paper and digital) of the prescription and/or an accompanying letter from their medical practitioner. They should take a back-up supply of critically indispensable medication in their suitcase.
Personal medical kit
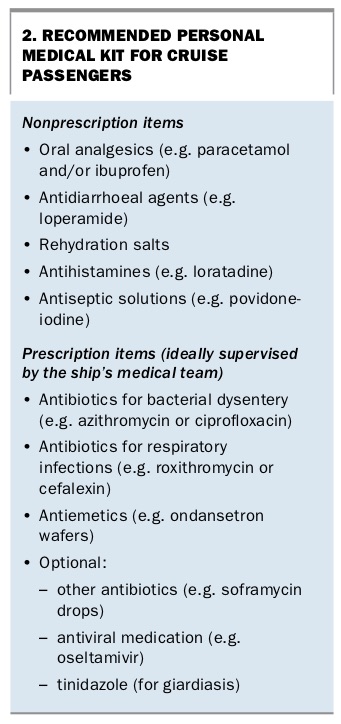
The contents of a personal medical kit should be individualised according to each passenger’s medical conditions and itinerary. Recommended essential items in addition to the passenger’s regular medications are listed in Box 2. This list is not exhaustive.
{kind=link}
Although passengers are recommended to carry a supply of commonly required antibiotics, empirical self-treatment with antibiotics on a cruise can sabotage efforts to control outbreaks. Ship’s doctors generally prefer pre-travel health providers to instruct passengers not to take antibiotics empirically; self-treatment of a condition such as norovirus gastroenteritis for two to three days before presentation can increase the risk of a large outbreak on board. Pre-travel health providers should advise passengers to report any vomiting and diarrhoea to the ship’s medical centre immediately at any time of the day or night.
Medical services on cruise ships
Availability of vaccines, medication and diagnostics
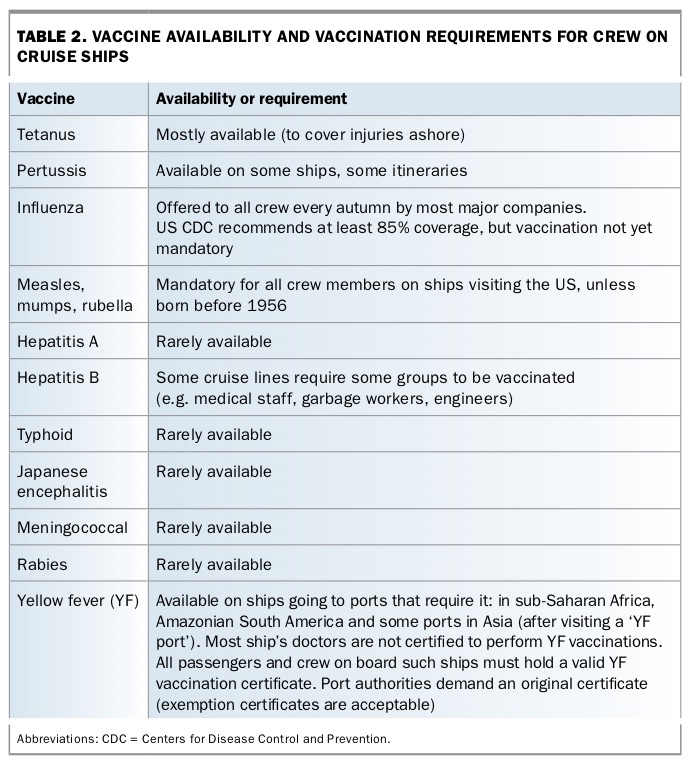
The availability of pharmaceutical items varies between cruise lines, ships and -itineraries. Doxycycline is available on most ships travelling to malaria-endemic regions (Professor Eilif Dahl, University of Bergen, Norway, personal communication). Some ships carry quick diagnostic tests for malaria. Most ships carry diagnostic tests for influenza A and B, Legionnaire’s disease and Helicobacter pylori.4 Ships equipped to perform blood transfusions may also test for HIV and hepatitis. The availability or requirement for vaccines also varies between ships (Table 2).
{kind=link}
Cost of medical services on cruise ships
The cost of medical services varies between ships but is generally expensive and is almost never covered by Medicare or private health insurance, even on cruises within Australian waters. All medical expenses are added to the room services bill and are payable before disembarkation. The importance of premium travel insurance cannot be overemphasised, ideally covering any pre-existing medical conditions.
The Department of Foreign Affairs and Trade advises on its Smart Traveller website that ‘Medicare benefits are only payable to cruise passengers if you are travelling between two Australian ports, with no intermediate stops outside Australia, and services are provided by a Medicare eligible doctor’ (https://smartraveller.gov.au/Pages/default.aspx). Even when a vessel is sailing from one Australian port to another, there is no requirement that any doctor employed on board be registered with the Australian Health Practitioner Regulation Agency. Most ship doctors are not registered to practise in Australia and do not have Medicare provider numbers.
Medical charges are generally higher on ships that are more ‘upmarket’. Charges for US-registered cruise lines are based on the 50th percentile of the usual, customary and reasonable (UCR) rates in the US (former Chief Medical Officer, Royal Caribbean, personal communication 2016).5 An average consultation costs between US$100 and $200 for a walk-in visit for a new patient, with extra charges for medical supplies, medication and nursing. An emergency medical evacuation from the Pacific islands could cost $60,000 or more (former Chief Medical Officer, Carnival Corporation, personal communication 2016).
Regulations on pregnant women and infants
Many cruise lines require pregnant women to provide a medical letter stating their expected due date and confirming that the pregnancy is not high risk and both the woman and her unborn child are healthy enough to travel. Because of concerns about potential pregnancy complications and the possibility of preterm birth, most cruise lines (with the exception of river cruises) do not accept passengers who will enter their 24th week of pregnancy at any time during the sailing. Most cruise ships are not equipped to care safely for a premature newborn. Moreover, a baby born in interna-tional waters on a ship flying a foreign flag may be rendered stateless. Without passport and visas, it is a diplomatic challenge to bring the baby home.
The minimum age limit for passengers is three months on most cruise lines and six months on some.
Common medical concerns on cruise ships
Seasickness
Seasickness is caused by a disturbance between equilibrium and balance in the nervous system. While travelling on a ship, the eyes see the surrounding fixtures as stable, whereas the body senses that it is tilting with the ship. This generates conflicting messages to the brain.
Children aged between 2 and 12 years are more likely to experience motion -sickness on the sea, in the air and in cars. Women are also more prone to experience motion sickness, especially when pregnant, menstruating or using menopausal hormone therapy.
Seasickness remedies
Seasickness remedies such as motion sickness wristbands and bracelets that exert pressure on acupuncture points and ginger tablets are minimally effective in most cases.
Medications for seasickness
Antihistamines are the most often used medications for seasickness. Nonsedating antihistamines are generally not effective. Oral promethazine alleviates symptoms but also induces drowsiness.
Hyoscine hydrobromide tablets work well if taken before the ship sails. They are not recommended for children younger than 2 years. An injection of prochlorperazine or metoclopramide, which accelerates gastric emptying, may be required if seasickness is severe. Ondansetron is not effective in preventing seasickness but attenuates the nausea and vomiting.
Other medications to treat seasickness that may be available on cruise ships or overseas, possibly over the counter, include cinnarizine tablets, a sedating oral antihistamine, and hyoscine hydrobromide transdermal patches. These patches are applied to the hairless area behind the ear about four hours before needed and deliver 1 mg of hyoscine hydrobromide over three days. They are contraindicated in people with acute angle glaucoma or pre-existing gastrointestinal or urinary obstruction and should be used with caution in older people because of the increased likelihood of -central nervous system effects such as confusion and agitation.
Hyoscine hydrobromide transdermal patches are effective if used correctly but are unpopular with ship’s doctors and are not available on most cruise ships. The most common side effect is prolonged pupil dilation on the side of the body where the patch is applied, which is inconvenient for the patient on sunny days and confusing for doctors who need to assess a head injury.
Passengers should be advised to trial any seasickness medication on land well before their departure to become aware of any adverse reactions. All preventive medication should be taken before the onset of symptoms, preferably before the ship sails.
Norovirus infection
Norovirus is a nonenveloped single- stranded RNA virus, formerly termed Norwalk-like virus. It is a global cause of traveller’s diarrhoea and viral gastroenteritis. Although sometimes incorrectly referred to as ‘stomach flu’, it has no biological association with influenza viruses.3,6 Norovirus is transmitted primarily through the faecal-oral route. It may be spread directly by person-to-person contact or indirectly via contaminated water or food, aerosols of vomitus and contaminated surfaces and objects (fomites). Norovirus is highly contagious. An infected person can shed billions of norovirus particles, but as few as 18 are required to infect another person; 1000 people could be infected by the amount of virus that could fit on a pin head.
Norovirus survives routine cleaning procedures. Viral contamination of fomites may persist during and after outbreaks. On a cruise ship, these fomites often lead to recurrent outbreaks on successive cruises with newly boarded passengers.
There are many different types of noroviruses, and people can be infected many times. Although it is possible to develop immunity to specific types, it is not known how long this immunity lasts. This may explain why so many people of all ages are infected during norovirus outbreaks.
Norovirus outbreaks
Norovirus outbreaks occur far more commonly on land than on ships. Nevertheless, more than 90% of gastroenteritis outbreaks with a confirmed cause on cruise ships that call into US seaports are caused by norovirus.3 Between 2007 and 2016, almost 2000 cruise ship voyages arrived in Sydney; 98 cases of onboard gastroenteritis were reported, 40 of which were attributed to norovirus.7 In early January 2018, about 200 passengers on a cruise ship from New Zealand bound for Brisbane were infected with norovirus.8
Presentation and management
The incubation period of norovirus infection is 12 to 48 hours. Symptoms include acute onset of vomiting and nonbloody diarrhoea, often accompanied by abdominal cramps, nausea and low-grade fever. The illness is usually self-limiting, with full recovery after one to three days. Passengers with gastrointestinal symptoms, even if mild, should promptly inform the ship’s medical centre and follow isolation and other infection control guidance. Treatment of norovirus infection is mainly supportive.
Prevention
There is no vaccine for norovirus, although vaccine development is advancing. Passengers and crew should always maintain stringent personal hygiene on board and on shore. Frequent hand washing with soap and water is essential, particularly before eating and after using the toilet. Alcohol based hand sanitisers may be useful between hand washing but do not deactivate the virus and hence are not a substitute for soap and water. Other prevention measures include maintaining a courteous but healthy distance from other passengers and crew and doing the ‘fist bump’ (also termed the ‘cruise bump’) instead of a handshake (Figure). Sick passengers should use their own toilet instead of shared facilities.
{kind=link}
Health risks ashore: vector-borne diseases
Mosquito-borne diseases are a possible risk for cruise passengers. However, as cruise ships sail mainly in the evening and overnight and are seldom moored in port between dusk to dawn, the risk of contracting malaria is generally low. Personal protection against insect bites (PPE) alone is sufficient in most cases. Malaria chemo-prophylaxis may be indicated on cruises with frequent late shore excursions and longer overnight tours in malaria-risk regions. In areas where dengue fever, Chikungunya and Zika viruses are endemic, PPE is crucial for passengers who go on land tours during the day.
Tick-borne diseases are a potential risk for passengers who go ashore in some regions. PPE against ticks should be used by passengers on cruises to the east coast of the US and adjacent parts of Canada if they go on tours to forested regions during warm seasons, to protect against Lyme disease. Similarly, PPE is important for passengers on river cruises in continental Europe with a potential risk of tick-borne encephalitis.
Mal de debarquement syndrome
After disembarking from a cruise, passengers typically continue to feel ‘at sea’, unable to regain their ‘land legs’. The sensation has been described as similar to walking on a mattress or trampoline. Although most passengers experience this land sickness temporarily after disembarking, in some it persists for weeks, months or even years. Mal de débarquement syndrome (MdDS) is more common in women, with the age group 41 to 50 years most likely to be affected. Management of this uncommon condition requires input from a specialist neurologist. Further information and resources about MdDS are available on the website of the MdDS Foundation (www.mddsfoundation.org).
Conclusion
A pre-travel consultation is highly recommended for people planning a cruise and should cover risk assessment specific to the patient and itinerary, vaccination needs and planning a personal medical kit. Advice on preventing or treating common problems such as influenza, seasickness and norovirus infection is indispensable. The value of travel insurance should be emphasised. As with other travel, expert comprehensive medical advice and pre-paration will help ensure a healthy and enjoyable cruise. MT
Acknowledgements
The author thanks Professor Eilif Dahl, ship’s doctor and Professor in Maritime Medicine at the University of Bergen, Norway, for his encouragement and for sharing his experience.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.