Navigating the new diabetes drugs: cardiovascular benefits and when to use

Diabetes type 2
Diabetes medicines
The recent introduction of antihyperglycaemic medications that not only improve glycated haemoglobin (HbA1c) levels but also provide cardiovascular, renal and overall mortality benefit renews hope for better management of diabetes. The new sodium-glucose cotransporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists are potential game changers for people with type 2 diabetes.
Diabetes is a major contributor to morbidity and mortality among people in Australia. An estimated 1.2 million (6%) Australian adults have been diagnosed with diabetes, with about 85% having type 2 diabetes.1 Diabetes results in more than one million hospitalisations annually and contributes to about 10% of the 160,000 deaths in Australia each year, and these numbers are rising.1,2 Improved glycaemic control in people with type 2 diabetes aims to prevent complications such as stroke, acute myocardial infarction, heart failure, amputation, end-stage kidney disease and blindness.
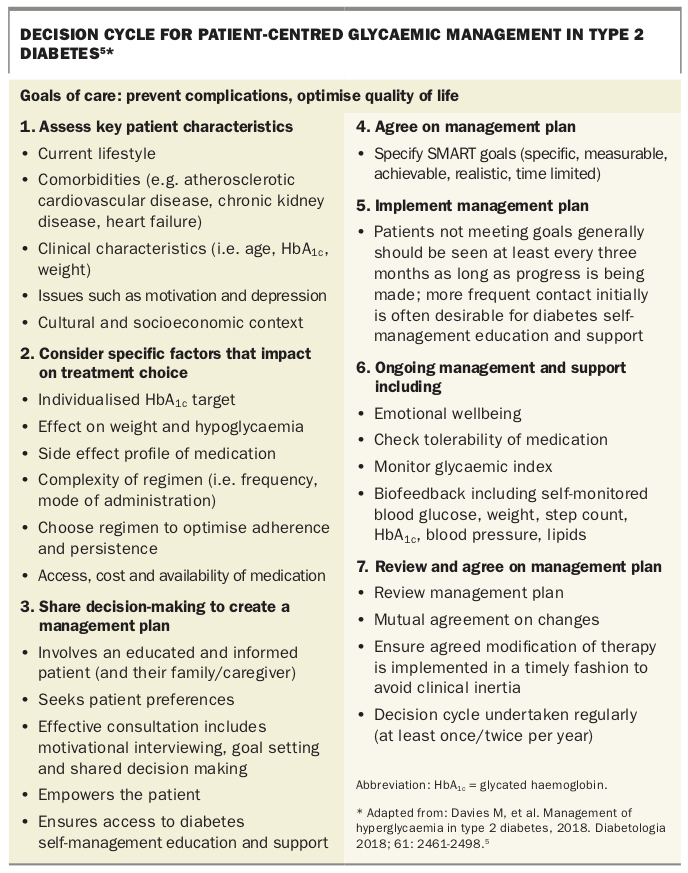
GPs are at the front line of managing type 2 diabetes and play a crucial role in regularly assessing and modifying medications in patients with this progressive disease. Guidelines for the management of type 2 diabetes from the Australian Diabetes Society and Royal Australian College of General Practitioners include a progressive algorithm to guide GPs on how to intensify antihyperglycaemic medications in a stepwise manner.3,4 Additionally, the joint position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) on management of hyperglycaemia in type 2 diabetes recommends how to tailor prescribing to the individual’s characteristics and comorbidities and how to create a management plan in conjunction with each patient (Box).5
{kind=link}
The ADA/EASD statement features use of the sodium-glucose cotransporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists, which have now been shown to provide cardiovascular and mortality benefit in populations with diabetes who are at risk of or have cardiovascular disease (CVD). These medications are potential game changers for people with type 2 diabetes. The statement also highlights the importance of regular review of patient progress in achieving the agreed glycated haemoglobin (HbA1c) target, with routine uptitration or addition of medications to avoid clinical inertia.5
This article provides an overview of the SGLT-2 inhibitors and GLP-1 receptor agonists. It summarises their side effects, the evidence supporting their use and tips on prescribing.
SGLT-2 inhibitors
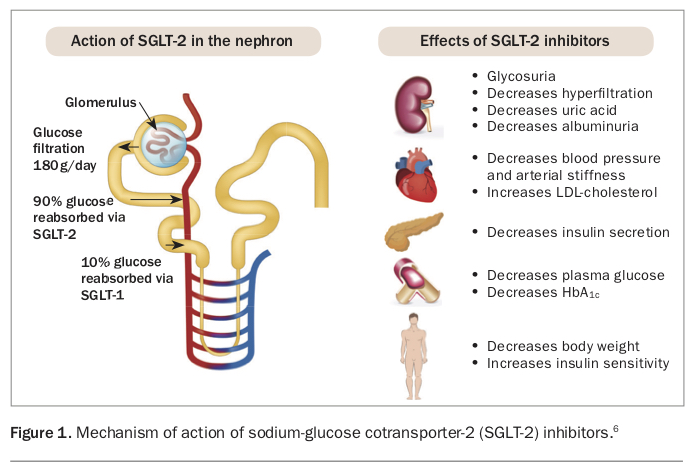
SGLT-2 is a high-capacity sodium and glucose transporter protein that is present in the proximal tubule of the nephron, where it is responsible for 90% of glucose reabsorption from urine into the bloodstream.6-9 It is also present in the enterocytes of the small intestine. Inhibition of SGLT-2 blocks glucose and sodium reabsorption in the nephron, leading to significant glycosuria and natriuresis, resulting in a reduction in plasma glucose levels and low-level diuresis (Figure 1). This is accompanied by a reduction in weight and blood pressure, with no increased risk of hypoglycaemia.
{kind=link}
The SGLT-2 inhibitors approved for use in Australia are dapagliflozin, empagliflozin and ertugliflozin. Canagliflozin is no longer available in Australia.
Side effects
Use of an SGLT-2 inhibitor is associated with an increased risk of genital infections caused by glycosuria. A slight increase in the risk of urosepsis has also been reported, although some studies have suggested that the overall rate of urinary tract infections and pyelonephritis is not significantly different.9-11 Given the osmotic diuresis that accompanies glycosuria, other effects such as polyuria, volume depletion and postural hypotension can occur, as well as a transient impairment in renal function.9,10,12 Case series of euglycaemic ketoacidosis in patients who are physically stressed by illness or concurrent surgical procedures have also been reported. The Australian Diabetes Society and Australian and New Zealand College of Anaesthetists have released statements advising routine cessation of SGLT-2 inhibitors during the perioperative period to reduce this risk.9,10,13,14
Trial evidence
The EMPA-REG OUTCOME trial examined empagliflozin in patients with established atherosclerotic CVD.9 It showed a significant reduction in the composite endpoint of nonfatal myocardial infarction, nonfatal stroke, cardiovascular mortality and all-cause mortality. In addition, empagliflozin significantly reduced hospitalisation for heart failure and progression of chronic kidney disease, which was defined as development of macroalbuminuria, doubling of the serum creatinine level, initiation of renal replacement therapy or death from renal disease. No significant difference in outcomes was seen between the 10 mg and 25 mg empagliflozin doses.9,15,16
The DECLARE-TIMI 58 trial examined dapagliflozin in a mixed patient population with or without established atherosclerotic CVD.17 It showed a significant reduction in the composite outcome of cardiovascular death or hospitalisation for heart failure (primarily because of a lower rate of hospitalisation for heart failure) and in progression of chronic kidney disease. However, it did not demonstrate a statistically significant reduction in nonfatal myocardial infarction, nonfatal stroke or all-cause mortality.
Canagliflozin (not available in Australia) was examined in the CANVAS program (involving CANVAS and CANVAS-R) in patients with high cardiovascular risk, involving either a history of, or at least two risk factors for, atherosclerotic CVD.18 It showed a significant reduction in the composite endpoint of cardiovascular death, nonfatal myocardial infarction and nonfatal stroke, as well as a lower risk of hospitalisation from heart failure, progression of albuminuria and reduction in kidney function. However, canagliflozin was associated with an increased risk of both minor and major amputations that has not been seen in other SGLT-2 inhibitor trials.
The first trial to specifically examine renal endpoints in patients taking an SGLT-2 inhibitor was the CREDENCE trial, which examined the use of canagliflozin in patients with established kidney disease.19 The trial was stopped after interim analysis showed a significant reduction in the composite endpoint of end-stage kidney disease, doubling of serum creatinine level and death from renal or cardiovascular causes. The increased amputation risk seen in the CANVAS trial was not replicated in the CREDENCE trial.
The VERTIS-CV trial examining the cardiovascular and renal benefits of ertugliflozin in patients with established atherosclerotic CVD is currently in progress.20
Several mechanisms have been proposed to contribute to the benefits of SGLT-2 inhibitors, which are seen as a class effect across many of those currently on the market in Australia and other countries. These mechanisms include changes in arterial stiffness, vascular resistance, cardiac function and cardiac oxygen demand, as well as reductions in albuminuria, uric acid, glucose levels, weight, adiposity and blood pressure.9,15,16
Prescribing tips
SGLT-2 inhibitors should be considered for use in patients with established atherosclerotic CVD and an HbA1c above the target level despite other antihyperglycaemic medications. SGLT-2 inhibitors should be avoided in patients prone to genital or urinary tract infections and used with caution in patients already taking loop diuretic therapy. SGLT-2 inhibitors should be withheld during the periprocedure period or when fasting.
Empagliflozin is available as a single agent and in fixed-dose combinations with metformin or linagliptin. It should be commenced at a dose of 10 mg daily, which can be increased to 25 mg daily as required. Empagliflozin is currently contraindicated in people with a creatinine clearance less than 45 mL/min.21
Dapagliflozin is available as a single agent and in fixed-dose combinations with metformin or saxagliptin. It is used as a single dose of 10 mg daily. Dapagliflozin is currently contraindicated in people with a creatinine clearance less than 60 mL/min and should be avoided in those with severe hepatic impairment.22
Ertugliflozin is available as a single agent and in fixed-dose combinations with metformin or sitagliptin. It should be commenced at a dose of 5 mg daily, which can be increased to 15 mg daily as required.Ertugliflozin is currently contraindicated in people with an estimated glomerular filtration rate less than 45 mL/min/1.73m2.23
Current PBS criteria require SGLT-2 inhibitors to be used in combination with metformin, a sulfonylurea, a dipeptidyl peptidase 4 (DPP-4) inhibitor (gliptin) or insulin in patients with an HbA1c higher than 7%.24,25 The exception is ertugliflozin, which is not subsidised for use with insulin.26 SGLT-2 inhibitors are not subsidised as monotherapy or in combination with a thiazolidinedione or GLP-1 receptor agonist.
GLP-1 receptor agonists
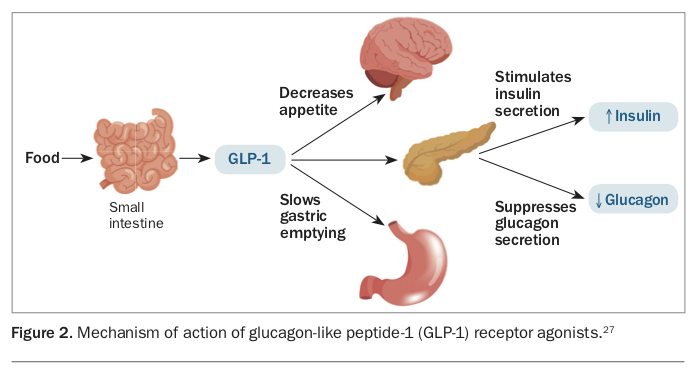
The GLP-1 receptor is present in the brain, neurons of the stomach and beta cells of the pancreas, as well as the heart, kidneys and possibly blood vessels. Activation of the GLP-1 receptor decreases appetite and improves satiety, slows gastric emptying, increases glucose-dependent insulin secretion and decreases glucose-dependent glucagon secretion (Figure 2).27 This results in a significant reduction in postprandial glucose levels, without the additional risk of hypoglycaemia when a GLP-1 receptor agonist is used as monotherapy or in combination with other glucose-lowering therapies that do not directly increase the risk of hypoglycaemia. GLP-1 receptor agonists have the additional benefit of weight reduction.28-30
{kind=link}
The GLP-1 receptor agonists available in Australia are dulaglutide, short-acting and modified-release exenatide and liraglutide.
Side effects
The most commonly reported adverse event with GLP-1 receptor agonists is gastrointestinal upset, which may settle over time with continued use. Gastrointestinal upset is more pronounced with the shorter-acting GLP-1 receptor agonist, liraglutide, compared with the longer-acting dulaglutide. Slight decreases in blood pressure and increases in heart rate have also been documented. A rare increased risk of acute pancreatitis and gall bladder pathology has also been reported, as well as a theoretical risk of medullary thyroid cancer.28,31-35
Trial evidence
The LEADER trial examined once-daily liraglutide in patients with established atherosclerotic CVD, chronic kidney disease, heart failure or significant cardiovascular risk factors.36 It showed a significant reduction in the composite endpoint of nonfatal myocardial infarction, nonfatal stroke and cardiovascular mortality, as well as all-cause mortality. Liraglutide also significantly reduced both the development and progression of chronic kidney disease.37
The REWIND trial examined once-weekly dulaglutide in a mixed population with and without established CVD.38 It showed a significant reduction in the primary composite endpoint of nonfatal myocardial infarction, nonfatal stroke and cardiovascular mortality, without a significant effect on all-cause mortality. In addition, there was a significant reduction in the renal arm of the composite microvascular outcome, involving new macroalbuminuria, sustained decline in estimated glomerular filtration rate or chronic renal replacement therapy.
The SUSTAIN trial examined once-weekly semaglutide (not available in Australia) in patients with established atherosclerotic CVD, chronic kidney disease, heart failure or significant cardiovascular risk factors.39 It showed a significant reduction in the primary composite endpoint of cardiovascular death, nonfatal myocardial infarction and nonfatal stroke, mainly driven by a reduction in stroke rate. Semaglutide significantly reduced both the development and progression of chronic kidney disease but was also associated with a significant increase in retinopathy complications.
The ELIXA trial examined once-daily lixisenatide (not available in Australia) in a population with a recent myocardial infarction or recent hospitalisation for unstable angina.40 Lixisenatide was noninferior to placebo but not significantly superior for the composite endpoint of cardiovascular death, myocardial infarction, stroke or hospitalisation for unstable angina.
The EXSCEL trial examined once-weekly exenatide in patients with or without a history of CVD.41 It also showed noninferiority compared with placebo, but the results did not reach significance for the primary composite endpoint of death from cardiovascular cause, nonfatal myocardial infarction and nonfatal stroke.
Prescribing tips
GLP-1 receptor agonists with proven cardiovascular benefit should be considered for use in patients with, or at risk of, atherosclerotic CVD with an HbA1c above the target level in whom weight loss would be of particular benefit. GLP-1 receptor agonists should be avoided in patients with significant gastrointestinal disturbances or a history of pancreatitis, medullary thyroid cancer or multiple endocrine neoplasia syndrome type 2.30,31,35
Dulaglutide is prescribed as a single weekly dose of 1.5 mg subcutaneously and does not require dose adjustment for renal impairment. It is not recommended in patients with a creatinine clearance less than 15 mL/min because of lack of evidence about its use in patients with end-stage kidney disease.42 Current PBS criteria require dulaglutide to be used in combination with metformin alone (where a sulfonylurea is contraindicated or not tolerated) or in triple therapy with metformin and a sulfonylurea, with an HbA1c greater than 7%.43
Exenatide can be prescribed either as a short-acting twice daily subcutaneous injection (5 mcg or 10 mcg dose) or a modified-release weekly dose of 2 mg. The short-acting dose should be administered within one hour before commencing a meal. Exenatide is contraindicated in people with a creatinine clearance less than 30 mL/min.44 PBS criteria require exenatide to be used in combination with metformin, a sulfonylurea or both or, in the case of the short-acting formulation, with insulin, with an HbA1c above 7%.45
Liraglutide should be commenced at a dose of 0.6 mg subcutaneously daily, which can then be increased after a week up to 1.2 mg daily if tolerated, and up to a maximum dose of 1.8 mg daily. Liraglutide does not require dose adjustment for renal impairment. It is not recommended in people with a creatinine clearance less than 15 mL/min because of lack of evidence about its use in patients with end-stage kidney disease.46 Liraglutide is not currently subsidised by the PBS and therefore incurs additional out-of-pocket expenses for patients but is not limited by PBS restrictions on combination prescribing.
GLP-1 receptor agonists are not subsidised for use as monotherapy or in combination with a DPP-4 inhibitor, thiazolidinedione, SGLT-2 inhibitor or insulin (except for short-acting exenatide which can be coprescribed with insulin).45
Conclusion
Individualising patient care is essential in the ongoing multifaceted management of diabetes. Newer therapeutic options such as the SGLT-2 inhibitors and GLP-1 receptor agonists can provide improved glycaemic control as well as additional cardiovascular, renal and mortality benefits in patients at risk of or with established CVD. They have the added advantages of weight loss, lower blood pressure and lower risk of hypoglycaemia. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.