Nocturnal enuresis in children. When to treat, when to refer

Child development
Nocturnal enuresis is common and has the potential to have a significant negative psychosocial impact on children. Most children with enuresis can be successfully treated by GPs. This article aims to assist GPs with the initial treatment of enuresis using sound principles of assessment and triaging.
Nocturnal enuresis (bedwetting) is common in school-aged children. It affects one in five children at 5 years of age and about one in 10 children at 10 years of age.1 Children with enuresis can have strong feelings of shame, guilt and failure, and a sense of being different to others. Often children with enuresis will avoid social activities. The negative impact seems to be greater in older children and in girls.2 In addition to the emotional costs, there are the financial costs to parents and/or carers, as well as time and effort in cleaning. One in seven children will spontaneously become dry every year and treatment should be offered to help others with significant enuresis achieving dryness sooner.
What causes bedwetting?
The three main physiological factors in enuresis are:
- defective sleep arousal
- nocturnal polyuria
- urinary bladder factors (e.g. lack of inhibition of bladder emptying during sleep, reduced bladder capacity or bladder overactivity).
The contribution and pathogenesis of these factors vary from child to child. Enuresis is more common in children with:
- a positive family history – large UK study found the odds ratios for severe nocturnal enuresis were 3.6 and 1.9 times higher if a mother or father, respectively, had a history of enuresis3
- sleep-disordered breathing – in children with enuresis and obstructive sleep apnoea from adenotonsillar hypertrophy, the enuresis resolves in up to half after appropriate treatment
- obesity
- attention deficit hyperactivity disorder (ADHD)
- autistic spectrum disorder
- developmental delay and physical or intellectual disability.
What type of enuresis is it?
The initial assessment of the child with nocturnal enuresis should determine:
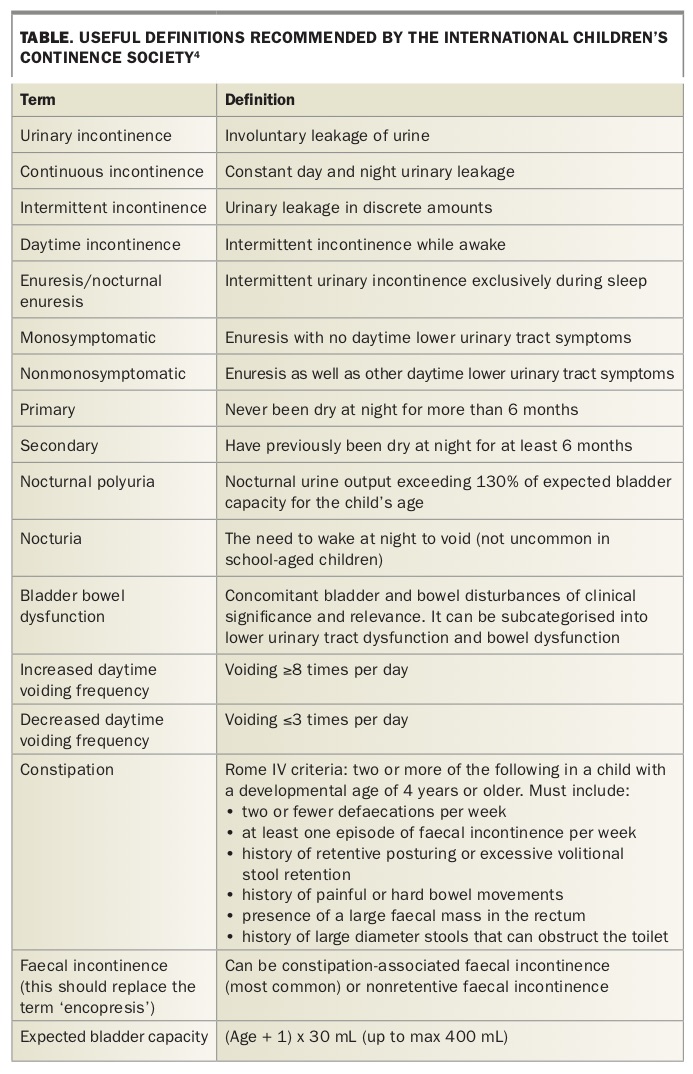
- if nocturnal enuresis is monosymptomatic (MNE) or nonmonosymptomatic (NMNE [for definitions see Table])4
- if it is primary or secondary
- the severity of enuresis and of any other symptoms.
{kind=link}
The Flowchart outlines how to classify the type and severity of nocturnal enuresis.1 Pathogenic differences exist between the different groups. For example, children with NMNE, secondary enuresis and more severe symptoms are less likely to respond to first-line treatment, are more complicated to manage and take longer to achieve dryness.
Clinical assessment
It is important to allow sufficient time for a thorough assessment and to formulate a plan with the child and parents.
History
- Family history of enuresis or urinary incontinence.
- Daytime urinary symptoms, such as:
— frequency and severity of wetting
— urgency
— voiding frequency more than eight times a day
— dysuria or pain
— holding manoeuvres. - Bowel history. Enuresis is often associated with chronic constipation and faecal incontinence. In those with constipation and enuresis, enuresis has been shown to resolve in up to two-thirds of children after the constipation is successfully treated.5
- Fluid intake and diet. This may impact on bladder function (fluid restriction may reduce the size of the bladder, and fluid loading in the evening may increase the risk of bedwetting) and constipation.
- Sleep history. Children with enuresis are more difficult to arouse than their peers, have more fragmented sleep and have higher levels of daytime sleepiness. There is also a higher prevalence of sleep-disordered breathing and the child may need assessment for adenotonsillar hypertrophy.
- General health, including developmental delay, ADHD, oppositional defiant disorder and other mental health history. Enuresis may be a symptom of an undiagnosed medical condition such as diabetes or kidney disease. The presence of ADHD, autistic spectrum disorder or other physical, psychological or behavioural disabilities can complicate management and signal the need for greater input and support.
- Home, school and family situation. This may clarify the impact of the enuresis on the child and influence the choice of treatments.
Physical examination
- An abdominal examination.
- A brief neurological examination, including deep tendon reflexes, anal reflex, lower limb tone and examination of the back for signs of spinal lesions.
- An examination of the perineum and genitalia.
Investigations
- Urinalysis with or without urine culture.
- Bladder diary (frequency and volume chart, which can be downloaded online at: www.neresourcekit.com.au). A bladder diary for 48 hours provides objective data and helps to detect children with NMNE and those needing further evaluation. Practitioners should look for abnormalities in amount and distribution of fluid intake, daytime frequency, daytime leakage, severe urgency and nocturnal urine production.
- Renal ultrasound and postvoid residual assessment. A renal and bladder ultrasound is only indicated in cases of refractory enuresis or NMNE. Noninvasive uroflowmetry and postvoid residual assessment are available in some specialised bladder and continence clinics, which provide additional information for children with treatment resistance and/or those with severe associated daytime urinary symptoms.
When to refer early
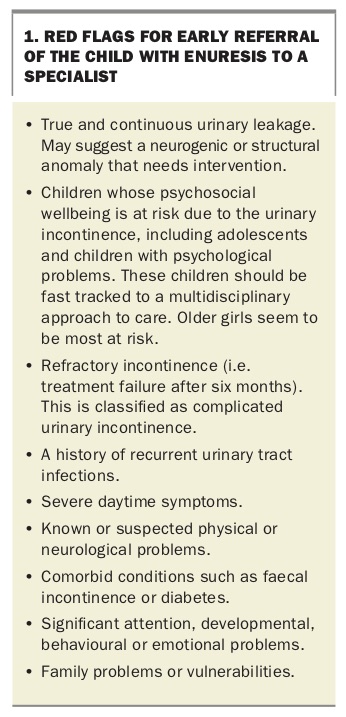
Some children with nocturnal enuresis will require referral to, and management by, a specialist urologist and/or a multidisciplinary team, and some cases should be fast tracked. Indications for early referral are listed in Box 1.
{kind=link}
Initial management
Initial management of enuresis consists of conservative measures aimed at rehabilitation of the lower urinary tract and bowel function (i.e. standard urotherapy).4,6,7 This includes the following:
- Provide information and demystification. Explain about normal function and differences in the child’s condition.
- Give instructions in establishing optimal micturition. Explain about the importance of regular voiding, proper voiding posture, avoidance of voiding postponement and regular bowel habits. Encourage regular voiding during the day and void before bed. Voiding postponement may reduce the child’s awareness of bladder sensations and their need to void. Encourage or teach relaxed voiding to optimise bladder emptying and storage.
- Establish guidelines for diet and fluid intake. Ensure patient is drinking adequately for optimal bladder function (fluid restriction may reduce the size of the bladder and fluid loading in the evening may increase the risk of bedwetting) and avoiding caffeinated drinks.
- Document symptoms and voiding habits. Use bladder diaries, frequency and volume charts and/or mobile apps.
- Ensure normal bowel habits. Treat constipation and ensure daily bowel movements passing normal consistency stools without straining. Note that some children with NMNE have remission of daytime symptoms when bowel problems are resolved.
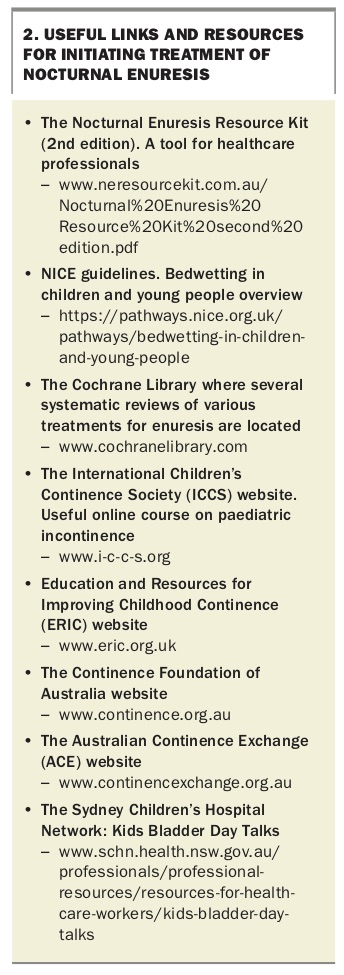
- Support and encouragement. Ensure regular follow up with the caregiver and treating team. Information sheets and other useful tools can be downloaded from www.neresourcekit.com.au (see Box 2).
{kind=link}
Managing children with monosymptomatic enuresis
For young children who are not bothered by the enuresis, active treatment may not be warranted. Spontaneous resolution rate of MNE is 15% per year.1 For younger children, star charts and rewards may help by providing incentives for rewarding the child for doing the right thing (such as drinking more during the day, reducing bedtime drinks and getting out of bed to void if they wake at night).7
Managing children with nonmonosymptomatic enuresis
In children with NMNE, treatment should target bladder function first as it can impact on both daytime and night-time wetting.6 Once these symptoms are resolved, it is easier to address the enuresis.
Treatment
Alarm training
Enuresis alarms train the child to wake to void when their bladder is full and hold on when they do not need to void during the night. The enuresis alarm detects when the child wets and emits a noise or vibration, alerting that the child has wet. When the alarm sounds, the child needs to wake and try and void in the toilet (even if they do not feel they need to void). Often children do not wake to the sound of the alarm (even if the rest of the family does). Parents need to wake the child if the child is unable to wake themselves. Alarm training takes two to three months. The child should continue alarm therapy until they have had 14 consecutive dry nights.
If relapse occurs, repeating alarm training will often produce a good response. For further tips, refer to the following website: www.neresourcekit.com.au. Alarm therapy needs commitment from both the child and family, as well as assistance from supportive and knowledgeable healthcare professionals.
Desmopressin
Desmopressin is an antidiuretic, a synthetic analogue of the hormone vasopressin. Use of desmopressin in children with enuresis reduces overnight urine production; however, recent studies have pointed to an additional effect on the arousal mechanisms.8 About 70% of children with MNE will have a response to desmopressin, about 30% will be full responders and a further 40% will have a partial response with a reduction in the number of wet nights per week.1 A Cochrane review of desmopressin for enuresis concluded that desmopressin rapidly reduced the number of wet nights per week, but the effect was not sustained after treatment stopped in most cases.9
Desmopressin is usually well tolerated, with adverse effects such as headaches, abdominal pain and emotional disturbance being uncommon. The most serious adverse effect reported for desmopressin is hyponatraemia, therefore, fluids should be restricted from one hour before medication until eight hours after. It is useful for short-term use, such as sleepovers or camps, or when alarm training is difficult or contraindicated (e.g. when family are not supportive).
Desmopressin is available on the PBS (authority required; streamlined) for primary nocturnal enuresis in patients 6 years of age or older who are refractory to an enuresis alarm or in whom an enuresis alarm is contraindicated. Desmopressin is available in the following formulations:
- sublingual wafer (melts), containing 60 mcg, 120 mcg or 240 mcg desmopressin
- tablet, containing 200 mcg desmopressin
- nasal spray, containing 10 mcg per actuation desmopressin. However, the nasal spray is not recommended because of a higher risk of adverse effects.
Melts are often used in primary school-aged children because they are easy to take compared with tablets and are preferred by children under 12 years of age, which may enhance adherence.9,10 Although food interaction influences the bioavailability of desmopressin, melts have a smaller variance in plasma concentration with low food interaction, which may make the melts more suitable for younger children who may have a short interval between the evening meal and bedtime.11,12 Furthermore, no water is needed to take the melt, so it is easier to comply with restriction of fluid intake.
The recommended dosage for children with enuresis is 200 to 400 mcg daily (for tablets) and 120 to 240 mcg daily (for melts) taken about one hour before bedtime. Fluid intake must be limited (no more than one cup of water) from one hour before until eight hours after administration.
Relapse commonly occurs when desmopressin is ceased. However, structured withdrawal of desmopressin results in better relapse-free rates compared with abrupt withdrawal of desmopressin.13
Desmopressin versus alarm therapy
A Cochrane review comparing alarm and desmopressin therapies found that although at cessation of therapy there were generally no differences between the two in the short term, alarm therapy was more effective than desmopressin in the long term.10 Some studies report a higher initial attrition rate in families and children who use alarm therapy compared with those taking desmopressin.14
Summary
Nocturnal enuresis should be treated in children who show no signs of spontaneous resolution (by the time the child reaches primary school) and in those who report negative psychosocial impact. The type of enuresis (monosymptomatic or nonmonosymptomatic) should guide initial therapy. Children with suspected underlying urological or neurological causes or inadequate response after six months of treatment should be referred to a specialist. Bedwetting alarms and desmopressin (tablets or melts) are effective treatment options in appropriately selected patients and when offered in conjunction with successful urotherapy. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.