Anaphylaxis – an allergic emergency

Anaphylaxis
Allergy
Anaphylaxis can occur as a result of an allergy to food, insect venom or medication. Affected patients should be educated about how to reduce their risk of accidental exposure to their specific allergen, how to use an adrenaline autoinjector and the importance of always carrying their adrenaline autoinjector and ASCIA action plan.
- The major causes of anaphylaxis are allergy to food, insect bites or stings, and medication, most often NSAIDs and antibiotics.
- Anaphylaxis diagnosis and treatment are often delayed, and misdiagnosis as acute asthma has led to fatalities.
- The major risk factors for fatal anaphylaxis are failure to recognise early symptoms, poorly controlled asthma, delayed or absent adrenaline (epinephrine) use and assumption of an upright posture.
- The cornerstones of acute management are supine positioning of the patient; administration of intramuscular adrenaline (epinephrine) and intravenous saline, airway support and oxygen; and observation for four hours after symptom resolution.
- Patients who experience anaphylaxis should be referred to a clinical immunology or allergy specialist for further investigation and treatment.
- The mainstays of long-term management are patient education to avoid accidental allergen exposure; teaching about recognition of early symptoms; advice to seek early medical attention if needed and to carry and be trained in the use of an adrenaline autoinjector; and provision of an ASCIA action plan.
Anaphylaxis has become an increasing public health burden in developed countries over the past decade, contributing to increased demand for specialty services, significant economic cost of care and reduced quality of life for patients and their families.1-3 Australia reportedly has higher rates of food allergy and fatal anaphylaxis than other westernised countries.4 Anaphylaxis diagnosis and treatment are often delayed, and misdiagnosis as acute asthma has led to fatalities.4
Effective strategies for primary prevention of anaphylaxis are emerging, such as early allergenic food introduction.5 Secondary prevention is limited to strategies to reduce the risk of unintentional allergen exposure, except for insect venom anaphylaxis for which specific immunotherapy is available. Immunotherapy for food allergy remains at the investigational stage in Australia because of relatively high rates of adverse reactions.6
What is anaphylaxis?
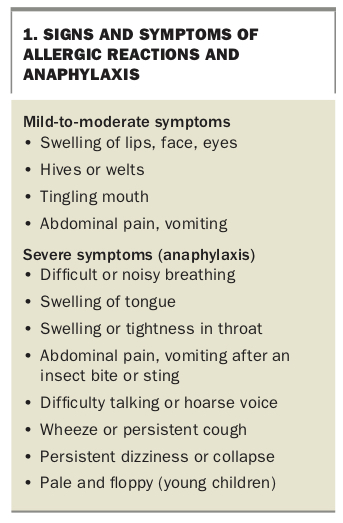
Anaphylaxis is a rapidly developing multisystem allergic reaction that may result in death.7 Symptoms and signs arise from the massive release of mediators from mast cells and basophils by mechanisms that are immunoglobulin (Ig) E-dependent (most cases) or independent (some cases). Although flushing or rash is usually present, anaphylaxis should be considered in the differential diagnosis for patients presenting with acute hypotension, bronchospasm or severe upper airway obstruction, even when rash is absent. Respiratory symptoms are more common in children, especially when triggered by food allergy, whereas cardiovascular symptoms dominate in adults, especially when triggered by medication or insect venom.8 An overwhelming sense of impending doom is not uncommon.9
In intraoperative anaphylaxis, cardiovascular collapse may be the only presenting sign.10 Importantly, abdominal pain and vomiting are symptoms of anaphylaxis in patients with insect venom reactions, correlating with hypotension (Box 1).
{kind=link}
Pathophysiology
The essential underlying mechanism of anaphylaxis is mast-cell and basophil activation with release of various mediators, with resultant vasodilation, fluid extravasation and bronchial and gastrointestinal smooth muscle contraction. Death may occur from hypoxaemia due to upper airway angioedema, bronchospasm and mucus plugging, or shock due to massive vasodilation, fluid shift into the extravascular space and depressed cardiac function. This range of effects underscores the importance of physiological antagonism with adrenaline (epinephrine) and fluid resuscitation, rather than antagonism of a single mediator such as histamine.11
Common causes of anaphylaxis
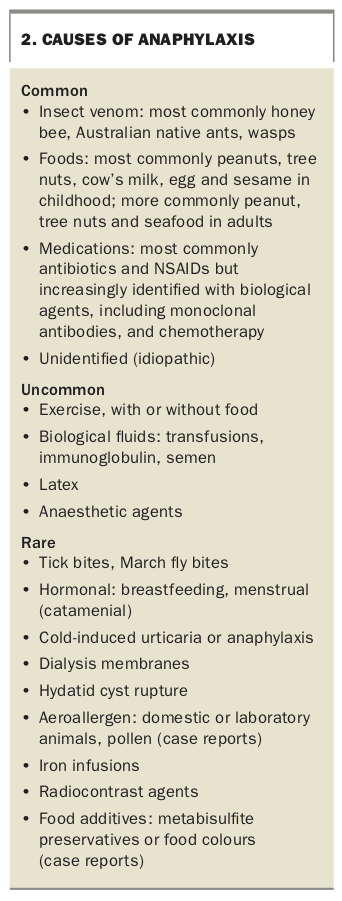
Food, insect venom or medication trigger most cases of anaphylaxis, with a variable proportion of patients having less common causes, such as exercise-induced anaphylaxis (Box 2). Idiopathic anaphylaxis is diagnosed when extensive evaluation fails to identify the underlying cause. In hospital emergency settings, food allergy is responsible for about 80% of paediatric anaphylaxis presentations when the cause has been identified, whereas in adults, food is initially identified as the cause in only 20 to 30% of presentations.8,11 This finding reinforces the need for all patients with anaphylaxis to be referred to an allergy specialist and to be assessed.
{kind=link}
Anaphylaxis is increasing
Hospital admission rates for anaphylaxis are higher in Australia than in other westernised countries. In the financial year 2011 to 2012, total and food-related anaphylaxis rates were 17.7 and 8.2 per 100,000 of the overall population, respectively, with the highest rates being in young children aged 0 to 4 years, at 35.1 and 30.3 per 100,000, respectively.12 These rates are almost certainly underestimates, as they exclude people treated in the community or in emergency departments but not admitted, or cases where medical assistance was not sought. An estimated 2 to 3% of adults have experienced anaphylaxis after stings from honey bees or native Myrmecia ant species (in areas where these are prevalent).13 There is also evidence that food allergy and anaphylaxis have increased over the past decade in westernised countries.14
Risk factors for developing food allergy include atopic eczema, delayed introduction of allergenic food, Asian genetic background and, perhaps, low vitamin D levels in the first year of life (evidence is conflicting).15
Fatal anaphylaxis
Deaths from anaphylaxis are likely to be underestimated because of the difficulty of postmortem diagnosis (there are no pathognomonic features), miscoding of anaphylaxis deaths as due to asthma and lack of mandatory reporting to the coroner. Anaphylaxis is considered to be ‘death from natural causes’ in Australia.
Drug and insect allergies are reported as being the most common causes of fatal anaphylaxis in Australia. This may be because most drug-related anaphylaxis deaths occur in medical facilities, leading to higher rates of reporting.
Most food-related anaphylaxis deaths in children and young adults in Australia are due to peanuts, tree nuts and cow’s milk, whereas in older individuals seafood is the major trigger.4 Further, most food-related fatalities occur in young adults. This may reflect in part the epidemiology of food allergy in the population (it is most common in children who have higher rates of comorbid asthma) and also perhaps other risk factors, such as eating away from home in teenagers and young adults.4 By contrast, most fatal cases of anaphylaxis to insect venom and medication occur at the median ages of 55 and 67 years, respectively, reflecting greater cardiovascular comorbidity in older age groups that increases the risk of fatal anaphylaxis.16
Major risk factors for fatal anaphylaxis are:
- past severe reactions
- poorly controlled asthma
- delayed (or no) administration of adrenaline
- assumption of the upright posture, including while being driven to hospital.4,16
Many patients with anaphylaxis in Australia have been incorrectly treated for asthma first, leading to delayed adrenaline administration. As a result, the Australasian Society of Clinical Immunology and Allergy (ASCIA) has incorporated specific wording in its action plan for anaphylaxis first aid, including advice to administer adrenaline first and bronchodilators second when the diagnosis is uncertain.17
Cofactors
Cofactors can be important in aggravating the severity of an allergic reaction or may be required before an allergen will provoke a reaction, the most common being exercise. Intercurrent infection, concomitant medication (particularly beta blockers and NSAIDs), alcohol, spicy food and high ambient temperatures have also been associated with an increased risk of anaphylaxis. This phenomenon may account for some cases of intermittent anaphylaxis where a cause has not been established.
Exercise-induced anaphylaxis affects predominantly young adults. Although some people experience symptoms with exercise alone, most are allergic to a food ingested within the previous four hours. Wheat, celery, seafood, nuts, fruits or vegetables are most commonly associated with food-related, exercise-induced anaphylaxis.18 Whether an episode occurs may be determined by the amount of food ingested, the intensity of exercise and the time between the two, as well as other cofactors listed above. Although most episodes occur during exercise after food ingestion, some may occur when the order is reversed.
Differential diagnosis
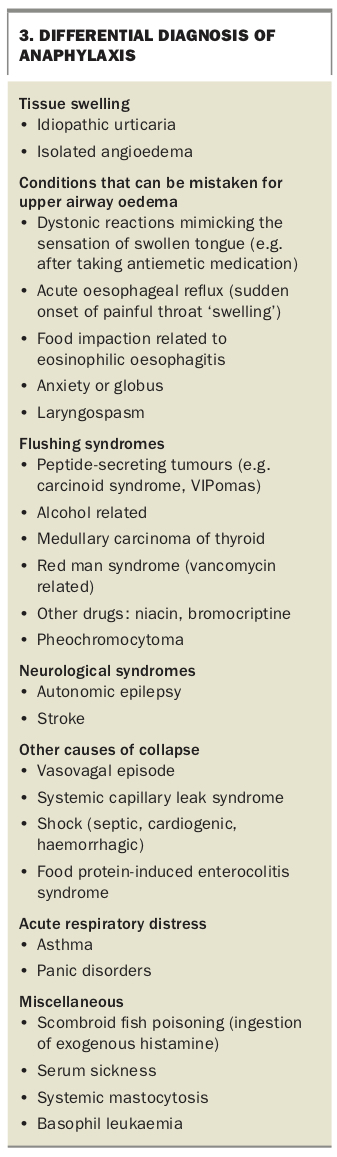
The differential diagnoses depend on the mode of presentation. The many causes of hypotension should be considered in patients with shock (Box 3). The most common mimicking conditions for anaphylaxis are urticaria and angioedema. Importantly, when urticaria or angioedema last for days at a time, an allergic origin (with the possible exception of drug allergy) is unlikely, even when symptoms are severe.
{kind=link}
Acute management of anaphylaxis
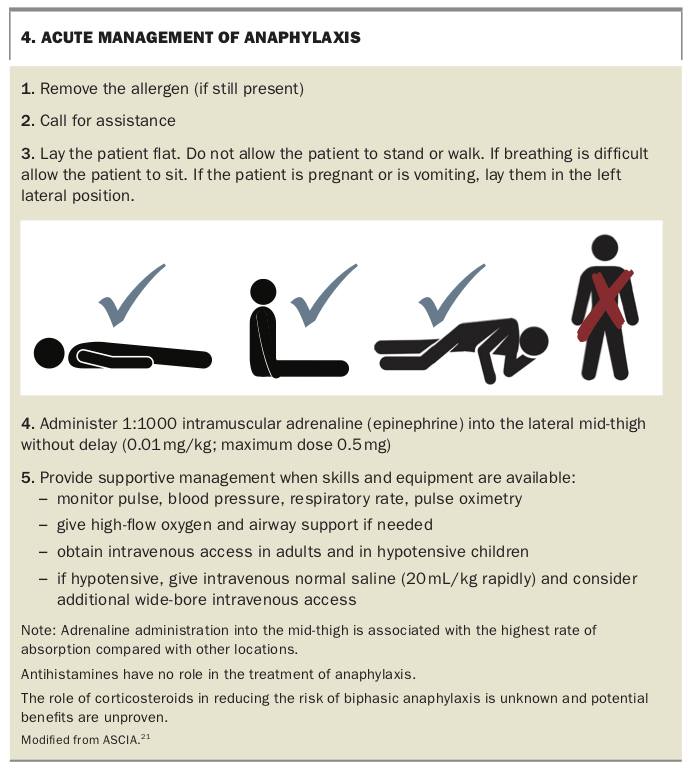
The cornerstones of acute management of anaphylaxis are:
- positioning the patient in the supine position (or left lateral position for patients who are vomiting or pregnant)
- intramuscular injection of adrenaline (epinephrine) into the lateral mid-thigh (1mg/mL [1:1000] solution at a dose of 0.01mg/kg with a maximum dose of 0.5 mg [0.5mL])
- intravenous fluid resuscitation with saline at 20mL/kg (repeated up to a total 50mL/kg over the first half hour)
- support of the airway and ventilation
- supplementary oxygen (Box 4).19-21
{kind=link}
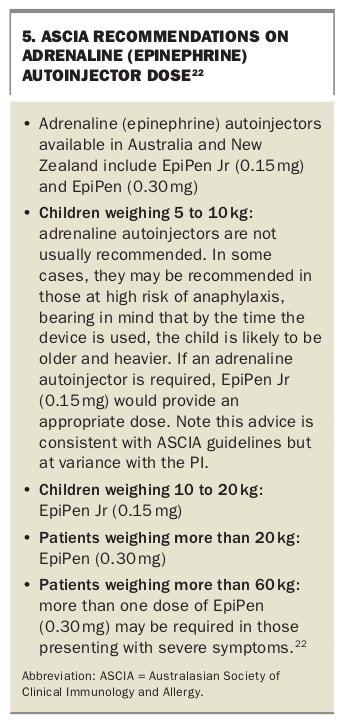
The appropriate dose of an adrenaline (epinephrine) autoinjector (if available) can be used instead of an intramuscular injection of adrenaline (Box 5).22
{kind=link}
Adrenaline acts to reduce airway mucosal oedema, induce bronchodilation and vasoconstriction, and increase the strength of cardiac contraction, thus increasing heart rate and blood pressure. As the effects of adrenaline last about 15 to 20 minutes, repeated doses may be required, and can be given after five minutes if the first dose is ineffective.
As acute asthma and acute anaphylaxis can have similar presentations, the current recommendation (reflected in the ASCIA anaphylaxis action plans) is that if there is uncertainty whether the diagnosis is asthma or anaphylaxis, adrenaline should be administered first and bronchodilators second.17
The supine position helps to maximise venous return in patients with hypotension. In pregnant women, the left lateral position is recommended to reduce the risk of compression of the inferior vena cava by the pregnant uterus and impairment of venous return to the heart.
Glucagon may be helpful in patients who have pre-existing heart failure or are taking beta blockers, as glycagon is inotropic independent of beta receptors and can stimulate endogenous catecholamine release.23 Other medications such as antihistamines, H2-blockers, corticosteroids and antileukotrienes have no proven impact on the immediate and life-threatening effects of anaphylaxis, although they may ameliorate mild allergic reactions confined to the skin.19 The only registered antihistamine for parenteral use in Australia (promethazine) can worsen vasodilation and hypotension and cause muscle necrosis if injected intramuscularly, and its use in anaphylaxis is not advised.21,24,25
A wallchart showing the emergency management of anaphylaxis is available to download and is recommended for reference in medical facilities (www.nps.org.au/australian-prescriber/articles/anaphylaxis-emergency-management-for-health-professionals).20
Anaphylaxis in infants: special considerations
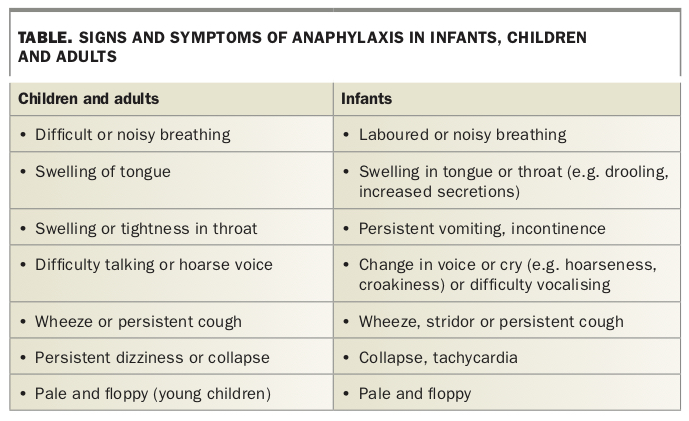
Delayed introduction of allergenic food is associated with greater risk of food allergy development, particularly in infants at high risk (those with severe eczema, egg allergy or both). This has led to advice to introduce allergenic foods in the first 12 months of life to reduce the risk (ASCIA guidelines for infant feeding).26 The National Allergy Strategy recently released a website to encourage parents to introduce the common food allergens (www.preventallergies.org).27 In rare cases, anaphylaxis may occur in infants who are nonverbal and may present with subtle signs and symptoms (Table).28
{kind=link}
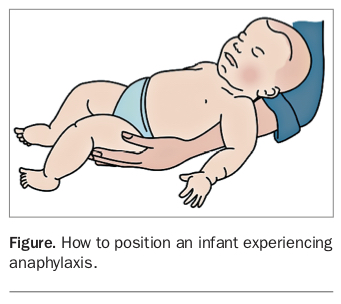
As in adults, it is important that an infant with anaphylaxis is not held upright as this increases the risk of vascular collapse. The correct positioning for an infant experiencing anaphylaxis is shown in the Figure.
{kind=link}
The main differential diagnosis of infant anaphylaxis presenting with cardiovascular collapse is food protein-induced enterocolitis syndrome (FPIES). Infants with FPIES may present with severe vomiting, pallor and limpness two to four hours after ingestion of allergenic food, most commonly rice, dairy or soy in Australia.29 Other conditions in the differential diagnosis include:
- acute urticaria (common in infants)
- causes of respiratory distress (e.g. foreign body, infection)
- causes of acute gastrointestinal symptoms (e.g. pyloric stenosis, intussusception, infective gastroenteritis)
- causes of central nervous system symptoms and signs (e.g. seizure, head trauma, meningitis)
- causes of syncope (arrhythmia, breath holding).
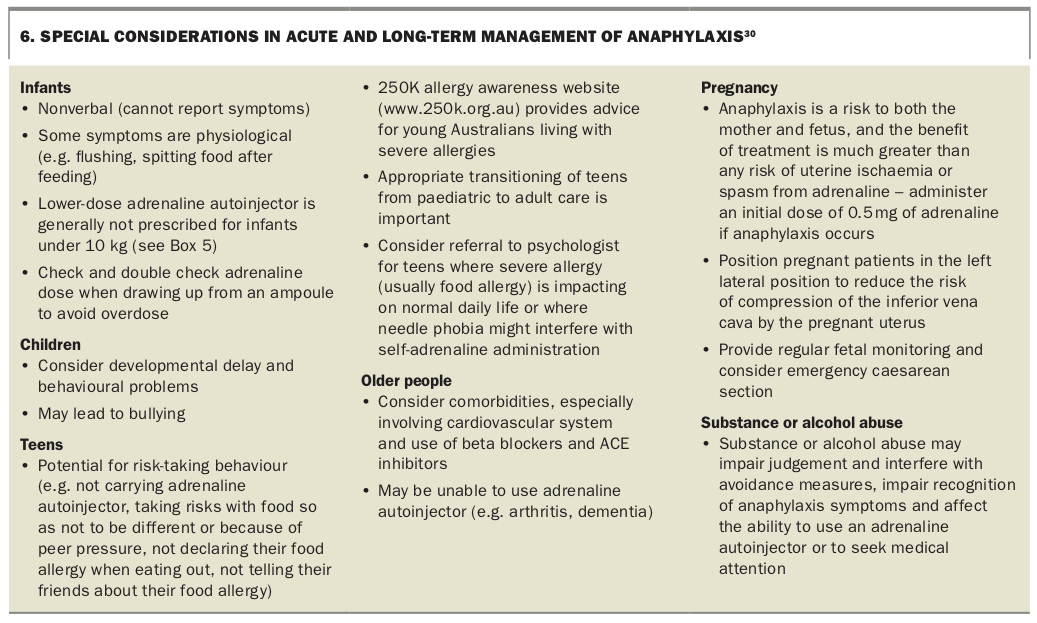
Special considerations in the acute and long-term management of anaphylaxis in infants, as well as in other groups, are listed in Box 6.30
{kind=link}
Observation after anaphylaxis
An observation period of four hours after symptom resolution is recommended for all patients, as symptoms may fail to improve or may worsen as the effect of adrenaline wears off (protracted anaphylaxis), may return after early resolution (biphasic reactions) or may recur as more food allergen is absorbed.
More prolonged observation may be required in those with severe or refractory symptoms or in those with asthma, as most fatalities associated with anaphylaxis occur in these groups. Other factors to consider include time of presentation or location of residence (e.g. city versus remote location).
Identification of the cause
It is important first to determine whether the patient has experienced anaphylaxis, before examining the surrounding circumstances to identify a cause. Although not satisfying the definition of anaphylaxis, rare and short-lived bouts of urticaria and/or angioedema lasting less than 12 hours should prompt suspicion of an allergic cause, whereas ongoing symptoms lasting for days are unlikely to have an allergic origin.
Exposure to potential triggers (e.g. food, medication, insect venom or occupational allergens such as latex) and cofactors in the preceding eight hours should be recorded while the patient’s or carer’s memory of the event is fresh. ASCIA has developed an event record template for patients to complete, which can be downloaded (https://allergy.org.au/hp/anaphylaxis/anaphylaxis-event-record).31
Almost all anaphylactic reactions to insect venom or food/medication occur within one and six hours, respectively. The presence of known food or drug hypersensitivity should be recorded and the possibility of accidental exposure considered. When insect bites or stings have occurred, the insect appearance and the presence of a stinger left in the skin (which indicates honey bee sting) may help identify the cause.
Investigations
Anaphylaxis remains a clinical diagnosis. Mast-cell tryptase is an insensitive biomarker for anaphylaxis, although serial determinations (e.g. on arrival, one hour later and before discharge) may improve the sensitivity and specificity of the test.2,32 Importantly, tryptase levels are more likely to be elevated in those with severe drug or insect allergy than in those with food allergy. An elevated tryptase level may help when the diagnosis is uncertain (highest levels observed with drug and venom anaphylaxis), but a normal result does not exclude anaphylaxis, especially when triggered by food.
Skin allergy testing to assess sensitisation to food, medications and insect venom carries a small risk of inducing anaphylaxis. It should only be carried out by trained personnel in an environment where anaphylaxis can be treated.
In vitro testing for allergen-specific IgE is a useful initial test when a trigger is strongly suspected (e.g. in an infant with anaphylaxis after peanut exposure). Measurement of total IgE levels provides no useful information and is discouraged. In vitro testing using food mixes often provides misleading or irrelevant results and should not be requested (e.g. a negative nut mix result may provide false reassurance when the trigger is cashew, as cashew-specific IgE is not measured by a nut mix test).
Oral food challenges can also help to identify the allergen and to confirm whether the patient has outgrown their allergy. However, as there is a potential risk of anaphylaxis, the decision whether to perform an oral challenge (and location of the challenge) should only be made by clinical immunology or allergy specialists.
There is currently no test to confirm tick-bite allergy, although anti-alpha-galactose IgE has been observed in most patients with tick bite allergy.33 Following an insect bite or sting reaction where the causative insect cannot be identified, it is appropriate to test for honey bee, jack jumper ant, paper wasp (Polistes spp.), European wasp/yellow jacket and fire ant (in parts of Queensland where it is endemic). When the causative insect is uncertain, allergen-specific component venom testing may provide more specific information, and specialist advice should be obtained on which tests to request.34 Measurement of blood tryptase levels at the same time is also useful, as baseline elevation may indicate the presence of systemic mastocytosis, which can increase the risk and severity of venom anaphylaxis. Skin testing for jumper-ant allergy is not available outside research programs in Tasmania, but blood allergy testing is available from the Institute of Medical and Veterinary Science (IMVS), Adelaide, South Australia. This detects only 80% of cases, and although the subject of ongoing research, there is no validated test to detect allergy to related ant species.
Some drug reactions (e.g. to NSAIDs or radiographic contrast agents) are usually independent of IgE, and there are numerous difficulties in assessing many cases of antibiotic allergy owing to lack of suitable reagents for testing (except for the penicillin group). Medically supervised challenges are sometimes required to prove or disprove allergy.
There is no scientific validity for ‘alternative’ tests (e.g. cytotoxic or Vega testing, hair analysis, kinesiology) and their use should be discouraged.35
When to refer
Specialist evaluation of patients is recommended after a diagnosis of possible anaphylaxis to:
- identify or confirm the cause
- educate patients on appropriate allergen avoidance strategies
- assist in drafting an emergency action plan (e.g. using the ASCIA action plan), including adrenaline autoinjector provision
- advise whether immunotherapy is available and clinically appropriate.
All of these factors have been associated with less severe episodes of subsequent anaphylaxis.36
Long-term management and prevention
Anaphylaxis to insect bites or stings can be prevented with venom immunotherapy, which reduces the risk of anaphylaxis from repeated bites or stings, and is associated with an improved quality of life compared with carrying an adrenaline autoinjector alone.37 Attempts to modify the severity of food allergy using similar techniques have shown early promise but remain in the investigational stage in Australia owing to high rates of side effects, even in patients on maintenance doses.6 Protocols exist to provide desensitisation to medications, but these provide only temporary protection to allow for a window of therapeutic use, and the allergy returns on treatment cessation.
The mainstays of management are:
- patient education to reduce the risk of accidental exposure
- patient education on recognising early symptoms
- advice to seek early medical attention if these occur
- advice to carry and be trained in the use of self-injectable adrenaline
- provision of an emergency action plan.
Several resources, including ASCIA action plans (e.g. the emergency action plan), travel plan and diet sheets can also be downloaded from the ASCIA website (www.allergy.org.au/hp/anaphylaxis).17,38,39 A medical bracelet may provide additional information to attending medical and paramedical personnel about known allergies, reduce the risk of administration of allergenic medication and facilitate earlier recognition of anaphylaxis and treatment. An allergy alert should also be entered in medical records to reduce the risk of inadvertent exposure to allergenic medication or food, including in patients admitted to hospital.
Annual GP review is recommended to:
- re-educate patients on the use of adrenaline autoinjectors
- ensure that the device is renewed at appropriate intervals
- provide updated ASCIA action plans
- provide psychological support
- provide specialist referral for review.
Adrenaline (epinephrine) autoinjectors
Patients diagnosed at risk of anaphylaxis may be prescribed an adrenaline (epinephrine) autoinjector (e.g. EpiPen). The autoinjector may be obtained over the counter at full cost or on a PBS authority prescription by patients considered at high risk of severe allergic reactions. Initial PBS prescription must be provided in consultation with an allergy or immunology specialist, paediatrician, emergency specialist or respiratory physician (which can be by telephone in the first instance). Up to two devices may be provided with PBS subsidy; additional devices (if desired) need to be purchased privately. The ASCIA guidelines for adrenaline autoinjector prescription and instructions on its use are available from the ASCIA website (www.allergy.org.au/hp/anaphylaxis/adrenaline-autoinjector-prescription).22
It is essential that patients and carers are educated in both the recognition and management of allergic reactions. They should be shown how to use their prescribed adrenaline autoinjector using a trainer device and given advice on allergen avoidance measures. They should also be educated about the need to always carry the adrenaline autoinjector and their ASCIA action plan for anaphylaxis.
Where to store adrenaline
Adrenaline autoinjectors should not be exposed to extremes of heat (to protect the adrenaline) and should not be stored in the refrigerator or freezer as this can damage the autoinjector mechanism, causing it to jam. Room temperature is optimal. Regardless of location, everyone who might need to give adrenaline should know where it is located. At school, adrenaline should be stored in an unlocked location, known and easily accessible to staff. Pouches designed to keep the adrenaline autoinjector at the correct temperature for an extended period when in the heat (e.g. at the beach, during outdoor sporting activities, camping) are available for patients to purchase (https://allergyfacts.org.au/shop).
Although expiry dates are included in the product label of each device, it is important to be aware that even expired devices contain significant amounts of active adrenaline. Thus, if an in-date device is not available, it is better to administer an expired device than to withhold treatment in a patient experiencing anaphylaxis.
Dose of adrenaline autoinjectors
The adrenaline doses often recommended by specialist bodies such as ASCIA (Box 5) are based on consensus of expert opinion and often differ from the product information leaflet.22
Travelling with food allergy
Patients should contact their airline to determine its policies regarding food allergy well in advance of travel and before booking and paying for tickets. All necessary documents, letters and medicines should be prepared in advance of travel. An ASCIA travel plan can be completed by the patient’s GP to authorise them to carry their adrenaline autoinjector and food on the plane.38 They should ensure their adrenaline autoinjector is in date. Patients should also check that their travel insurance covers their allergy. Commercially available illustrated travel cards in different languages are available to use when travelling to communicate about food allergy (e.g. www.selectwisely.com).
Although adverse reactions to airborne allergens have been described while flying, the major risk remains oral ingestion of allergenic food.40
Online resources
ASCIA regularly reviews its online resources and also provides free online e-training on food allergy and anaphylaxis for healthcare professionals, which can be completed as part of continuing education programs (https://etraininghp.ascia.org.au/). Allergy and Anaphylaxis Australia also maintains resources of use to patients and their carers (https://allergyfacts.org.au). Recently, the National Allergy Strategy has developed several websites and useful resources for healthcare professionals and patients (www.nationalallergystrategy.org.au).
Conclusion
Anaphylaxis is an increasingly common condition in Australia requiring prompt, accurate recognition and appropriate management. Managing comorbidities and cofactors is important in potentially reducing the risk of fatal anaphylaxis. Although immunotherapy options exist for some insect allergies, daily management relies on prevention strategies to reduce the risk of unintentional allergen exposure. It is essential to educate patients about how to reduce their risk of accidental exposure to their allergen, how to use the adrenaline autoinjector and the importance of always having their adrenaline autoinjector and ASCIA action plan with them. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.