Managing children and consent

Medicolegal medicine
Children's health
This series highlights common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, the scenarios are based on a range of previous cases with details changed for privacy and some issues summarised for discussion. In this scenario, a 15-year-old girl presents without her parents to ask for an antidepressant prescription, raising the question of children’s capacity to consent to treatment.
For many GPs, a great reward of practice is the opportunity to build long-term relationships with patients and their families. However, this can also present a particular challenge, as this scenario illustrates. As children mature and become capable of making decisions, so the law recognises that they develop legal capacity to make healthcare decisions independently of their parents. However, this is not necessarily a clear, or linear, progression. Although a child may be competent to make some medical decisions, this does not mean they have the capacity to make all medical decisions independently. Further, growing independence can put children in conflict with their parents, and navigating this complex terrain can be a challenge for doctors.
Case scenario
Presentation
Late one afternoon, Dr White’s next patient is Clara, a 15-year-old local school student. Clara has come in with her mother in the past but is here on her own today. After Dr White greets her, Clara says she has come to see her as she wants to be prescribed antidepressants.
‘My friend’s doctor has prescribed them for her’, she explains. ‘And she’s so happy now. It’s like she’s a whole new person! I just think that’s what life is meant to be like, but it’s not how I feel.’
Dr White is initially hesitant but asks some detailed questions and explores Clara’s medical and family history. Clara says that she has been struggling since her parents split up and wonders whether she is permanently damaged because of it. She describes feeling ‘worthless’ and ‘useless’, and thinking that nothing is ever going to get better. She has difficulty sleeping and has stopped attending the hip-hop dance class she loved in the past because she has no energy. She admits to dark thoughts and occasionally contemplating self-harm.
Management
Dr White is concerned and feels that maybe Clara could benefit from psychological therapy and referral to a psychiatrist for an opinion on antidepressant use. However, as a first step Dr White wants to be assured that Clara is able to provide adequate consent to the treatment plan. Dr White recognises that some minors have sufficient maturity to make their own decisions and considers Clara to fall in this category. She has met Clara several times. On each occasion, Clara has presented as a mature and responsible individual, capable of understanding and appreciating information she has been given. Dr White asks some very specific questions to ascertain whether Clara has understood the discussion about depression and medication and records them in the clinical file.
Still wary about prescribing antidepressants to a teenager, Dr White advises Clara it would be in her best interests to attend sessions with a psychologist and to consult a psychiatrist who could make the decision to start an antidepressant. She asks whether she can discuss the treatment plan with Clara’s parents. At first, Clara is distressed and absolutely forbids Dr White to mention this to her parents. This is a bit troubling for Dr White, so she engages Clara in a discussion about the benefits of having the advice and support of at least one parent. Eventually, Clara agrees that she will tell her mother and gives Dr White permission to discuss the plan with her.
Clara’s mother comes to see Dr White with Clara and together they agree that Clara will be referred to a local psychologist and a psychiatrist with a special interest in adolescent mental health. As the expected wait list for both services is longer than six weeks, Dr White advises Clara and her mother to return to see her in the interim for a review.
The complaint
Two days later, Dr White is between patients when the practice manager tells her that she has just had an angry phone call from someone identifying himself as the father of one of Dr White’s patients – a 15-year-old named Clara. He wanted to know what Dr White was doing referring his child to a psychiatrist and aggressively asserted that Dr White had no right to do so without his consent. The practice manager thinks he will probably make a complaint.
Dr White reviews Clara’s medical record as soon as possible. She confirms that she made good notes and fully documented her discussion with Clara about talking to the parents and her own assessment of Clara’s capacity. She diarises to contact her medical defence organisation early the next day to check whether there is anything else she should do.
Discussion
Informed consent
Before patients can undergo any examination, investigation, procedure or treatment, they must give their consent. However, urgent treatment may be provided when it is not possible to get consent and the treatment is required to save a person’s life or prevent serious harm to their health.
The informed consent process has three components:
- capacity
- voluntariness
- disclosure.
To provide valid consent to treatment decisions, a patient must have capacity. The law presumes that adults have capacity to make decisions about their health care. This presumption arises at 18 years of age in all Australian jurisdictions except South Australia, where the relevant age is 16 years. This means that for patients aged 18 years or older (16 years or older in South Australia), doctors can assume that the patient is capable of making a decision about their own health care unless there is any reason to doubt their capacity. However, the law also considers that children can in fact develop the capacity to make decisions about their health care earlier than 18 years, depending on their level of maturity.
Mature minors
The law provides that a child or young person can give valid consent to treatment when the child or young person has achieved a sufficient level of understanding and maturity that they understand fully what is being proposed.
This is also sometimes known as ‘Gillick competent’. The name comes from a 1986 English case in which Mrs Gillick was concerned about the possibility that her daughters might receive family planning advice without her consent. She sought a court order that a medical practitioner could not give advice or treatment to her daughters without her consent. The case went to the House of Lords, which held that a child or young person could consent on their own behalf, as long as the doctor was satisfied that the child understood the advice and that the treatment was in the best interests of the child.
Importantly, the child’s understanding needs to be considered in relation to each decision and in the particular circumstances. The fact that a child may have the capacity to consent to one type of treatment does not mean that they have the capacity in relation to all future treatment. The treating medical practitioner needs to satisfy themselves in each case that the child has the capacity to consent to the specific treatment at the particular time.
In general, the riskier the procedure, the higher the standard should be to ensure that the child has fully understood the nature of the procedure. Some issues for consideration include age, medical history, social background, how much of the issue the child understands and the complexity of the treatment that has been requested. There are some procedures to which particular considerations apply (Box 1).1
{kind=link}
A medical practitioner should be careful to ensure that their reasoning as to whether a child has capacity or not is recorded in the clinical notes.
Disputes between parents and children
If it is established that a child has capacity to provide consent and there is a disagreement between the child and their parent as to appropriate treatment, the wishes of the child will override those of the parent.
Even if a medical practitioner has determined that a child has the maturity and capacity to make their own decisions, it is likely that the child will need support for significant healthcare issues. It may be that a medical practitioner reaches a conclusion that it is in the best interests of the child to have their parents or guardians involved. In that case, it is advisable to discuss with the child the benefits of informing their parents or guardians about the proposed treatment. However, if a child refuses, they are entitled to the same confidential treatment of their medical information as an adult. Of course, as for adults, the doctor’s duty of confidentiality is not absolute, and there are circumstances where confidentiality may need to be broken (Box 2).
{kind=link}
Parents providing consent
If a child is not mature enough to make their own decisions, generally a parent or guardian can consent to treatment decisions on their behalf. Usually, consent of either parent is sufficient. The parent’s ability to consent on behalf of the child may be affected if:
- a parenting order is in place
- there is any question as to whether the treatment is in the best interests of the child
- the treatment is one that requires court authority.
Separated parents
Even if the parents of a child are separated, medical practitioners generally need the consent of only one parent. However, sometimes parenting orders permit only one parent to make medical decisions for the child or stipulate that one parent must notify the other parent before consenting to medical treatment. If parents are separated or divorced, it is best practice to enquire as to whether there are any parenting orders giving authority over medical decisions to one or other parent.
Parental disagreement
Sometimes, a doctor will be caught between parents disagreeing over the medical treatment of their child. It is the doctor’s duty to act in the best interest of the child; it is not their responsibility to counsel warring parents. In cases of disagreement, doctors may need to seek guidance from a court.
Outcome
After speaking to her medicolegal adviser, Dr White feels confident that she acted appropriately. She considered whether Clara understood the medication and treatment proposed, and whether she had the maturity and understanding to weigh up the options for herself. Dr White reached the conclusion that Clara did have capacity; however, as an additional step, she also spoke to Clara about the benefits of involving her parents and obtained Clara’s permission to discuss the treatment with one parent. Dr White made a detailed record of these steps in the notes. The medicolegal adviser reassures Dr White that she has done everything necessary and she would be in a good position to respond to any complaint that might be made.
Conclusion
When a child such as Clara presents to a medical practitioner for treatment, it is important that the medical practitioner assess the child and satisfy themselves of the child’s capacity to make the particular decision. It should be remembered that capacity may change depending on the complexity and implications of the decision. As in this case, although a child may have capacity to make a decision alone, they are likely to still need support with their treatment. The decision whether to involve someone else is for the child to make. However, we recommend that where medical practitioners feel it would be in the child’s best interests, they encourage the child to involve a supportive adult. If there is disagreement in the family, the decision of the child may be contentious. In this situation, it is particularly important to document the discussion and reasoning carefully in the medical record.
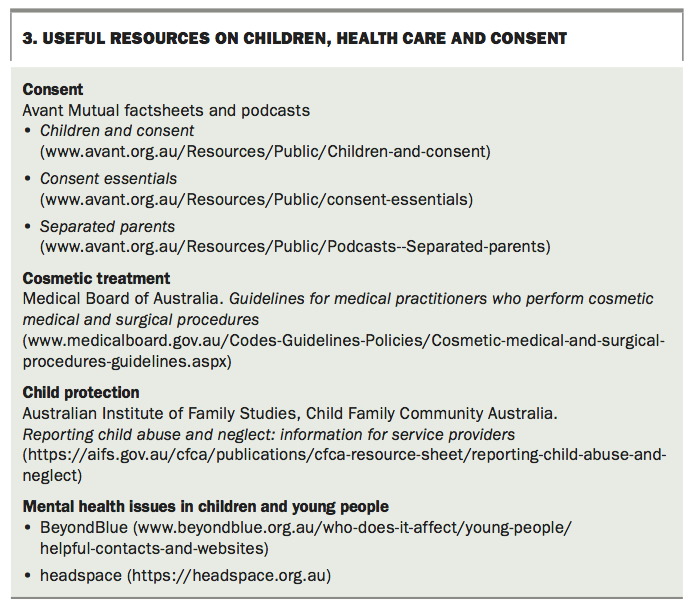
Useful resources about children, health care and consent are listed in Box 3. If there is a concern as to whether a child has the capacity to consent to treatment, medical practitioners can also contact their medical defence organisation for further assistance. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.