Iron deficiency anaemia in children: a practical guide for management

Dr Shanmuganathan is a Haematology Advanced Trainee, and Dr Ross and Dr Teo are Staff Specialists in Haematology in the Department of Haematology, The Children’s Hospital at Westmead, Sydney, NSW.
Children's health
This practical guide outlines an approach for the diagnosis, treatment and follow-up of children with iron deficiency anaemia, a common clinical problem seen by GPs and paediatricians.
- Iron deficiency anaemia in children is common and is most prevalent among toddlers and preschoolers.
- Dietary deficiency is the most common cause; a small number of patients will need investigations for other causes.
- Serum iron must not be used to assess iron stores; ferritin provides the most useful information about iron stores.
- Oral iron therapy is the most appropriate treatment for most patients; intravenous iron is indicated for a select few.
- The rate of haematological response is similar for oral and intravenous iron.
- Intravenous iron is not appropriate for iron deficiency without anaemia.
- Most children with iron deficiency anaemia do not need tertiary haematology care, and can be managed confidently by their GP or paediatrician.
The bulk of the body’s iron – 70 to 80% – is bound to the haem protein, haemoglobin, in red blood cells, and myoglobin, in muscle cells. Of the remainder, most is bound to the iron-storage protein ferritin and the iron-storage complex haemosiderin, and a tiny proportion (2 to 3%) is bound to enzymes such as the cytochromes. Consequently, changes to red blood cells are typically the first sign of iron deficiency.
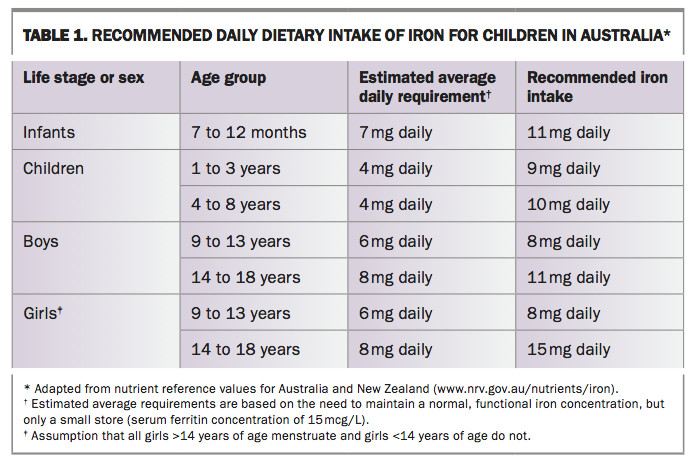
Iron absorption in the digestive tract is upregulated by iron deficiency, hypoxia and increased erythropoiesis, and decreased in inflammation, infection and iron repletion. The daily iron requirement changes with age. In healthy adults and older teenagers who have stopped growing, about 5% of daily requirements are derived from dietary sources (1 to 1.5 mg) to compensate for daily iron lost through the gastrointestinal tract, the skin and menstruation in females; iron recycled from the breakdown of old red blood cells provides the remaining 95%. However, the diet needs to provide 30% of the daily iron requirement in growing children (Table 1), particularly in the first few years of life and in adolescence, because of the increase in body mass that includes muscle and haemoglobin.1
{kind=link}
Iron deficiency (ID) is the most common nutritional deficiency in children and iron deficiency anaemia (IDA) is the most common cause of anaemia in children in both developed and developing countries, with significant adverse health consequences.2 It is most prevalent among toddlers and preschoolers, with a much higher prevalence among Indigenous children.3 The prevalence of IDA among children one to five years of age in the US is estimated to be 1 to 2%.4 A study of 678 preschoolers (9 to 62 months of age) in Sydney in the 1990s showed the prevalence of ID was 2.8% and IDA 1.1%; children between two and three years of age had the highest prevalence of IDA.5
Causes of iron deficiency anaemia in children
Inadequate dietary intake
Inadequate dietary intake is by far the most common cause of IDA. The inadequate intake of iron-rich foods that accompanies excessive cow’s milk intake in ‘milkoholic’ toddlers and preschoolers is the most common cause of IDA in children. Although it is rich in calories and other nutrients, cow’s milk contains no iron; however, children drinking iron-fortified milk-based formula are usually iron replete. Early introduction of cow’s milk before 12 months of age is also a risk factor for IDA.
Premature infants or infants born to mothers with severe iron deficiency may be born with lower iron stores than those born at full-term and are at risk of early-onset IDA if they are not given supplemental iron in the first few months of life. Children who are fussy eaters or on restricted or exclusion diets are also at risk, including those with developmental delay, autism and vegetarian or vegan diets. They may also be deficient in other micronutrients, such as vitamin B12.
Blood loss
In contrast to adults, blood loss is an uncommon cause of IDA in children. Sick and premature infants are at risk of depleted iron stores early in life owing to multiple blood tests and other haemorrhagic events such as surgery. Young children with cow’s milk protein intolerance present with IDA and a low plasma albumin level (with clinical oedema in some) because cow’s milk protein-induced enteropathy results in gastrointestinal blood and protein loss.
Other causes of gastrointestinal blood loss include inflammatory bowel disease, Helicobacter pylori gastritis and anatomical or vascular abnormalities that may bleed slowly. Excessive menstrual blood loss is a common risk factor for IDA in adolescent females.
Iron malabsorption
Iron is absorbed through the duodenum, and iron malabsorption is uncommon. Malabsorption may occur in disorders of the upper gastrointestinal tract such as coeliac disease, Crohn’s disease and surgical resection of the proximal small bowel.
Clinical features of iron deficiency anaemia
The presenting clinical features of iron deficiency anaemia in children may include the following:
- The child appears pale but is usually otherwise asymptomatic if the anaemia is not severe. Even when IDA is severe (haemoglobin < 50 g/L), many young children remain seemingly asymptomatic due to their compensatory ability.
- Some children may present with lethargy, irritability and anorexia, and a small number may appear very unwell, particularly if there is co-existing infection.
- Adolescents do not compensate as well and generally present earlier with lethargy, shortness of breath or syncope.
- Pica, most common in younger children with IDA, is the craving for eating nonfood items such as dirt, rocks, soap, paper or chalk. The underlying mechanism is unknown.
- Short-term neurocognitive changes may occur in young children with severe IDA, most commonly presenting with irritability in some young children;6 however, evidence showing long-term negative outcomes is lacking.4
- Cerebral vein thrombosis is rarely associated with IDA due to an unclear mechanism.7,8
Diagnosis
History and examination
Children in whom IDA is suspected should be assessed for a potential cause. A detailed history forms part of the diagnostic work-up and helps direct further investigations if indicated.
A history guided by the patient’s age is essential to assessing causes and risk factors for IDA. It should include the perinatal history in young children, a detailed dietary history, any history of gastro-intestinal symptoms and menstrual history in adolescent females. A family history of coeliac disease or thalassaemia, for example, should also be explored.
The physical examination may yield features of anaemia and its complications, if present. There may be signs to suggest the underlying cause, such as peripheral oedema in a toddler with cow’s milk protein intolerance. Invasive rectal and vaginal examinations are not appropriate in children and adolescents. Most often, the cause of IDA is not apparent on examination.
Investigations
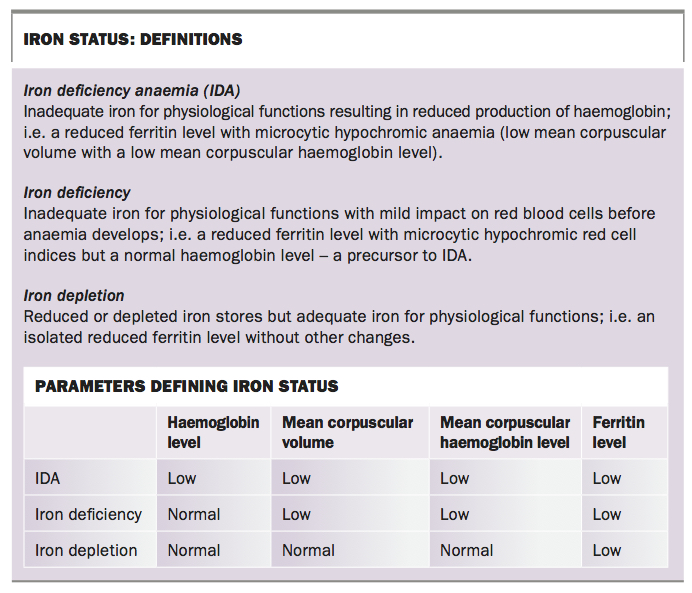
Basic screening investigations for every child with suspected iron deficiency comprise a full blood count and blood film, reticulocyte count, serum ferritin level and biochemical tests including plasma albumin level. IDA is defined by microcytic hypochromic anaemia and a low ferritin level (Box). The extent of the workup is dependent on the patient’s history and characteristics.
{kind=link}
Lead level should be considered in children displaying pica, and levels of other micronutrients such as vitamin B12 should be checked in patients with very restricted diets.
It would be appropriate to initiate screening tests such as a coagulation screen and von Willebrand studies to test for an underlying bleeding disorder in adolescent females with menorrhagia and IDA. Most children with IDA do not initially require endoscopy, unless the history suggests gastrointestinal disease.
Interpretation
Full blood count, blood film and reticulocyte count
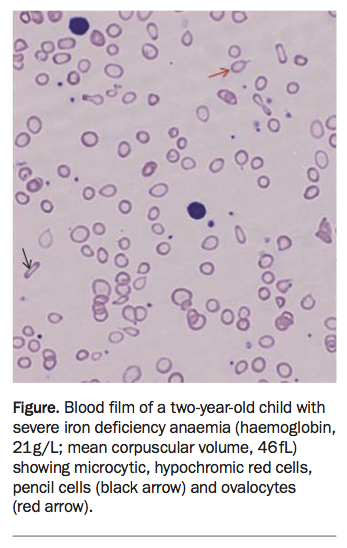
In IDA, the full blood count shows microcytic hypochromic anaemia with the characteristic blood film features of anisocytosis (red blood cells of different sizes), ovalocytes, elliptocytes and pencil cells (Figure). Reticulocytes (polychromasia on the blood film) are typically reduced.
{kind=link}
The main differential diagnoses for microcytic hypochromic anaemia are thalassaemia and anaemia of chronic disease but the red cell distribution width is usually not increased in these, and blood film features could help differentiate them from IDA.
Serum ferritin
Serum ferritin is the most useful test in assessing iron stores or iron status. A reduced ferritin level always indicates reduced iron stores. As it is an acute-phase reactant, a normal ferritin level does not exclude iron deficiency; in this case, the patient’s clinical characteristics, history and haematological features (and blood film) would usually provide enough information for the diagnosis of IDA to be made.
The rest of the iron studies panel (i.e. serum iron, transferrin and transferrin saturation) provides little, if any, useful information in assessing iron stores and is frequently misinterpreted, leading to unnecessary iron treatments, further tests and parental anxiety. Many young children who have never been iron deficient have been unnecessarily treated because of a low serum iron level. The serum iron level varies over the course of the day and is lowered in response to inflammation and infection. It must not be used to diagnose iron deficiency; its main use is in assessing iron poisoning or overdose.
The level of serum ferritin that is adequate or normal in healthy children is dependent on the patient’s age and dietary intake. Many pathology laboratories set their reference range limits for serum ferritin between 20 to 30 mcg/L and 300 to 350 mcg/L, which are inappropriately high cut-offs for children. In children without haematological features of iron deficiency, a serum ferritin level of greater than 10 mcg/L is adequate (based on the authors’ experience).
Results within the normal ranges for haemoglobin level, mean corpuscular volume, mean corpuscular hemoglobin level and red cell morphology indicate that there is enough iron for physiological needs even when the level of stored iron (ferritin) is low. This scenario is neither uncommon nor abnormal and is most commonly seen during periods of rapid growth in children who have enough dietary iron to meet their physiological needs but not enough to put significant amounts into stores (i.e. they have depleted iron stores).
Treatment
Blood transfusion
Blood transfusion is rarely required to treat IDA, as development of the condition is nonacute. The indication for transfusion is dependent on symptoms rather than the level of haemoglobin.
Most young children with severe IDA handle the anaemia well even when their haemoglobin level is less than 50 g/L. Those who are not coping with the anaemia should be referred to hospital for assessment and possible blood transfusion. Older adolescents are more likely to be symptomatic with severe anaemia, particularly if bleeding is ongoing (e.g. females with IDA and menorrhagia), and may benefit from blood transfusion.
Iron therapy: oral vs intravenous vs intramuscular
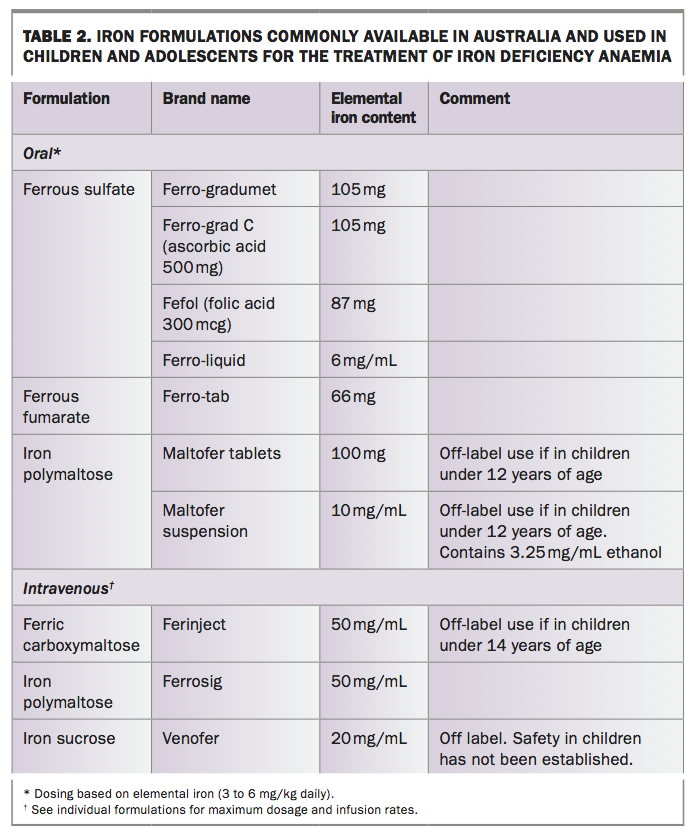
Oral iron is the most appropriate treatment for most children with IDA or ID. The recommended dosage of 3 to 6 mg/kg daily is based on the amount of elemental iron, and is given in divided doses or once daily with food or drink (liquid iron may cause a brown stain on teeth). Crushed iron tablets or granules from opened capsules may be sprinkled on food for young children (off-label use). Single element preparations (e.g. ferrous sulfate, ferrous fumarate and iron polymaltose) are recommended. The amount of iron in iron-containing multivitamins is generally inadequate for the treatment of IDA. Table 2 shows some of the commonly available preparations that are available over the counter.
{kind=link}
It is advisable to continue treatment for a further three to four months after correction of anaemia (based on a normal haemoglobin level) in order to replenish iron stores; patients taking the lower dosage of 3 mg/kg/day should have treatment extended to six months. Iron deficiency anaemia is likely to recur if iron stores are not adequately restored. Patients who have undergone a blood transfusion should also receive iron treatment at this dosage and for this duration.
Intravenous (IV) iron is indicated in selected patients, including those in whom oral iron has been ineffective or for whom oral administration is too difficult (e.g. children with autism). The dosage of IV iron should include an amount to replenish iron stores. The required dosage is determined from the following formula (Ganzoni method).9 Local paediatric services should be consulted if guidance is needed.
Cumulative iron dose (mg) = body weight (kg) x (target haemoglobin – actual haemoglobin [g/L]) x 0.24 + iron stores (mg)
Where:
- target haemoglobin = 130 g/L for body weight < 35 kg, and 150 g/L for body weight ≥ 35 kg
- iron stores = 15 mg/kg body weight for body weight < 35 kg, and 500 mg for body weight ≥ 35 kg.
There is a small risk of anaphylaxis and of skin staining (from extravasation) with IV iron.
Intramuscular iron injections are infrequently used as they are painful, usually more than one injection is needed and brown staining of the skin around the injection sites may last for months to years. IV iron is not appropriate for children without anaemia. Children with iron depletion should be treated by increasing dietary iron or supplementation with oral iron.
Address the cause
To avoid recurrence of IDA, the cause of iron deficiency should be addressed in addition to the patient receiving iron therapy. Dietary advice to ensure infants and toddlers have an adequate iron-rich food intake and avoid an excessive intake of cow’s milk is particularly pertinent for families. Adolescent females with menorrhagia may require hormonal therapy or treatment with antifibrinolytics to control menstrual bleeding.
Follow up
A full blood count and reticulocyte count seven to 10 days after initiating treatment is recommended to check the patient’s adherence to oral iron therapy. An early reticulocyte response is expected before the haemoglobin level improves.
Haemoglobin increments of 30 to 50 g/L can be expected in children with severe IDA after two to four weeks of treatment if they are adherent with oral therapy. Once the haemoglobin level has normalised, iron treatment is continued for a further three to six months. The full blood count and serum ferritin level are rechecked at the end of the treatment period. Further testing beyond that is not necessary for those with dietary-related IDA if an adequate diet is maintained.
The rate of correction of anaemia after IV iron therapy is similar to that seen with oral iron. IV iron may be more convenient in some circumstances but the rate of response is not different to that with oral iron.
Further investigations
Further investigations are indicated if iron malabsorption or blood loss are suspected at presentation or during the course of treatment. Patients who are slow to respond to treatment despite compliance with the correct dosage of oral iron may have coeliac disease (malabsorption) or gastrointestinal bleeding. Further tests may include coeliac serology, a urea breath test or a stool antigen test for H. pylori, or a faecal occult blood test.
Patients with recurrent IDA within a few months of completing treatment may be bleeding from the gastrointestinal tract, or may not have received enough iron to replenish iron stores or may not have had the underlying cause addressed. Thalassaemia and haemoglobin variants such as haemoglobin E should be considered if microcytic hypochromic features persist despite iron treatment, particularly if the patient’s ferritin level has normalised.
Referral
Patients with severe anaemia should be referred to a hospital for assessment, particularly if they have symptoms such as dizziness or shortness of breath. Severe anaemia is usually defined as:
- a haemoglobin level of less than 50 g/L in prepubertal children
- a haemoglobin level of less than 70 g/L in adolescents.
Patients with suspected gastrointestinal disease such as coeliac disease, inflammatory bowel disease or gut bleeding should be referred to a gastroenterologist for further evaluation. Adolescent girls with menorrhagia should be referred to a gynaecologist if their periods are difficult to manage. A referral to a dietitian may be helpful for some families.
Prevention
Dietary iron deficiency is avoidable with healthy eating, and education of parents on appropriate feeding would likely reduce the prevalence of iron deficiency in young children. As mentioned above, preterm infants should receive iron supplementation for the first few months of life. Also consider iron supplementation for children with restricted diets (e.g. those with autism or on vegetarian or vegan diets) and early intervention in girls with heavy menstrual periods.
Conclusion
Iron deficiency anaemia in children is common and most children can be confidently managed by the family GP or general paediatrician; only a small number with severe anaemia require tertiary care. Unlike adults, inadequate dietary iron is the most common cause of IDA in children. The full blood count and serum ferritin are the most useful tests; serum iron must not be used to assess iron stores or status. Oral iron is the most appropriate therapy and the underlying cause of IDA should be addressed to avoid recurrence. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.