Abnormal liver function test results in pregnancy – causes and management

It is common in pregnancy for patients to have abnormal liver function test results, and both pre-existing and unique pregnancy-related liver disorders need to be considered as a cause. Diagnosis and management require a systematic approach, with some of these conditions being associated with serious maternal and perinatal outcomes. The continued collaboration between the GP, obstetrician and gastroenterologist is crucial to ensuring good outcomes for mothers and their babies.
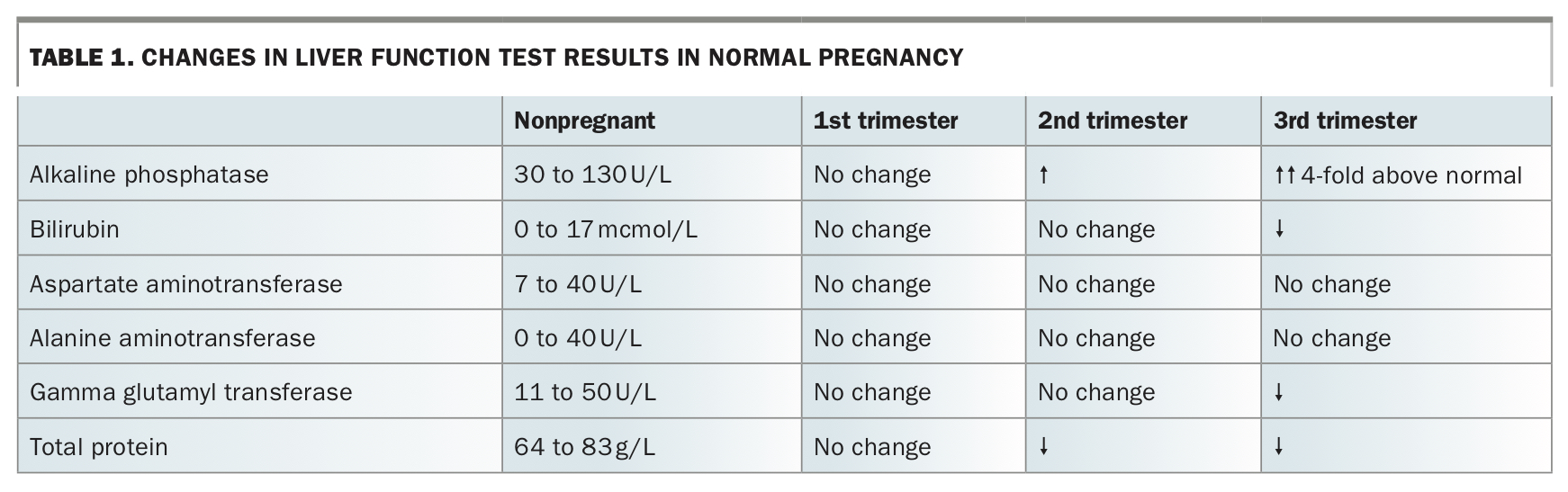
- The normal ranges for several liver function tests are different for pregnant patients compared with non-pregnant patients.
- An increase in serum alkaline phosphatase level is usually physiological; however, any rise in bilirubin or aminotransferase levels should be investigated.
- Both pregnancy-specific and primary liver pathologies need to be considered.
- Pre-eclampsia, HELLP (haemolysis, elevated liver enzymes and low platelets) syndrome, acute fatty liver of pregnancy and intrahepatic cholestasis of pregnancy can have associated perinatal morbidity and mortality.
- Blood tests and imaging are recommended to assist with diagnosis.
Abnormal liver function test (LFT) results are observed in about 3% of pregnancies.1 The physiological changes of pregnancy can unmask previously subclinical liver diseases, while disorders unique to pregnancy can also cause liver dysfunction.2-4 This article gives an overview of the challenges in diagnosis and management of abnormal LFT results in pregnant patients.
Physiological changes in LFT results during normal pregnancy
Pregnancy results in an increase in liver metabolism, a decrease in serum protein concentration caused by haemodilution, a slight decrease in serum aminotransferase levels and an increase in alkaline phosphatase level, which is often increased up to fourfold above the upper limit of normal by the third trimester (Table 1). The rise is due to placental alkaline phosphatase secretion and does not reflect liver injury, with gamma glutamyl transferase levels remaining unchanged. However, any increases in bilirubin or aminotransferase levels during pregnancy should be investigated.
{kind=link}
Diagnostic approach to abnormal LFT results
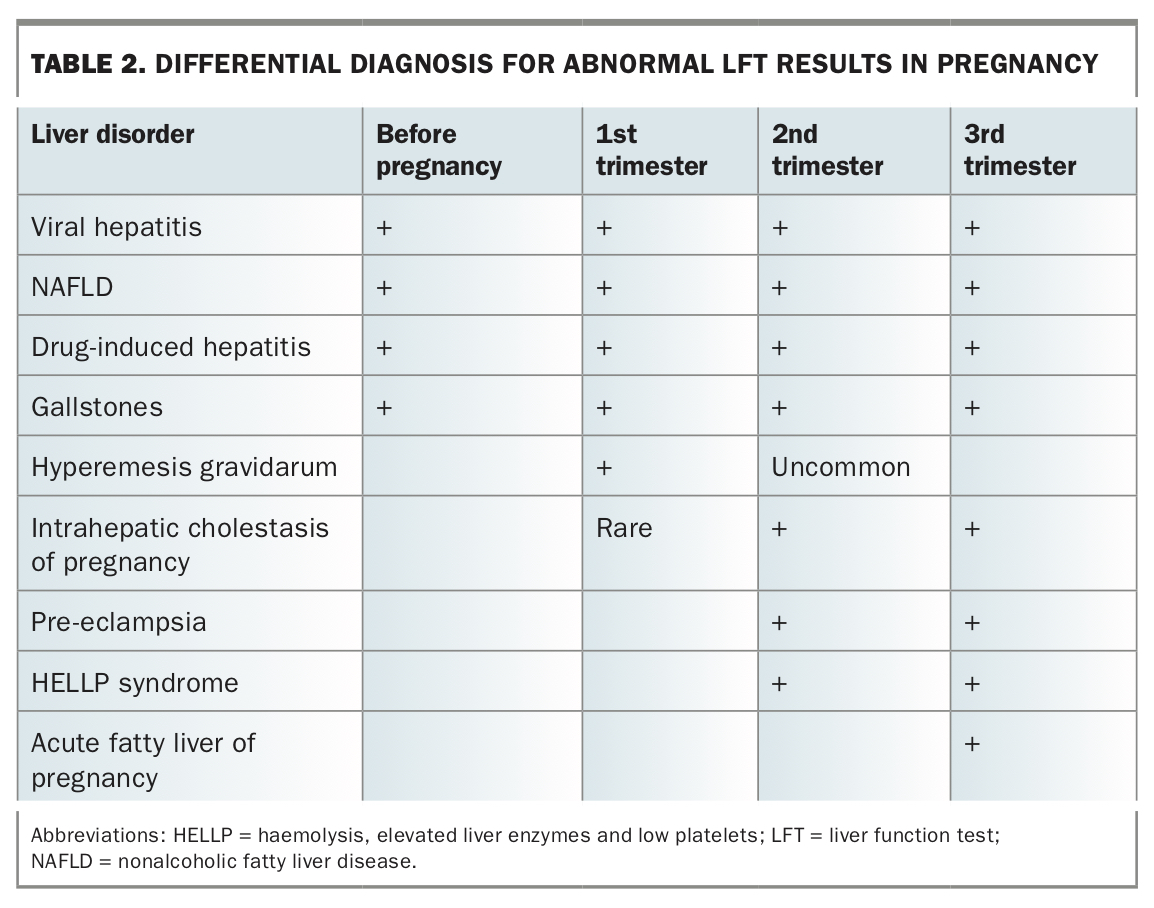
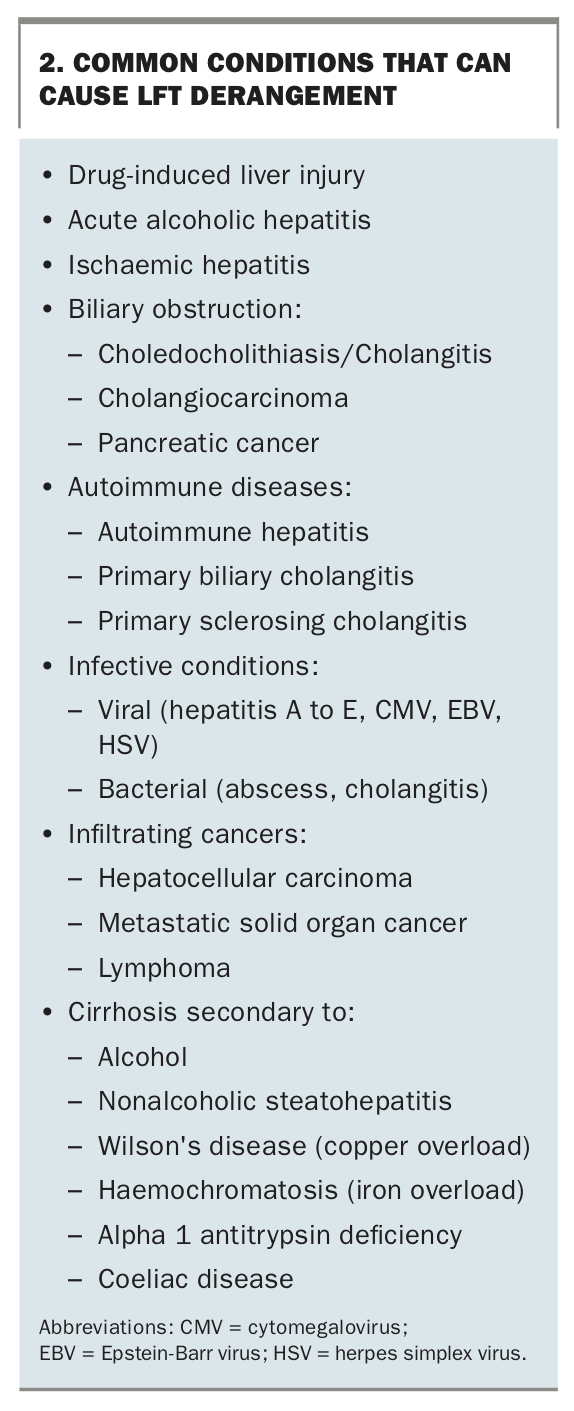
To determine the cause of abnormal LFT results in pregnancy, it is important to consider both new and pre-existing liver disorders (Flowchart). Reviewing results of LFTs done before pregnancy can help identify longstanding and nonpregnancy-related conditions such as nonalcoholic fatty liver disease (‘fatty liver’) or chronic viral hepatitis.
The patient history is key to guiding the differential diagnosis:
- A history of travel, injecting drug use and exposure to hepatitis can raise the suspicion of a viral hepatitis infection.
- A history of itch, particularly itch that starts in the palms and soles, is suggestive of intrahepatic cholestasis of pregnancy.
- A recent history of medication use, particularly antibiotics (e.g. amoxicillin-clavulanic acid, flucloxacillin), may suggest a drug-induced liver injury.
- Upper abdominal or right upper quadrant pain radiating to the back in a person with known gallstones suggests biliary colic.
- If pre-eclampsia or intrahepatic cholestasis has been documented in previous pregnancies, consider the possibility of recurrence.
The differential diagnosis varies by trimester of the pregnancy, with hyperemesis gravidarum occurring almost exclusively in the first trimester, whereas pre-eclampsia and HELLP (haemolysis, elevated liver enzymes and low platelets) syndrome present in the second half of pregnancy (Table 2).
{kind=link}
Physical examination of the abdomen during pregnancy can be challenging because of the enlarging gravid uterus. Also, typical stigmata of chronic liver disease, such as spider naevi, palmar erythema and oedema, are normal findings in pregnancy, making them less useful. Blood pressure measurement and urinalysis are important as pre-eclampsia, HELLP syndrome and acute fatty liver of pregnancy can all manifest with hypertension and proteinuria. Biliary tree imaging with ultrasound or magnetic resonance imaging can identify gallstone or primary biliary pathologies.
Specific conditions that cause abnormal LFT results in pregnancy
Hyperemesis gravidarum
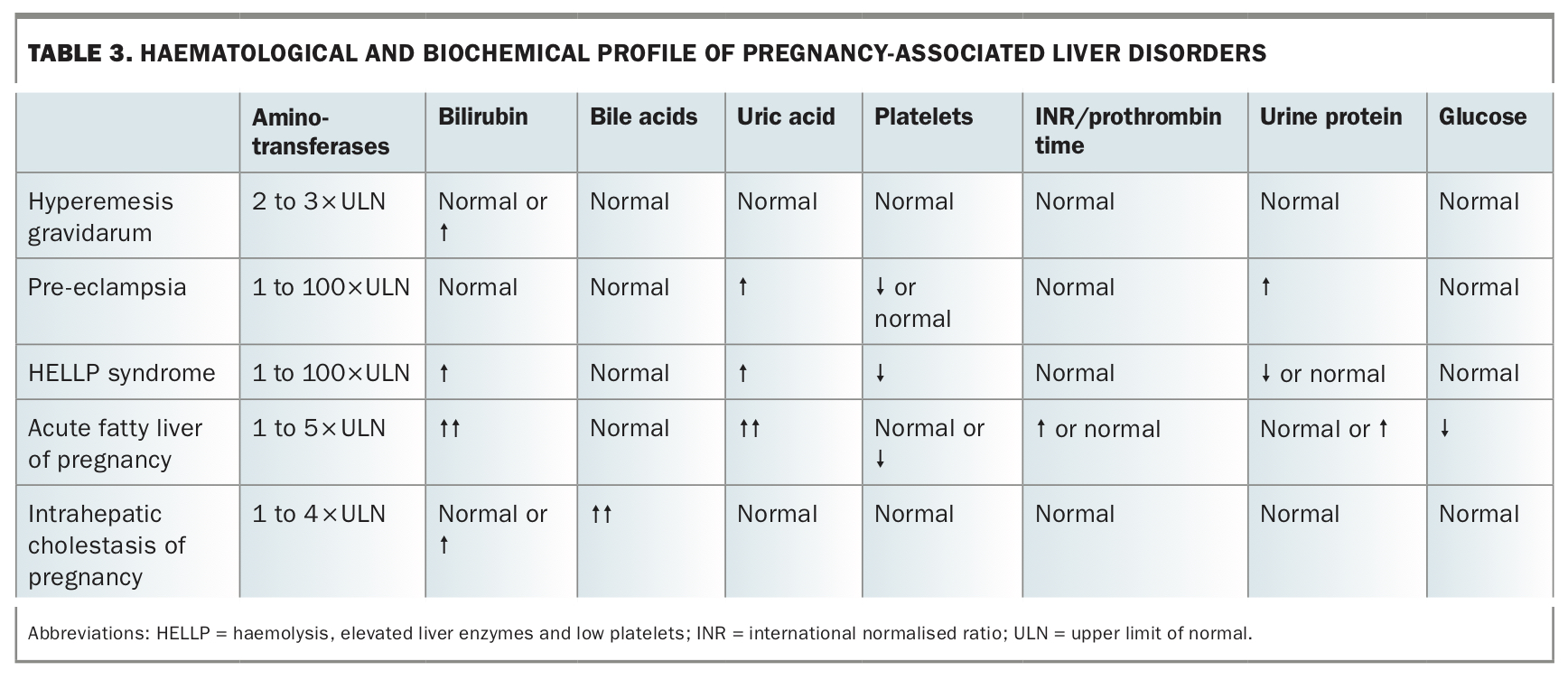
This first trimester disorder is characterised by intractable nausea, vomiting, dehydration and weight loss of more than 5% of body weight.3 Half of patients hospitalised with hyperemesis gravidarum have associated LFT derangement (Table 3). Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels can be elevated two- to threefold above normal but they usually normalise with treatment and improved oral nutrition.
{kind=link}
Management
The GP can manage patients with mild to moderate cases of hyperemesis gravidarum in an outpatient setting, with antiemetics. Where available, outpatient administration of IV fluids up to three times per week through ambulatory services can be used to prevent hospital admission. Patients with hyperemesis gravidarum who are unable to tolerate any oral intake should be referred to hospital for assessment. Patients with severe cases should be managed under the care of an obstetrician, with admission for antiemetics, electrolyte correction, thiamine and rehydration being the mainstay of treatment for severe cases. Rarely, patients with refractory cases require courses of corticosteroids and/or parenteral nutrition. For further details, refer to the Society of Obstetric Medicine of Australia and New Zealand guideline for the management of nausea and vomiting in pregnancy and hyperemesis gravidarum.5
Intrahepatic cholestasis of pregnancy
Intrahepatic cholestasis of pregnancy (ICP) occurs in about 0.7% of pregnant women in Australia.6 There are ethnic variations in ICP, with higher rates seen in South Asia and Chile. Although the aetiology is unclear, ICP is now considered to be a consequence of the effect of hormonal/metabolite alterations in individuals who are genetically susceptible to alterations in bile flow, including genetic polymorphisms within genes coding for biliary transporter proteins, such as the multidrug resistance protein 3 and bile salt export protein.2
Most cases of ICP present in the third trimester, but the condition can present earlier. The most common symptom is pruritus, which usually starts in the palms and soles of the feet. Aminotransferase levels can be raised to eight times normal. Jaundice is less common (less than 25% of cases) and should prompt a search for other pathologies. Serum bile acids should be measured as they are frequently elevated and help support the diagnosis. High serum bile acid levels above 40 mcmol/L have been associated with adverse outcomes for the fetus, including prematurity, stillbirth and neonatal distress.7 Bile acid levels above 100 mcmol/L have been associated with stillbirth rates of over 3%.8
Management
ICP is a self-limiting condition that resolves after delivery. Management is aimed at reducing maternal symptoms, namely itch. Antihistamines and topical emollients such as calamine lotion can be tried but the mainstay of treatment is ursodeoxycholic acid, a synthetic bile acid that is not currently subsidised by the PBS for this indication. Ursodeoxycholic acid is started at 10 mg/kg/day in divided doses that can be titrated (up to 15 mg/kg) as needed. Earlier meta-analyses had documented improvements in liver tests, pruritus and fetal outcomes, but a recent randomised trial did not show improved perinatal outcomes and the reduction in itching was too small to be considered meaningful.9-11 At present, ursodeoxycholic acid is still widely prescribed but patients must be made aware of the lack of robust data relating to perinatal events.
Early delivery (around 37 weeks gestation) is often recommended and close liaison with the obstetric team is crucial. ICP can recur in subsequent pregnancies. There is an increased risk of cholestatic jaundice with oestrogen use in patients with a history of ICP. Although pruritus usually resolves soon after delivery, LFT levels can take up to six weeks to return to normal. Cholestatic liver disorders such as primary biliary cholangitis need to be excluded if LFT changes persist beyond three months after delivery. If GPs are concerned about ongoing LFT derangement with an unclear cause then further investigation and referral to a hepatologist are recommended.
Pre-eclampsia and HELLP syndrome
Although hyperemesis gravidarum and ICP are fairly distinct disorders, pre-eclampsia, HELLP syndrome and acute fatty liver of pregnancy have overlapping features. Conceptually, pre-eclampsia and HELLP syndrome are regarded as primarily hypertensive disorders with liver injury occurring as collateral damage, whereas acute fatty liver of pregnancy is essentially a mitochondrial hepatopathy with a high likelihood of progression to acute liver failure.
Pre-eclampsia is characterised by hypertension (blood pressure above 140/90 mmHg after 20 weeks gestation), with dysfunction of at least one other end organ and/or fetal growth restriction. Liver involvement in pre-eclampsia is a consequence of endothelial dysfunction, hepatic vasoconstriction and fibrin deposition.3 Marked increases in ALT and AST levels may occur with significant liver involvement, but this is uncommon. Patients may be asymptomatic or present with right upper quadrant discomfort and hepatomegaly may be observed.
HELLP syndrome is a rare entity in the spectrum of pre-eclampsia, affecting 0.1 to 1% of all pregnancies and up to 20% of cases with severe pre-eclampsia. It commonly presents between 28 and 36 weeks gestation, but 30% of cases occur postpartum.3 As the name suggests, HELLP syndrome manifests with haemolysis (decreased haptoglobin, raised lactate dehydrogenase and schistocytes on peripheral blood smear), elevated liver enzymes (typically AST above two times the upper limit of normal and bilirubin above the upper limit of normal) and low platelets (typically below 100×109/L). It should be noted that changes in LFT levels can occur in severe pre-eclampsia without the full constellation of HELLP.
Patients with HELLP syndrome may be asymptomatic or present with right upper quadrant pain, nausea, vomiting and/or jaundice. Maternal complications include hepatic infarction, hepatic rupture, disseminated intravascular coagulation and consequences of maternal hypertension such as acute kidney injury and pulmonary oedema. As with all forms of severe pre-eclampsia, fetal complications of HELLP include prematurity, fetal growth restriction, placental abruption and stillbirth.
Management
Untreated HELLP syndrome carries a significant risk of maternal and fetal mortality (up to 5% and 30%, respectively). Therefore, all patients with suspected HELLP syndrome or pre-eclampsia should be referred to an obstetric unit for urgent assessment and management. Delivery of the fetus and placenta is curative; however, this may be delayed in some cases to allow administration of corticosteroids for fetal lung maturation or to reduce the risks of extreme prematurity.
Acute fatty liver of pregnancy
Acute fatty liver of pregnancy is a very rare disorder affecting between one in 7000 and one in 15,000 pregnancies. It typically presents in the third trimester and is associated with high maternal and neonatal mortality rates (10% and 25%, respectively). The pathogenesis of acute fatty liver of pregnancy is unclear, but defects in long-chain fatty acid oxidation pathways appear to play a role. Fetuses with a homozygous defect of long-chain 3-hydoxacyl-CoA dehydrogenase accumulate metabolites that may enter the maternal circulation and cause maternal liver injury.3
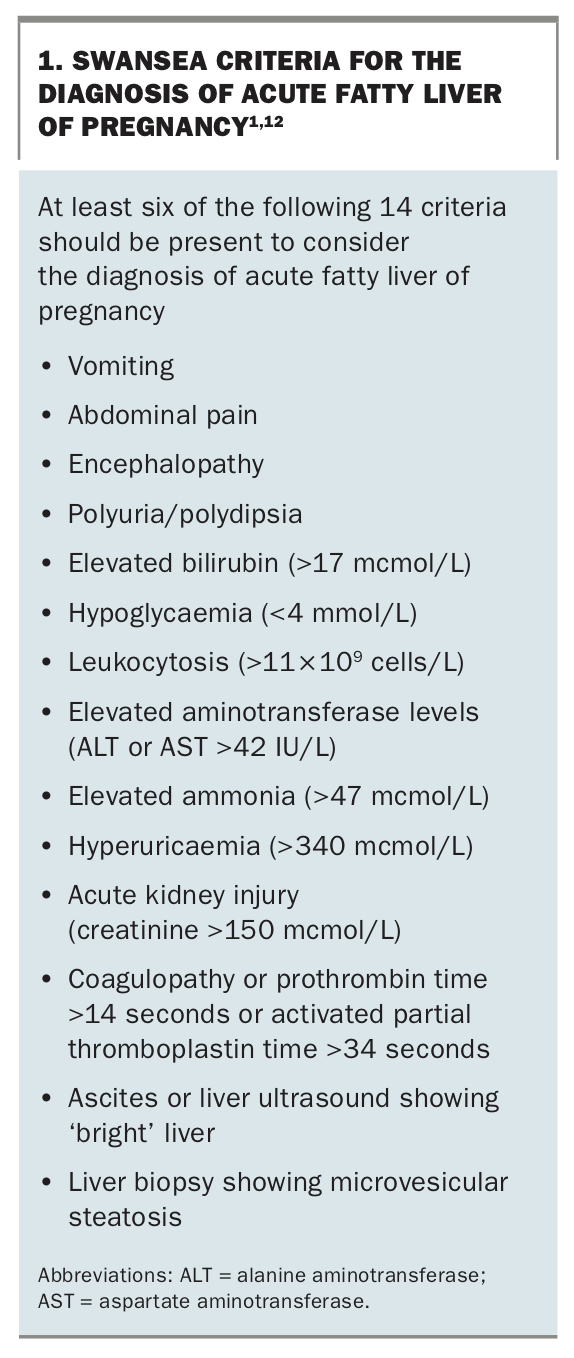
Early symptoms include fatigue, abdominal pain, nausea, vomiting and jaundice. This is followed by rapid development of acute liver failure. LFT levels can be elevated in a similar pattern to pre-eclampsia or HELLP syndrome, with aminotransferases elevated five to 10 times the upper limit of normal, although in acute fatty liver of pregnancy the bilirubin level is usually also elevated (Table 3). However, the clinical presentation is more severe with patients developing progressive multiorgan failure, often with worsening jaundice and encephalopathy. Laboratory tests increasingly reflect a failing liver with hypoglycaemia, hyperammonaemia and an elevated prothrombin time. These and other clinical/imaging criteria (Swansea criteria) are useful in making a diagnosis, with a positive predictive value of 85% and a negative predictive value of 100% (Box 1).1,12
{kind=link}
Management
GPs should contact the obstetric unit about any patient they are worried may have acute fatty liver of pregnancy. Patients with a suspected diagnosis of acute fatty liver of pregnancy must be admitted to hospital under the care of the obstetrics team and the fetus delivered expediently if the diagnosis is confirmed. Patients with organ dysfunction may require supportive care in an intensive care unit. There are a few case reports of recurrence of acute fatty liver of pregnancy in subsequent pregnancies.13,14
Gallstone disease
The physiological changes of pregnancy (e.g. hormone changes and gallbladder dysmotility) lead to biliary sludge and gallstone formation in about 3% and 2% of pregnancies, respectively. Symptomatic gallstone disease usually presents in the second and third trimesters. The presenting symptoms are similar to those in nonpregnant individuals. Elevations in ALT, AST and/or bilirubin levels can occur when gallstones enter the bile ducts (choledocholithiasis). It should be noted that although cholelithiasis can cause nausea and biliary colic, it does not usually cause LFT derangement. Cholangitis results in LFT derangement, fevers, right upper quadrant pain and nausea. Acute cholecystitis can sometimes result in LFT derangement as well as fever and right upper quadrant pain.
Management
GPs should contact the gastroenterology unit as well as an obstetrician for symptomatic patients with suspected or imaging proven choledocholithiasis/cholangitis. Endoscopic retrograde cholangiopancreatography is the treatment of choice for choledocholithiasis. It can be performed in pregnancy after the first trimester, with careful shielding of the fetus to avoid radiation exposure and minimising fluoroscopy duration. Acute cholecystitis should be managed aggressively given the risk of triggering preterm labour. Laparoscopic cholecystectomy is best avoided in the first trimester but may be safely performed in the second trimester.
Viral hepatitis
The Royal Australian and New Zealand College of Obstetrics and Gynaecology guidelines recommend screening for hepatitis B in all women planning pregnancy or in early pregnancy.15 Antenatal hepatitis C screening should be considered based on patient risk factors and state guidelines.16
The course of acute viral hepatitis in pregnancy is similar to that for nonpregnant individuals, usually lasting a few weeks to months. An exception is acute hepatitis E, which is seen particularly in travellers from endemic areas in South/South-east Asia and North Africa, as the maternal mortality can reach 30% and fetal loss is very high, at about 50%.17
Preventing perinatal transmission
Vertical transmission of hepatitis A has been described in case reports.18 Hepatitis A immunoglobulin should be administered to neonates of women who become infected within two weeks of delivery. Women with chronic hepatitis B should have their LFT levels and hepatitis B viral load monitored during pregnancy. Antiviral prophylaxis with tenofovir is offered to patients with viral loads above 200,000 U/mL in the third trimester to reduce perinatal transmission of hepatitis B. Vertical transmission of hepatitis C is uncommon except in mothers with HIV infection or if there is fetal exposure to blood. Invasive monitoring procedures should be avoided. Currently, there are no data on the safety of hepatitis C treatment during pregnancy or breastfeeding, and treatment should be deferred.
Herpes simplex virus (HSV) hepatitis can also present in pregnancy with fever and high serum aminotransferase levels without jaundice. The typical mucocutaneous features may be absent in over 50% of cases. If HSV hepatitis is suspected, a serum HSV polymerase chain reaction assay should be performed and empiric intravenous acyclovir started as an inpatient as the fetal-maternal mortality can be high (about 40%).
Other conditions specific to the liver
Management of other pre-existing or new liver diseases discovered in pregnancy should be addressed on a case-by-case basis (Box 2). In general, adequate control of maternal disease leads to better maternal and fetal outcomes. Therefore, patients with well-controlled autoimmune hepatitis or Wilson’s disease should not stop taking their medications during pregnancy. However, dose modifications or alternative drug use (e.g. azathioprine instead of mycophenolate) may be necessary.
{kind=link}
Ideally, patients with underlying liver conditions, particularly cirrhosis with portal hypertension, should be referred preconception to a maternal fetal medicine unit and to a hepatologist to ensure adequate prepregnancy counselling and disease optimisation. Patients with portal hypertension can develop variceal haemorrhage, with the risk being greatest in the second trimester and at the time of delivery. When indicated, prepregnancy endoscopic surveillance with variceal banding is preferred. Otherwise, gastroscopy can be performed safely in the second trimester in patients with pre-existing oesophageal-gastric varices.19
Conclusion
LFT derangement in pregnancy is common. Determining the cause of liver function derangement requires a systematic approach with history, examination and investigations. Some of the conditions that result in liver function derangement require prompt treatment, so establishing the correct diagnosis is important. GPs are the first point of contact for many pregnant patients and are likely to need to start the investigation process when LFT derangement is discovered. If GPs are ever concerned or worried about a pregnant patient with abnormal LFT results, they should contact an obstetrician and/or hepatologist for advice. The combined care of the GP, obstetrician and hepatologist is crucial to ensuring good patient outcomes. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.