Diabetic kidney disease and CVD
 © CRYSTAL LIGHT/STOCK.ADOBE.COM
© CRYSTAL LIGHT/STOCK.ADOBE.COM
Dr Østergaard is a Visiting Scientist at Department of Diabetes, Central Clinical School, Monash University, Melbourne; and Physician and Research Fellow at the Department of Endocrinology and Internal Medicine, Aarhus University Hospital and Steno Diabetes Center Aarhus, Aarhus, Denmark. Professor Cooper is a Professor at Department of Diabetes, Central Clinical School, Monash University and a Clinical Endocrinologist at Alfred Health, Melbourne, Vic.
Diabetic kidney problems
Heart diseases
Diabetic kidney disease is a common complication in both type 1 and type 2 diabetes. Appropriate surveillance of kidney function and timely intervention are key to mitigate the severity and burden of this disease. This article summarises the current recommendations for monitoring and treating diabetic kidney disease in general practice as well as emphasising its link to the risk of cardiovascular disease.
Correction
A correction for this article was published in the December 2020 issue of Medicine Today. The online version and the full text PDF of this article (see link above here) have been corrected.
- Early recognition of diabetic kidney disease is important for early intervention to reverse, halt or slow the progression of the disease.
- Close monitoring of urinary albumin excretion and estimated glomerular filtration rate is required to detect diabetic kidney disease.
- Tight blood pressure and glucose control are cornerstones in the treatment of diabetic kidney disease.
- Sodium glucose transporter 2 inhibitors and glucagon-like peptide 1 receptor agonists are new classes of glucose-lowering drugs that seem to be particularly renoprotective.
- Patients with a urinary albumin-to-creatinine ratio higher than 30mg/mmol or an estimated glomerular filtration rate of less than 30mL/min/1.73m2 should be referred to a nephrologist.
Diabetic kidney disease is a chronic complication of both type 1 and type 2 diabetes. About 30% of individuals with diabetes develop diabetic kidney disease, also known as diabetic nephropathy, despite increasing efforts to modify risk factors, including blood pressure and glycaemic control.1 Furthermore, in Australia as well as in other western countries, diabetes remains the most common cause of end-stage renal disease requiring either kidney transplantation or dialysis.2
As diabetic kidney disease is a progressive disease, which can be halted, reversed or slowed at an early stage, it is essential to identify this specific complication of diabetes, so that it can be monitored and treated in an optimal manner. The risk of cardiovascular disease (CVD) is significantly increased in patients with diabetic kidney disease; therefore, it is crucial to identify symptoms and signs of heart and macrovascular disease, which can be difficult to detect early. Furthermore, it is important to commence strategies directed at protecting both the kidney and the cardiovascular system as soon as possible.
Diagnosis and monitoring
Diabetic kidney disease is diagnosed based on evidence of renal injury as reflected by an abnormal urinary albumin excretion and/or a reduced estimated glomerular filtration rate (eGFR) in the context of diabetes. As a late complication, diabetic kidney disease is classically observed after 10 years of type 1 diabetes and usually in conjunction with diabetic retinopathy. However, the time course of diabetic kidney disease in type 2 diabetes is less clear, presumably because of the presence of incipient abnormalities in glucose homeostasis before the development of overt diabetes, which may therefore be present at the same time as when diabetes is diagnosed.
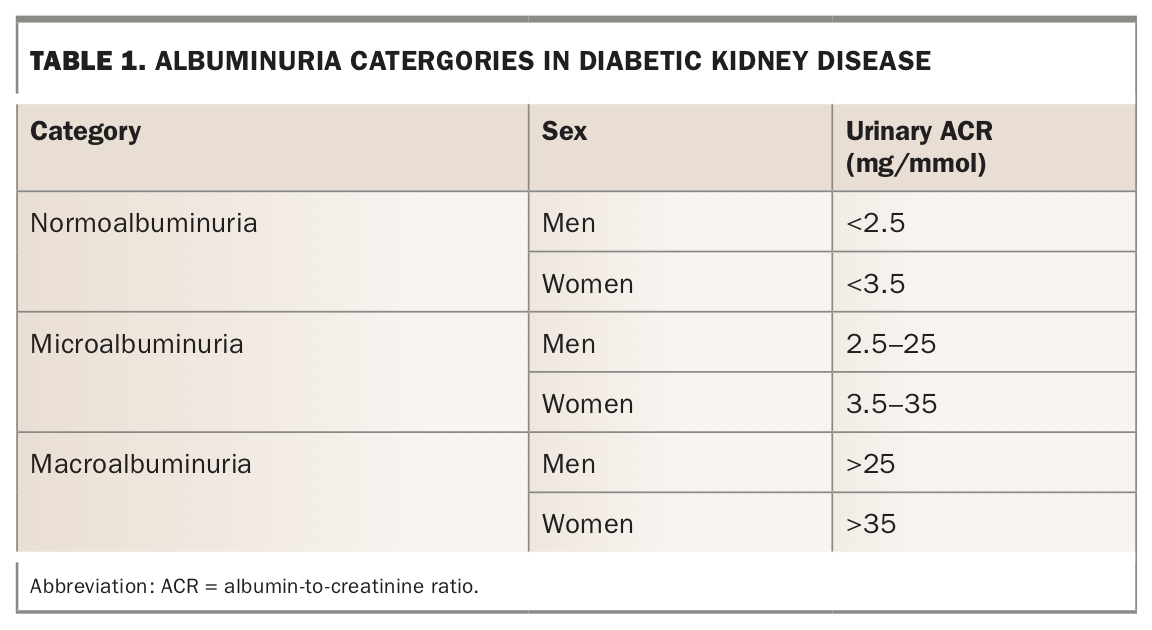
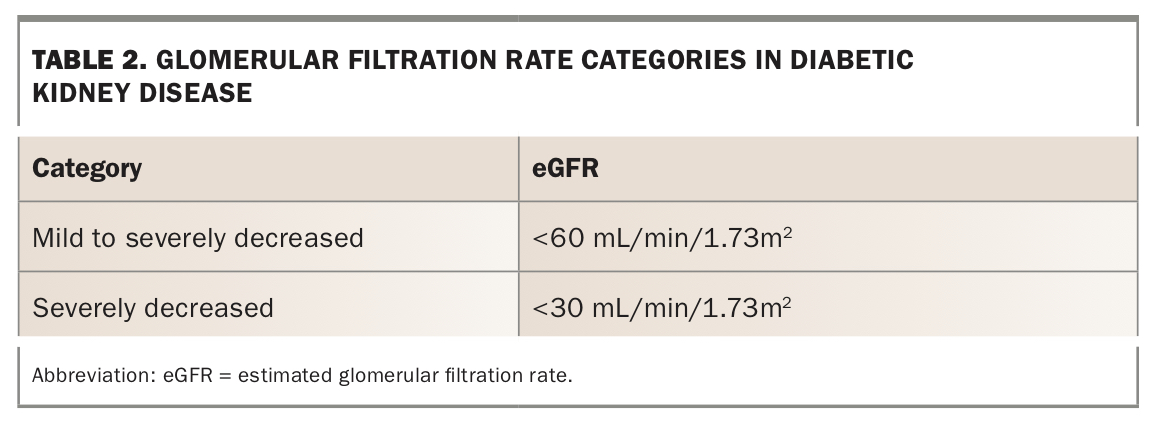
It is recommended that the urinary albumin-to-creatinine ratio (ACR) and eGFR should be monitored at least once per year in all patients with type 2 diabetes and in those with type 1 diabetes with a duration of more than five years.3 ACR and eGFR are traditionally graded by increasing severity as shown in Table 1 and Table 2.4
{kind=link}
{kind=link}
The ACR may be falsely elevated during infections, severe hypertension, menstruation and after exercise. eGFR may similarly be affected by exercise or loss of muscle mass.
Diabetic kidney disease is defined as a persistent abnormal ACR and/or reduced eGFR in two out of three measurements in a patient with no other cause of renal impairment. Alternative causes of renal impairment must be considered in certain settings, such as rapid change in eGFR or ACR, concomitant haemoglobinuria, severe hypertension or another systemic disease, which may explain the renal impairment. Furthermore, renal findings after only a short duration of type 1 diabetes may also indicate a nondiabetic cause of kidney injury.
Management
Glucose control
Improving glucose management decreases the risk and the rate of progression of diabetic kidney disease and is therefore a cornerstone in the prevention and treatment of the condition.5,6 The stage of renal impairment should be considered in patients with type 2 diabetes, as this has an impact on the choice of pharmacological treatment and the suggested algorithm of escalation. Furthermore, evidence of CVD or presence of cardiovascular risk factors, as well as the personalised glycaemic targets, are other considerations when developing a glucose-lowering plan for these patients.
Metformin, sodium glucose transporter 2 (SGLT-2) inhibitors and glucagon-like peptide 1 (GLP-1) receptor agonists deserve special mention in the context of diabetic kidney disease. Although sulfonylureas remain widely used in patients with diabetes at risk of diabetic kidney disease, these agents have not been shown to be renoprotective independently of their glucose-lowering effect. Nevertheless, in the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation) study, a significant proportion of patients who were taking the sulfonylurea gliclazide had improved renal outcomes.7
Metformin
Metformin is still the most often chosen first-line therapy for glucose lowering in people with type 2 diabetes. The dose of metformin should be adjusted if eGFR is less than 45 mL/min/1.73m2, and is contraindicated if eGFR is less than
30 mL/min/1.73m2. Metformin itself has not been shown to be renoprotective independent of its glucose-lowering actions.
Sodium glucose transporter 2 inhibitors
Clinical trials have demonstrated the cardiovascular benefits of the addition of SGLT-2 inhibitors to existing antidiabetic treatments in patients with type 2 diabetes who have established CVD. The SGLT-2 inhibitors empagliflozin, dapagliflozin and canagliflozin were all found to have significant protective effects on cardiovascular events in these study populations when added to existing treatments.8-10
This drug class is also attracting special attention because of emerging evidence of kidney-protective effects, which presumably are not solely explained by their glucose-lowering effects. Canagliflozin is the drug within this class that is best characterised with respect to the effects on renal function as described in the landmark CREDENCE (Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation) trial.11 In patients with type 2 diabetes and ACR of 300 to 5000 mg/g and eGFR ranging from 30 to 9 mL/min/1.73m2, canagliflozin reduced the incidence of the primary outcomes including worsening of renal function and mortality from renal or cardiovascular causes as well as additional secondary renal specific outcomes.11 However, it is important to note that canagliflozin is no longer available on the PBS.
A renally dedicated study, the DAPA-CKD (Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease) trial, which evaluated the effect of dapagliflozin on renal outcomes and cardiovascular mortality in patients with chronic kidney disease, has been terminated early due to positive results, although the full data set is not yet publicly disclosed. These results are in line with the secondary outcomes reported in the specific cardiovascular outcome trials using empagliflozin, dapagliflozin and canagliflozin.9,12,13 These benefits are likely to be glucose independent since in patients with a low GFR (<45 mL/min/1.73m2) no clear cut reduction in glycosylated haemoglobin (HbA1c) levels has been observed in various clinical trials14 despite this class of drugs conferring renoprotection in a population with low GFR.11
Finally, it is important to emphasise that patients included in these trials either had established CVD or were at high risk of CVD and the effects of these drugs in other populations of type 2 diabetes, such as in those without these complications, remain to be determined. Another exciting finding from this class of drug is the identification of a significant reduction in heart failure in people with type 2 diabetes.9,12,13 Furthermore, this benefit also appears to be unrelated to glucose lowering since in the DAPA-HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) study the risk of worsening heart failure or death from cardiovascular causes was lower, even in people without diabetes.15
Glucagon-like peptide 1 receptor agonists
Clinical trials have investigated the cardiovascular outcome of the addition of GLP-1 receptor agonists to existing antidiabetic treatments. In these trials it was reported that the addition of the GLP-1 receptor agonists liraglutide, semaglutide and dulaglutide to existing hypoglycaemic agents in patients with type 2 diabetes and established CVD or at high risk of CVD reduced the risk of cardiovascular events.16-18 Semaglutide and dulaglutude but not liraglutide are currently available on the PBS. Specific cardiovascular effects among the various trials were not uniform with effects on coronary events and stroke reported in some but not all trials. Furthermore, unlike SGLT-2 inhibitors, no effect on heart failure was observed with this class of drugs.
In addition, the evaluation of secondary outcomes in the cardiovascular outcome trials of GLP-1 receptor agonists indicated that these drugs are kidney protective in addition to their effects on blood glucose, body weight and cardiovascular events when added to existing glucose-lowering therapy.19-22 This includes studies of lixisenatide, exenatide, liraglutide, semaglutide and dulaglutide.19-22 In general, these agents do not appear to be as impressive on renal endpoints as SGLT-2 inhibitors. Reduction in albuminuria has generally been observed with these agents, which appears to be, at least in part, glucose independent. Effects on eGFR have not been consistent but the recent REWIND (Researching Cardiovascular Events with a Weekly Incretin in Diabetes) trial with dulaglutide reported a reduced incidence of a 40% and 50% decline in eGFR.23 These intriguing results have stimulated the commencement of dedicated renal trials with this class of drug.
Blood pressure lowering
The importance of blood pressure lowering regarding both mortality, cardiovascular events and new or worsening of albuminuria in patients with type 2 diabetes has been confirmed in a meta-analysis of over 100,000 participants.24
Blockade of the renin-angiotensin-system has been shown to have cardiac and renoprotective effects in hypertensive patients with type 2 diabetes and signs of diabetic kidney disease. Therefore, both ACE inhibitors and angiotensin 2 receptor blockers are recommended in this population, but not as dual therapy since this combination approach has been associated with hyperkalaemia and acute decline in renal function. The ACE inhibitor captopril was shown to prevent the deterioration of kidney disease in patients with type 1 diabetes who have increased urinary albumin excretion with or without hypertension.25 Similar renoprotective effects of angiotensin II receptor blockers were later observed in patients with type 2 diabetes in the RENAAL (Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan) and the IDNT (Irbesartan Diabetic Nephropathy Trial) trials.26-28 Subsequent studies also confirmed benefits in patients with type 2 diabetes with earlier disease as reflected by the presence of microalbuminuria.27 In these studies of patients with microalbuminuria, there was a decreased progression to overt proteinuria and increased regression to normoalbuminuria.
It should be noted that the role of renin-angiotensin-system blockers in the setting of normal blood pressure and normoalbuminuria has not been clearly demonstrated.
Blood pressure targets remain controversial but in the 2020 position statement from the American Diabetes Association, a blood pressure target of less than 140/90 mmHg is recommended to reduce CVD mortality and slow the progression of chronic kidney disease in all people with diabetes. However, it is also suggested to consider setting personalised lower targets (e.g. <130/80 mmHg) on the basis of potential benefits and risks in patients with diabetic kidney disease as they have a high risk of progression, especially in the presence of increased albumin excretion, as well as CVD.3
When to refer
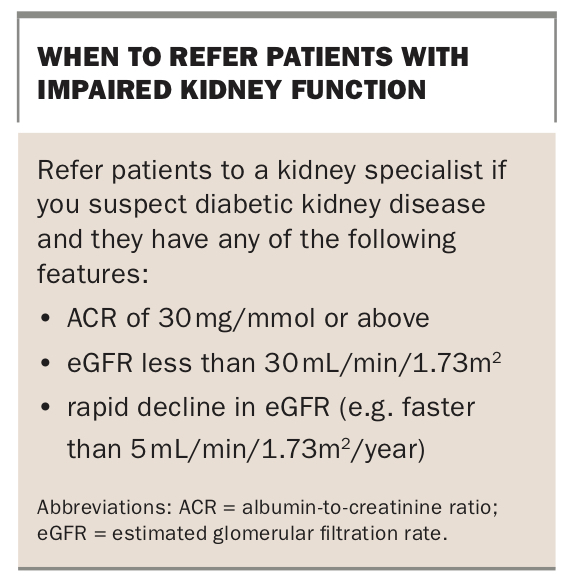
Patients with impaired kidney function, such as decreased eGFR or abnormal ACR of unknown cause, should always be considered for referral and review by a kidney specialist (see Box). Furthermore, if the cause of kidney disease is unknown and there are atypical clinical features, such as absence of retinopathy, overt haematuria and clinical features not typical of diabetes, patients should be referred to a nephrologist as renal biopsy may need to be undertaken to confirm the underlying diagnosis.
{kind=link}
Conclusion
Annual monitoring of ACR and eGFR is recommended for all patients with type 2 diabetes and in those with type 1 diabetes with a duration of more than five years. Addition of an SGLT2 inhibitor or a GLP-1 receptor agonist to existing glucose-lowering therapy should be considered when metformin is insufficient to maintain glucose control, and end-organ protection (both cardiovascular and renal) is a treatment priority. ACE inhibitors and angiotensin 2 receptor blockers have pleiotropic renoprotective effects in patients with diabetic kidney disease and should be used if possible to slow or reverse disease progression. Patients with signs of severe disease, including those with an ACR of 30 mg/mmol or above and/or eGFR of less than 30 mL/min/1.73m2, should be referred to a nephrologist. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.