Nonalcoholic fatty liver disease

Liver diseases
Metabolic disorders
Disease progression in patients with nonalcoholic fatty liver disease (NAFLD) occurs more commonly in patients with other features of the metabolic syndrome. Primary care physicians play an important role in diagnosing NAFLD, managing metabolic risk factors and noninvasive assessment of disease stage.
- Nonalcoholic fatty liver disease (NAFLD) affects about a quarter of Australia’s population.
- NAFLD encompasses a broad spectrum of clinical disease ranging from benign simple steatosis to end-stage cirrhosis.
- Patients with the metabolic syndrome are more likely to have NAFLD and more likely to have progressive liver disease from NAFLD.
- A noninvasive assessment for fibrosis and cirrhosis should be performed in patients with NAFLD.
- All patients with NAFLD should be counselled about the importance of weight loss and exercise.
- There is currently no approved, disease-modifying therapy for NAFLD and patients who have significant liver disease due to NAFLD should be referred to a gastroenterologist for assessment and consideration of participation in a clinical drug trial.
Nonalcoholic fatty liver disease (NAFLD) encompasses a spectrum of clinical disease ranging from benign fat accumulation in the liver (simple steatosis) to severe nonalcoholic steatohepatitis (NASH) causing cirrhosis and hepatocellular carcinoma. NAFLD is the most common cause of deranged liver function test results in Australia, and a recent study has found that its clinical significance is often underappreciated.1 This article provides practical information for primary care givers on the management of patients with NAFLD and its metabolic disease associations.
What is NAFLD?
NAFLD is defined as the presence of fat in the liver (known as steatosis) in the absence of a secondary cause such as excessive alcohol intake (>20 g daily for women and >30 g daily for men).2 Patients with NAFLD are asymptomatic until late stages of the disease and the diagnosis is often made incidentally. The requirements for diagnosis of NAFLD are summarised in Box 1.
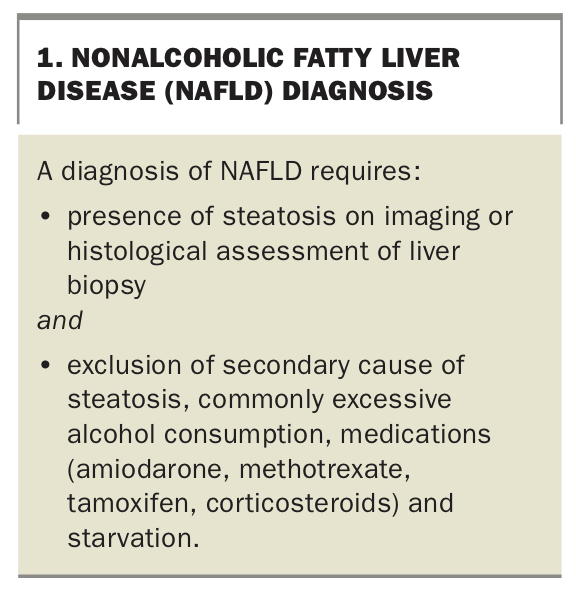{kind=link}
Liver function test results do not have to be abnormal to make a diagnosis of NAFLD; however, mild to moderate elevations of alanine aminotransferase (ALT), aspartate aminotransferase (AST) and gamma glutamyltransferase (GGT) levels are common among people with NAFLD in the absence of symptoms. A diagnosis of NAFLD should be suspected in patients who have any of the following:
- elevated liver enzymes (ALT/AST >30 IU/L or GGT >60 IU/L)
- steatosis on ultrasound or CT imaging
- two or more of the comorbidities from the metabolic syndrome.
In a patient with suspected NAFLD, clinicians should exclude other aetiologies of steatosis or elevated liver enzymes and try to establish whether the patient has fibrosis or cirrhosis.
How common is NAFLD?
There are no published Australian data on the prevalence of NAFLD in adults, although its prevalence is estimated to be 25% from a study of its global burden.3 The current burden of NAFLD in Australia is estimated to be 5.5 million cases, and is predicted to increase to 7 million by 2030.4 Although NAFLD is more common among elderly patients, an Australian study found its prevalence to be 15% among a cohort of adolescents.5,6 A total of 21% of this cohort had a body mass index in the obese range.
The natural history of NAFLD
The clinical spectrum of NAFLD ranges from benign, nonprogressive steatosis to end-stage cirrhosis with liver failure and hepatocellular carcinoma. The three main stages of NAFLD and their risks of progression to end-stage liver disease are shown in Box 2. A range of clinical and biochemical features can suggest the most likely NAFLD stage in an individual patient.
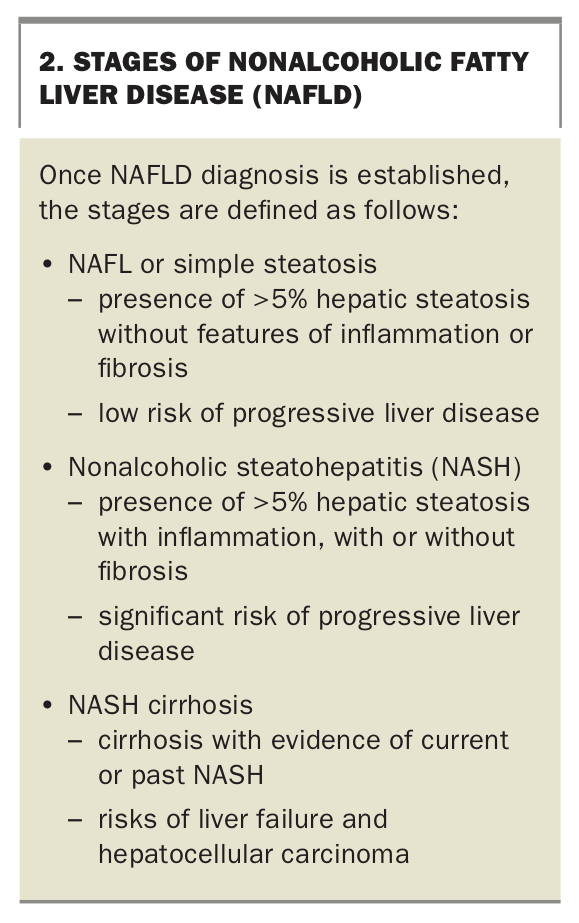{kind=link}
The progression of NAFLD to NASH was previously shown to occur in about 10 to 30% of patients;7,8 however, more recent data suggest that the true rate of progression may be higher, with one study showing that nearly half of patients with biopsy-proven simple steatosis progressed to NASH over an average 6.6-year period.6 The Figure illustrates the progression of NAFLD to NASH and cirrhosis.9 Reversal of liver injury back to NAFL can be achieved in patients with established NASH. The progression of NAFLD to cirrhosis is estimated to occur in up to 20 to 30% of patients, with higher rates of progression reported in studies with longer follow-up periods. Patients with NAFLD who have diabetes or obesity or who consume alcohol heavily are at increased risk of disease progression.10
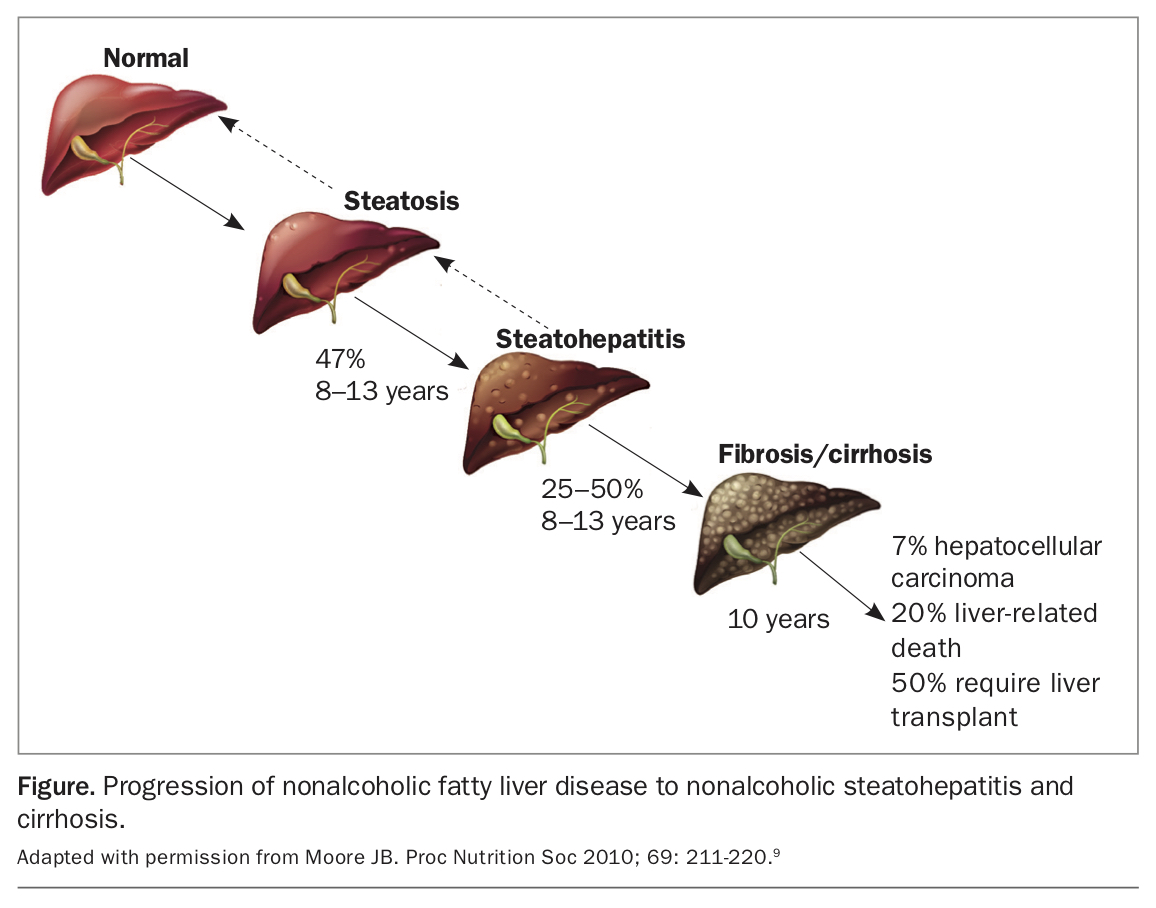{kind=link}
Previous data regarding NAFLD and mortality have been conflicting. The largest meta-analysis to date showed patients with NAFLD had increased all-cause mortality compared with those without NAFLD, and most deaths occurred due to cardiovascular disease.11
NAFLD and the metabolic syndrome
The metabolic syndrome is diagnosed in patients with at least three of the following five abnormalities: hypertension, elevated triglyceride level, low HDL cholesterol level, elevated fasting blood glucose level and central obesity.12 NAFLD and the metabolic syndrome are closely linked. The epidemiology and natural history of NAFLD is altered in patients with comorbidities from the metabolic syndrome. Further, patients with moderate to severe NAFLD are more likely to have the metabolic syndrome than the general population, with one study showing 18% of patients with NAFLD also had the metabolic syndrome.13 Therefore, NAFLD and the metabolic syndrome are bidirectionally linked and patients with one of these diagnoses should be regularly screened for the other.
NAFLD and type 2 diabetes
Patients with type 2 diabetes are about twice as likely to have concurrent NAFLD as people who do not have type 2 diabetes. A recent study showed a 56% prevalence of NAFLD in patients with type 2 diabetes.14 Rates of progression of NAFLD to NASH with advanced fibrosis are also higher in patients with type 2 diabetes.
NAFLD and obesity
The rising prevalence of NAFLD is associated with the obesity epidemic. The prevalence of NAFLD increases significantly with worsening obesity, and NAFLD is seen in up to 90% of patients who undergo bariatric surgery.15 Obesity appears to increase both all-cause and liver-specific mortality among patients with NAFLD.16
Differential diagnosis
NAFLD is the most common cause of mildly elevated ALT, AST and GGT levels among asymptomatic people in Australia, but primary care physicians play an important role in excluding relevant differential diagnoses. An accurate alcohol history is essential before a diagnosis of NAFLD can be considered. A complete drug history including complementary and alternative medicines should be taken.
We recommend testing all patients with suspected NAFLD for chronic hepatitis B and C infections, haemochromatosis and autoimmune liver diseases. Screening for other, rarer, causes of abnormal liver function test results such as Wilson’s disease or alpha-1 antitrypsin deficiency can be guided by the history, particularly by the family history. A summary of relevant investigations can be found in Table 1.
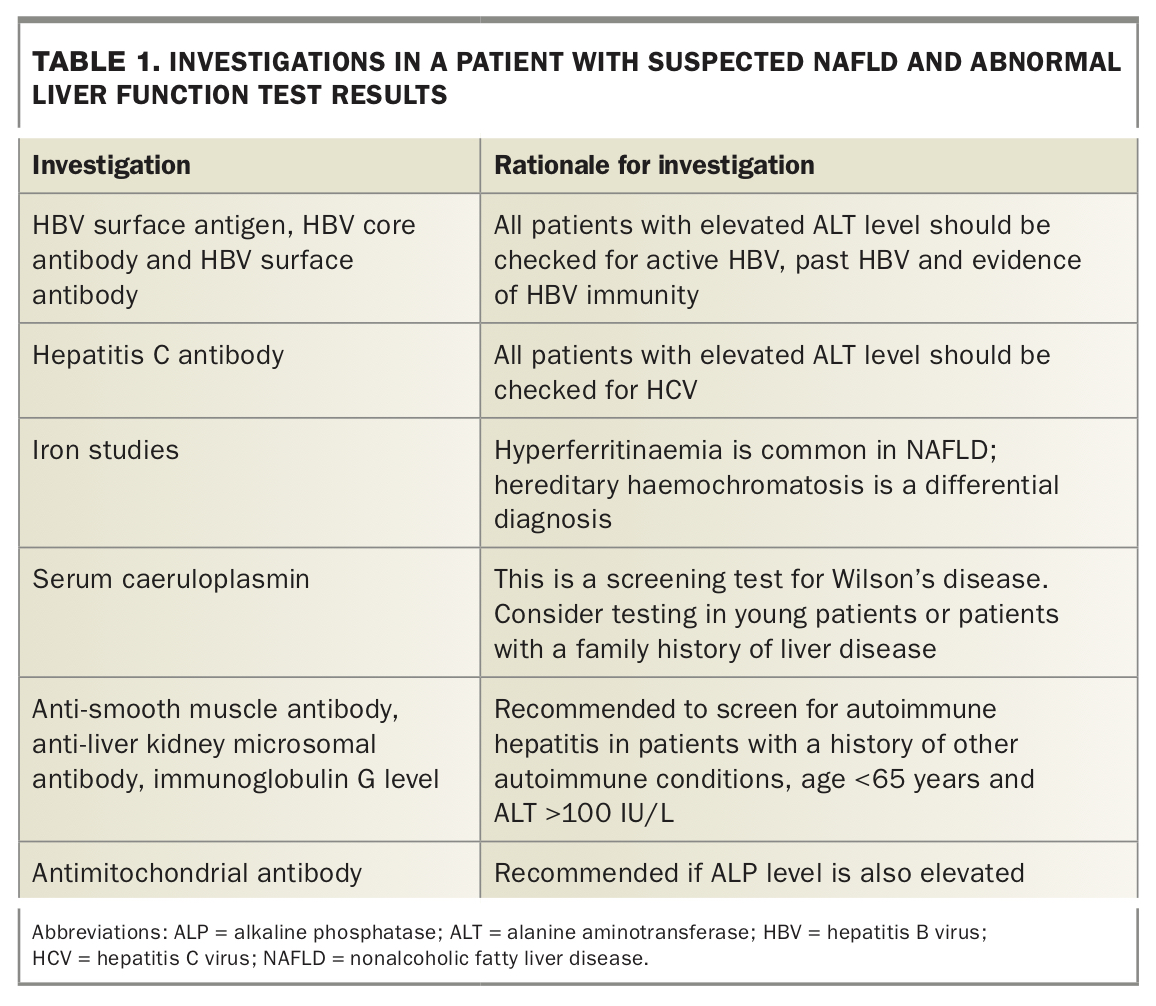{kind=link}
Chronic viral hepatitis
The most commonly missed alternative diagnosis causing mildly to moderately elevated liver function test results is chronic viral hepatitis (hepatitis B or C infection). Hepatitis B infection should be suspected in all patients in remote Aboriginal communities and those born in countries outside Australia where hepatitis B infection is common, such as Asia or Africa. Hepatitis C infection should be suspected in patients who use intravenous drugs or have a past history of intravenous drug use, have undergone a transfusion with blood products before the introduction of hepatitis C screening in 1990, have tattoos or piercings done in nonsterile conditions, as well as those who may have undergone nonsterile medical or dental procedures in countries where hepatitis C is more common.
Iron overload
Genetic haemochromatosis is an important, treatable differential diagnosis in asymptomatic patients with abnormal liver function test results. Presentation with other features of this condition such as diabetes, skin pigmentation or arthritis can increase clinical suspicion. However, patients with NAFLD commonly have hyperferritinaemia in the absence of haemochromatosis, and transferrin saturation levels greater than 45% can help to determine which patients need to have haemochromatosis genotyping performed.
Assessment of fibrosis and cirrhosis in NAFLD
Once a diagnosis of NAFLD is made, it is crucial to assess the fibrosis stage, as patients with advanced fibrosis or cirrhosis require screening for hepatocellular carcinoma and referral to a gastroenterologist. Liver biopsy is the gold standard for determining fibrosis stage but is invasive and not practical to perform in most patients with NAFLD. Well-validated methods can be used by the primary care physician to assess for advanced fibrosis and cirrhosis noninvasively, as outlined below.
Noninvasive fibrosis and cirrhosis assessment
Fibrosis and cirrhosis can be noninvasively assessed for in patients with NAFLD through clinical examination, blood results and imaging of the liver. These results can be used in a number of well-validated scoring systems to differentiate those patients at low risk of liver fibrosis who can be safely managed in the community from those with advanced fibrosis or cirrhosis who need to be referred for further assessment.
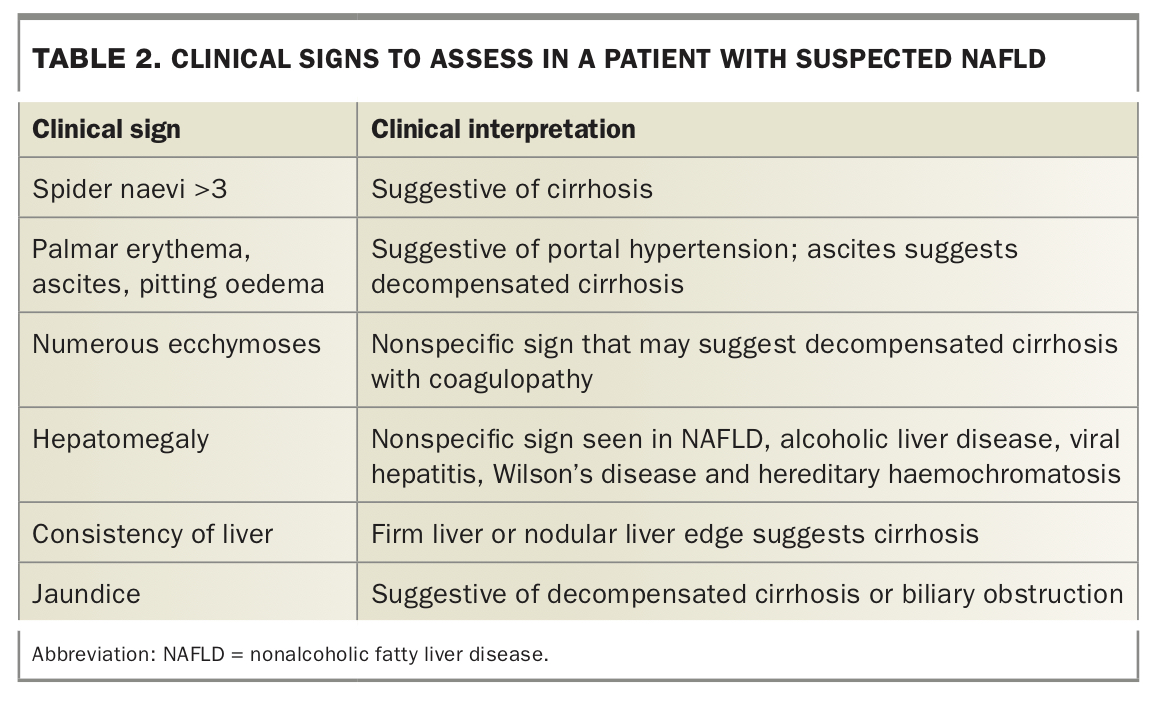
Examination
Patients with compensated and decompensated cirrhosis may have several clinical signs that can be elicited at the bedside, although the absence of such signs does not reliably exclude cirrhosis. Common clinical signs and their interpretation are summarised in Table 2.
{kind=link}
Noninvasive fibrosis scoring systems
Elevated levels of ALT, AST and GGT are common in patients with and without fibrosis or cirrhosis. No single blood test can assess fibrosis. However, numerous noninvasive scoring systems using bedside and blood tests can be used to assess for the presence of advanced fibrosis in patients with NAFLD. We recommend the use of either the NAFLD fibrosis score (NFS) or the AST to platelet ratio index (APRI) as these scores utilise commonly available variables and can be easily calculated with online calculators. Many patients fall into the ‘indeterminate’ range of one or both of these scores, and transient elastography can be used to stratify risk.
The NFS was designed and validated for noninvasive fibrosis assessment specifically in NAFLD patients. This score takes into account age, hyperglycaemia, body mass index, platelet count, albumin level and AST/ALT ratio. It can be calculated online at https://nafldscore.com. A score less than -1.455 excludes advanced fibrosis (F3 or F4) and a score greater than 0.676 suggests advanced fibrosis with high accuracy.17
As liver fibrosis progresses to cirrhosis, the platelet count falls owing to portal hypertension and the resulting splenic sequestration of platelets. Hence, the APRI can be used to predict the likelihood of fibrosis or cirrhosis. This is calculated easily by dividing the AST level (as a proportion of the upper limit of normal) by the platelet count (see https://www.hepatitisc.uw.edu/page/clinical-calculators/apri). The closer the APRI is to zero, the less likely it is that a patient has significant fibrosis. The higher the APRI is above 1, the more likely it is that a patient has established cirrhosis.
Transient elastography (Fibroscan)
Transient elastography, or Fibroscan, is an ultrasound-based technology now widely available in Australia. Fibroscan measures patients’ liver stiffness in kPA and provides an estimate of fibrosis, with higher values indicating more advanced fibrosis. Fibroscan readings have been validated against liver biopsy as a measure of fibrosis in NAFLD populations.18 Accurate assessment of fibrosis in primary care can be challenging, and we recommend that all patients with NAFLD undergo transient elastography for fibrosis assessment when the results would change management. Fibroscan readings may not be valid in morbidly obese patients and are not accurate when the standard deviation and interquartile range on the report are high.
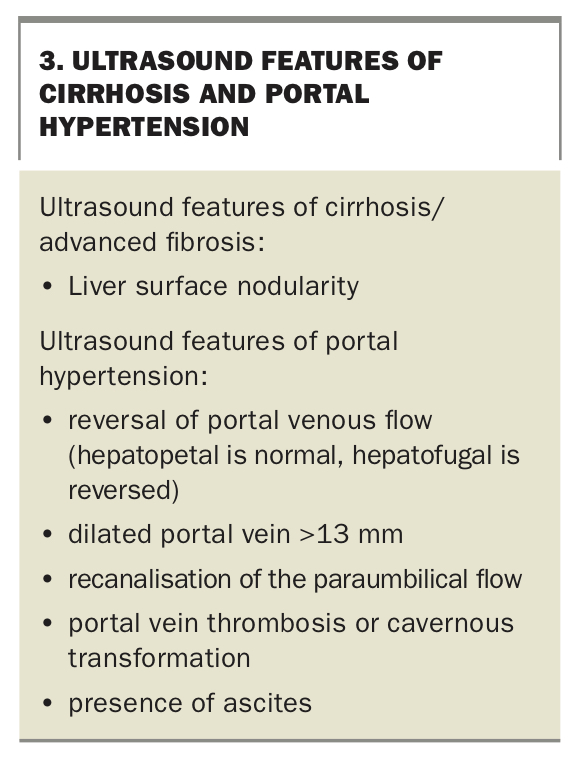
Ultrasonography of the liver is useful to detect steatosis but is unreliable in determining the presence of cirrhosis. A coarse and heterogenous appearance of the liver due to fatty infiltration can be difficult to distinguish from architectural change due to cirrhosis. Ultrasound features that are more specific to cirrhosis or portal hypertension are summarised in Box 3. Any patients found to have these features should be referred to a gastroenterologist for further assessment.
{kind=link}
Management of patients with NAFLD
An optimal, disease-modifying therapeutic agent for NAFLD would both reduce the level of steatohepatitis and prevent progression of or improve fibrosis. There is currently no approved, disease-modifying therapy for NAFLD. Multiple medications including statins and oral hypoglycaemic agents have been trialled for the treatment of NAFLD. These medications do not specifically improve patients’ NAFLD. However, as comorbidities from the metabolic syndrome worsen NAFLD, we recommend aggressive treatment of comorbidities.
Patients with cirrhosis from NAFLD should be managed in conjunction with a gastroenterologist. We discuss treatments that are of benefit in NAFLD patients below.
Weight loss
All patients with NAFLD and obesity should be counselled regarding weight loss. Numerous randomised controlled trials assessing the effects of weight loss on NAFLD have consistently shown clinically significant improvements in noninvasive biomarkers of disease severity but have not shown improvement in histological fibrosis.19 The benefits of weight loss for NAFLD appear after 5 to 10% of body weight loss is achieved. Weight loss through bariatric surgery reverses NAFLD in around two-thirds of patients, although it is not indicated for NAFLD alone.17
Exercise
Exercise therapy has been shown in numerous studies to improve noninvasive biomarkers of NAFLD and conditions related to the metabolic syndrome.20 Regular aerobic exercise of at least moderate intensity is ideal; however, the choice of exercise regimen should be tailored to individual patients based on their preference and physiological reserve.
Diet and lifestyle measures
Patients with NAFLD should be counselled to eat a balanced diet consisting of low glycaemic-index foods and food low in saturated fats. There is insufficient evidence to recommend a ‘best diet’ for patients with NAFLD, although the Mediterranean diet has shown promise in cross-sectional studies.21 It is unknown whether moderate alcohol consumption worsens NAFLD disease progression, but patients with NAFLD should be advised to avoid excessive alcohol consumption. There is evidence of decreased NAFLD risk in coffee drinkers, although there is insufficient evidence to recommend coffee consumption for the prevention of NAFLD.22
Diabetes and lipid management
We recommend aggressive diabetes and lipid management in patients with NAFLD. Most medications that are currently used for both type 2 diabetes mellitus and dyslipidaemia treatment have also been studied specifically in patients with NAFLD. These studies have reported improvements in liver biochemistry and steatosis, but no change in fibrosis.23 At present these medications should not be used specifically for NAFLD disease modification, but only if indicated as therapy for comorbid diabetes or dyslipidaemia.
Pharmacotherapy
A promising medication for NAFLD-treatment is obeticholic acid, which is a farnesoid X receptor agonist. A recent interim analysis of a phase 3 study showed histological improvement of NAFLD in patients treated with obeticholic acid compared to placebo.24 Phase 2 and 3 clinical trials are actively recruiting patients with NAFLD. Recruitment is generally limited to patients with elevated liver enzymes and evidence of fibrosis or well-compensated cirrhosis.
When to refer to a gastroenterologist
All patients with NAFLD and cirrhosis should be managed in conjunction with a gastroenterologist. We recommend referral to a gastroenterologist for all patients with NAFLD in whom fibrosis is suspected. A suggested approach to determining location of care is presented in the Flowchart. All patients with NAFLD who are reviewed in tertiary hospital liver clinics are considered for recruitment in NAFLD clinical trials, and patients with cirrhosis or advanced fibrosis are regularly reviewed for complications of their disease.
Conclusion
NAFLD encompasses a wide spectrum of clinical disease and is highly prevalent and under-recognised in Australia. Disease progression to fibrosis and cirrhosis occurs more commonly in patients with other features of the metabolic syndrome, and management of these risk factors forms the mainstay of treatment for NAFLD. For patients with NAFLD and elevated liver enzymes, noninvasive assessment of liver fibrosis is an important aspect of management that identifies patients who require referral to specialist care and those who should be screened for hepatocellular carcinoma. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.