Heavy menstrual bleeding. Tailoring treatment to the individual

In recent years, the number of women presenting with heavy menstrual bleeding has increased and the definitions relating to heavy menstrual bleeding have changed. A comprehensive approach to assessment and management is required to determine the severity of symptoms, differentiate between causes and tailor treatment options to the individual patient.
Heavy menstrual bleeding (HMB) was previously referred to as menorrhagia but has been renamed following the reclassification of the causes of abnormal uterine bleeding.1 The awareness among women and health professionals of the impact of HMB on both the individual and, potentially, the wider community has increased over recent years, with more patients presenting to GPs and gynaecologists with symptoms of heavy periods. Heavy menstruation interferes with normal daily life, leading to ill health and reduced productivity and income, and is the major cause of iron deficiency in women of reproductive age. Management of HMB requires informed choice and shared decision making between the individual and their health professional, taking into account the patient’s personal priorities and preferences. Any intervention should aim to improve quality of life rather than simply focusing on reducing the amount of blood lost. Guidelines and other helpful resources for managing HMB are provided in Box 1.
{kind=link}
Definition of HMB
HMB is defined as excessive menstrual bleeding that impacts on physical, social and emotional wellbeing, with a reduction in quality of life, with or without other symptoms.2 Traditionally, heavy menstruation was defined as a blood loss of greater than 80 mL, but further studies have shown this not always so for HMB to occur.3 HMB affects about 25% of reproductive aged women. Results of an Australian survey showed a significant increase in general practice consults for HMB over the last 16 years, with the highest presentation among women aged 35 to 44 years, followed by women aged 45 to 54 years and then those aged 12 to 17 years.4 HMB can present as both an acute or chronic disorder over the reproductive lifespan.
Causes of HMB
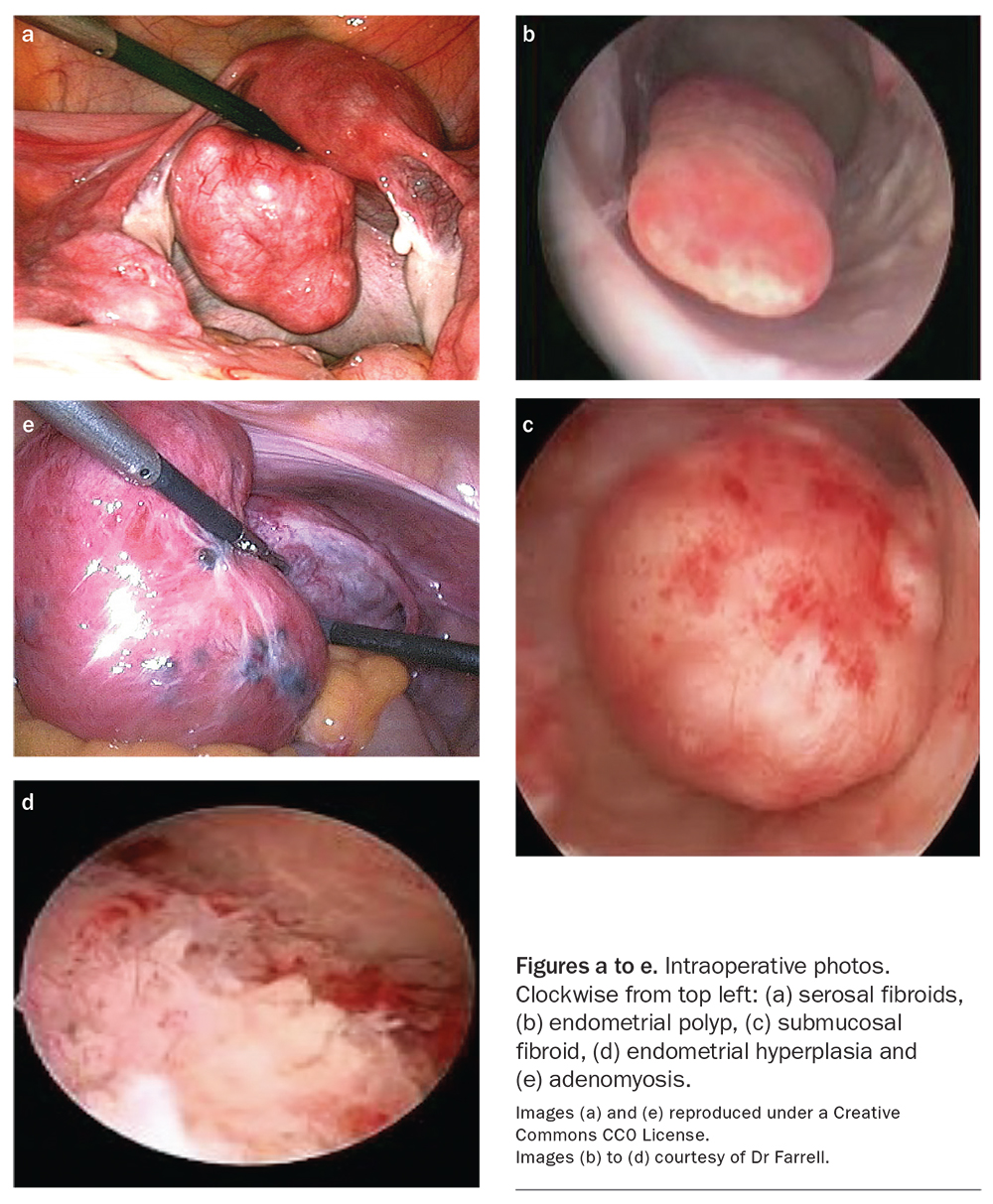
In many women (50 to 60%), no cause for HMB is found. Previously termed ‘dysfunctional uterine bleeding’, the causes of HMB are now thought to be related to mechanisms of excessive fibrinolytic and/or prostaglandin activity within the endometrium. Other important causes of HMB include uterine fibroids, endometrial polyps, adenomyosis, endometrial hyperplasia and gynaecological cancers (Figure). Non-structural causes include ovulatory bleeding, which is more common in the 30- to 40-year age group, and anovulatory bleeding. The latter is seen most commonly in the perimenopause and during the first two to three years after menarche in women with conditions such as polycystic ovary syndrome. Anovulatory HMB may be associated with endometrial hyperplasia and endometrial carcinoma. Bleeding disorders, such as Von Willebrand disease and platelet dysfunction disorders, may be the cause of HMB, especially in adolescents and women with persistent HMB since menarche. The PALM-COEIN classification system of causes of abnormal uterine bleeding, developed by the International Federation of Gynaecology and Obstetrics Working Group on Menstrual Disorders, is summarised in Box 2.
{kind=link}
{kind=link}
History
It is important to take a detailed history that distinguishes between a recent change in menstrual pattern and the persistence of heavy periods, often from menarche. A menstrual history should include:
- age of menarche
- age of onset of regular cycles
- cycle length and length of period
– the average menstrual cycle length is 28 days (range: 21 to 35 days)
– most women bleed for about four to five days each cycle - a measure of heaviness, determined by the size of period pad, tampon or period underwear and the frequency of changing them. A menstrual cup may give an accurate measure of blood loss over time
- passage of clots and their size, flooding through clothing or bedding, an inability to leave home on the heaviest days (menstrual scoring charts and pictograms may also be helpful)5
- any bleeding between periods (intermenstrual) or after penetrative sex (postcoital)
- pain, nausea, pelvic pressure or other associated symptoms
- bowel and bladder symptoms.
History should also include questioning on fatigue, dizziness, loss of energy, shortness of breath, palpitations and any reduction in exercise tolerance; these may be symptoms of iron deficiency. There should be an assessment of the impact of the HMB on the patient’s ability to carry out activities of normal daily living and the impact that it has on quality of life.
The factors that may affect treatment options should be determined. These include previous treatment and medications, comorbidities, current medications, including contraception, and previous medical history. The outcomes that a woman wishes to achieve from the management of her HMB should be determined, for example, some women find amenorrhoea undesirable.
Examination
Examination will depend on individual presentation and age. An abdominal examination may detect a suprapubic palpable mass consistent with uterine fibroids. Speculum examination is needed to exclude the presence of a cervical polyp, significant ectropion and cervical lesions. A bimanual examination is appropriate if a pelvic mass or pelvic inflammatory disease is suspected.
Investigations
Cervical screening should be up-to-date, and a co-test (human papilloma virus testing and liquid-based cytology) should be requested if any red flag symptoms are present, including intermenstrual or postcoital bleeding. A co-test is usually not indicated in most women presenting with vaginal discharge or dyspareunia but should be taken if there is unexplained persistent or blood-stained vaginal discharge.6
Other initial investigations will depend on the presentation from history and examination. Pregnancy should be excluded and iron deficiency (with or without anaemia) evaluated for. Iron deficiency is much more common than anaemia. Suggested initial investigations include:
- cervical screening test (if due) or co-test (if appropriate)
- full blood examination
- serum ferritin level
- pregnancy test
- thyroid stimulating hormone level (if a thyroid cause is suspected)
- testing for Von Willebrand disease and platelet dysfunction disorder (in patients who have had HMB since menarche)
- a transvaginal ultrasound scan (or a transabdominal ultrasound scan in adolescent patients) to exclude pelvic pathology. The ultrasound is more accurate when performed between days five and 10 of the menstrual cycle (at the end or immediately after menses), when the endometrium is thinner.
Subsequent investigations will depend on the results of initial testing but may include ovarian tumour markers, hormonal studies and further thyroid tests, such as thyroid function tests and thyroid autoantibodies.
Management
Initial management
Reducing blood loss and improving quality of life are the aims of initial management. Treatment should be started while investigations are being undertaken, except in the case of suspected malignancy when prompt referral to a gynaecologist or gynaecological oncologist is mandatory.
If the woman has acute heavy bleeding at the time of the initial consultation and has no contraindications, tranexamic acid should be started immediately; otherwise, it should be started on the heavy days of the next period. The usual dose of tranexamic acid is 1 g orally taken three to four times per day for a maximum of four to five days. Thrombosis is a rare risk.
Any systemic disease, including any bleeding disorder, should be treated accordingly, or patients referred on to the appropriate specialist for ongoing management. Iron deficiency is common in women with HMB. If the ferritin level is 30 mcg/L or less, with or without anaemia, daily oral iron supplementation should be started. If the ferritin remains low despite adequate oral iron therapy over 12 weeks, an infusion may be necessary. Referral to a gastroenterologist should be considered in cases of persistent low ferritin despite adequate iron replacement and treatment of the HMB to exclude other causes.
Once the results of initial investigations are known, the cause of HMB can often be determined. If investigations show an endometrial polyp, a submucosal fibroid or evidence of endometrial hyperplasia or carcinoma, prompt referral to a gynaecologist is needed for ongoing management.
Long-term management
Long-term management of HMB depends on the cause and can be further subdivided into medical and surgical options.
Medical management
The use of medical treatments further depends on whether the woman requires contraception.
Non-hormonal treatments
Tranexamic acid is an antifibrinolytic agent, which targets the over-activation of the fibrinolytic system that causes heavy bleeding. It inhibits the activation of plasminogen to plasmin, allowing clot formation. It reduces menstrual flow by about 50 to 60%. As a result of its short half-life, the prescribed dosage (1 g) is taken three to four times per day, only on the heavy days of the period, for up to four to five days. Side effects are infrequent but may include nausea. There is a small risk of thrombosis with the use of tranexamic acid and so its use should be avoided in women with a history of thromboembolism or coagulopathy. It is a suitable therapy for women wishing to get pregnant or who have experienced previous side effects with hormonal medications. Tranexamic acid can be used long term if it is effective in reducing menstrual loss.
NSAIDs have an anti-inflammatory effect on the endometrium by inhibiting the production of prostaglandins, thus reducing menstrual blood loss by 25 to 50%. Mefenamic acid has a similar effect of reduced menstrual blood loss and pain. These therapies are also suitable for women wishing to become pregnant or wanting to avoid any hormonal therapy side effects; however, they are not suitable in women with a history of stomach ulcers, NSAID-induced asthma or coagulopathy.
Hormonal treatments
Hormonal medications are the main treatments for HMB and may be considered if heavy bleeding persists after a few months of non-hormonal treatment or if preferred by the patient. Many hormonal therapies are contraceptive and therefore only suitable for women who do not wish to become pregnant. Hormonal therapies include:
- oral progestogens
- 52 mg levonorgestrel intrauterine system
- combined oral contraceptive pill or ring
- injectable progestogen.
Oral progestogens
Oral progestogens, such as norethisterone, may be used to reduce HMB and are usually prescribed from day five to 26 of the menstrual cycle in the dose of 5 mg three times per day. They are ineffective if used only in the luteal phase. Blood loss may be reduced by about 80%. They are often prescribed for the short-term management of HMB because of bothersome side effects, including breast tenderness, irregular bleeding or spotting, nausea and headache. They are not contraceptive, and their use is contraindicated in pregnancy and lactation. Because of its partial conversion to ethinyloestradiol, norethisterone may also potentially increase the risk of venous thromboembolism in some women.
Levonorgestrel intrauterine system (52 mg)
The 52 mg levonorgestrel intrauterine system (LNG IUS) (Mirena) has become the mainstay long-term treatment for HMB. It suppresses endometrial proliferation, leading to a thin endometrium and reducing menstrual flow by about 95% at one year. It is an effective treatment for HMB that is caused by anovulation, ovulatory bleeding, adenomyosis and HMB of unknown causes.
The 52 mg LNG-IUS is replaced every five years, is contraceptive and suitable for all ages. It also has a role in reducing HMB during perimenopause and is a suitable progestogen if oestrogen therapy is introduced in the management of menopausal symptoms. There is no indication for the use of the lower dose 19.5 mg LNG-IUS (Kyleena) in the management of HMB.
Counselling about potential side effects and the procedure itself before insertion will reduce concern. The main side effect is persistent vaginal bleeding for up to three to six months, which is usually light, but can be bothersome and cause anxiety if not discussed. Procedural complications, such as infection, expulsion, vasovagal episodes and perforation should also be discussed before insertion. Some women may experience a regular and lighter period and about 20% of women experience ongoing persistent bleeding because of a very thin fragile endometrium. Bloating, breast tenderness, mood changes, androgen side effects (e.g. hair loss) and ovarian cysts are less reported side effects.
The UK Medical Eligibility Criteria for Contraception (UKMEC) offers guidance on the safety of contraceptive choice for a number of medical conditions. The LNG-IUS is totally contraindicated (UKMEC 4) in pregnancy and in the presence of unexplained vaginal bleeding, intrauterine infection (including symptomatic sexually transmitted infections) and hormone sensitive cancers. An alternative, more suitable therapy is suggested in patients with severe decompensated liver disease and when the uterine cavity is distorted by fibroids or a congenital abnormality such as a significant bicornuate or septate uterus (UKMEC 3).
Combined oral contraceptive pill and ring
Combined oral contraceptives (COCs) contain both an oestrogen and progestogen, reduce blood loss in HMB by about 50% and create a predictable monthly bleeding pattern. Some women take the COC continuously or have a period every third cycle to reduce the frequency of periods and thus HMB. The combined vaginal contraceptive ring offers an alternative to women who are unable to tolerate oral contraception because of nausea or who have previously experienced significant breakthrough bleeding on oral contraception.
COCs and the vaginal ring are contraindicated (UKMEC 4) in women aged over 35 years who smoke 15 or more cigarettes per day; women who experience migraine with aura; women with a history of thromboembolism, thrombophilia or a known thrombotic mutation; women with current or recent breast cancer; women with antiphospholipid antibodies; or women with severe hypertension. COCs are relatively contraindicated (UKMEC 3) in those with a body mass index above 35 kg/m2 and women aged over 35 years who smoke less than 15 cigarettes per day.
The risks of this form of contraception include thromboembolism, cardiovascular and cerebrovascular events and some studies have shown an increased risk of breast cancer.
Injectable progestogen
Injectable medroxyprogesterone acetate (DMPA) can be used for HMB but is normally used as a long-acting contraceptive. It is administered every 12 weeks and can induce amenorrhoea in about 50% of cases in long-term users. Unfortunately, it may also result in bothersome breakthrough bleeding. DMPA results in anovulation and a suppression of oestrogen levels, which may cause significant bone loss in the long term, leading to osteopenia or osteoporosis.7
Progestogen-only contraceptive pill
Drospirenone 4 mg in a 24/4 regime is a progestogen-only oral contraception that suppresses ovulation. Its method of action is therefore similar to COCs. It is suitable for women who are unable to take the COC, such as women with a history of migraine with aura. Preliminary studies suggest that after nine months’ use there is significantly less bleeding on this pill compared with desogestrel. Additionally, this medication is able to induce amenorrhoea in some long-term users, although there is no evidence of a direct effect on HMB.8
Other hormonal therapies
There are other hormonal therapies that may be used to treat HMB but are not indicated for contraception. Gonadotrophin-releasing hormone agonists should only be considered for treatment in the short-term, if other treatments have failed and the patient rejects any surgical options. It is associated with ovarian suppression of oestrogen and progesterone, leading to menopause-like symptoms as side effects.
Selective progesterone receptor modulators are prescribed to reduce the size of large fibroids (greater than 3 cm) and have the advantage of reducing HMB and inhibiting ovulation without suppressing oestrogen levels.9 Liver function tests are usually done before treatment, as there have been cases of liver abnormalities leading to liver failure in some users.2
Surgical management
Surgical management of HMB is indicated when a trial of available medical treatments has failed or when it is the individual’s preference that a surgical solution is found. This requires appropriate referral to a gynaecologist. Management options will depend on the cause of the HMB and include the following.
- Endometrial polyps – usually managed by hysteroscopic removal (preferably by resection to reduce the risk of recurrence).
- Adenomyosis – usually managed conservatively when fertility is required, by the interim use of the 52 mg LNG IUS. When surgery is indicated, hysterectomy is the surgical treatment because of the breadth of the adenomyosis involvement throughout the myometrium.
- Fibroid – management depends on their size and position within the uterus, and suitable management options depend on the desire to retain fertility or personal choice. A submucosal fibroid within the uterine cavity is removed by hysteroscopic resection. Large fibroids that lead to an increase in the surface area of the uterine cavity are managed by either myomectomy or hysterectomy. Uterine artery embolisation is a form of treatment used to reduce fibroid size by occlusion of the uterine arteries.
- Endometrial hyperplasia or malignancy – requires immediate referral to a gynaecological oncologist for further management.
Surgical management options
Surgical options may be considered in cases where conservative medical treatment has failed or based on individual preference after there has been a comprehensive discussion of available alternative options. Surgical options in these cases include endometrial ablation and hysterectomy.
Endometrial ablation is a procedure to remove the endometrium by various techniques. First-generation techniques (e.g. roller ball ablation) have been compared with second-generation techniques (e.g. bipolar radiofrequency ablation). There appears to be no difference in achieving amenorrhoea; however, second-generation techniques have shorter operating times, do not require hysteroscopic visualisation and are able to be performed under local anaesthesia.10
Hysterectomy is an option if all treatments have failed, or if a woman specifically requests this option as a permanent solution. Hysterectomy may be total, with removal of the body of the uterus and cervix, or subtotal, with retention of the cervix. Hysterectomy with bilateral salpingectomy is usually recommended for benign causes, as removing the tubes reduces the risk of ovarian cancer. The ovaries are not removed. Most hysterectomies are performed laparoscopically but may also be performed vaginally if associated with uterine prolapse, or abdominally for a large fibroid uterus or malignancy.
Conclusion
HMB is the most common cause of iron deficiency in women and causes impaired quality of life and loss of productivity. Clinicians should ask women who present with general symptoms, such as tiredness, about their periods, as they may not realise that their periods are heavy. First-line treatment can be with tranexamic acid or NSAIDs while investigations to determine a cause are being undertaken. A range of hormonal therapies is available, of which the 52 mg LNG IUS is very effective. Treatment choice depends on the requirement for contraception, both short and long term. Women should be referred to a gynaecologist immediately if endometrial hyperplasia or malignancy is the possible cause of HMB. The choice of treatment is made together with the woman after the various options and their risks and benefits have been explained to her so that she is best able to make an informed decision. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.