Abdominal pain in children. An approach in general practice


Digestive diseases
Abdominal pain is a common yet infuriatingly nonspecific symptom in children presenting to GPs. Having a well-practised, thoughtful approach to diagnosis and investigation helps differentiate potentially serious conditions from the benign.
- Managing paediatric abdominal pain in general practice begins with a well-considered, confident diagnosis.
- Having an established approach to diagnosis allows a targeted evaluation within the short amount of time available during a consultation.
- Dangerous conditions should first be ruled out by screening for red flags.
- Investigations should be tailored towards confirming or ruling out diagnoses.
- GPs should not hesitate to seek another opinion; well-considered referrals and first-line investigations will facilitate prompt triaging.
Abdominal pain accounts for up to 5% of childhood consultations in family practice.1 GPs have the unenviable task of sorting through symptoms ranging from the sublime to the ridiculous to reach a diagnosis and ensure patients receive timely, appropriate care. Most difficulties arise when patients present for the first time, early in the evolution of disease.
In up to 90% of abdominal pain presentations, GPs suspect a nonorganic cause.1 However, it is often challenging to discriminate between organic and functional abdominal pain with confidence. It may be heartening to know that this problem is not exclusive to the family physician; subspecialty practitioners are often faced with similar feelings of consternation. Are symptoms being exaggerated? What if I miss a dangerous condition? Is there such a thing as overinvestigation?
It is helpful to have a well-considered strategy when dealing with abdominal pain. This article outlines a suggested approach to the diagnosis and investigation of abdominal pain in children.
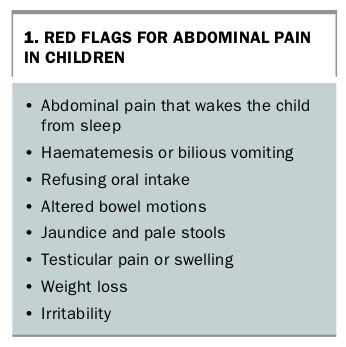
Are there red flag signs and symptoms?
Red flags are signposts for dangerous conditions not to be missed (Box 1). Presence of red flags should trigger further history taking and examination along the respective diagnostic pathways. This helps the physician determine the tempo for escalation, if required.
{kind=link}
What are the dangerous conditions not to be missed?
There are a handful of conditions for which children with abdominal pain should be screened to reduce the likelihood of missing a dangerous diagnosis. Although some common presentations (e.g. appendicitis) are easily recognised, other causes of abdominal pain may pose a diagnostic challenge, particularly in the early stages of illness.
Intestinal obstruction
Causes of intestinal obstruction in infants and young children include:
- volvulus and malrotation
- Hirschsprung’s disease
- Meckel’s diverticulum
- intussusception
- pyloric stenosis
- incarcerated hernia
- ileus secondary to sepsis or perforation.
- In older children, causes include:
- volvulus and malrotation
- incarcerated hernias
- strictures
- ileus secondary to sepsis or perforation.
Key red flags
The key red flags for intestinal obstruction are:
- vomiting
- reduced bowel output.
The textbook red flag for intestinal obstruction is bilious (dark green) vomiting. There are two main pitfalls to this. The first is that parents tend to describe most vomiting as bilious, without really understanding what this means. Parents should be asked what they mean by ‘bilious’; they may have photos of their child’s vomit on their smartphone.
The second problem is that the absence of bile-stained vomitus does not rule out subacute or partial obstruction; nor does it rule out gastric outlet obstruction (e.g. pyloric stenosis). Rather, it is the severity and persistence of vomiting, coupled with the GP’s clinical acumen in assessing other aspects (history, reduced oral intake and bowel output, dehydration and how unwell the child appears) that will help narrow the diagnosis. A conscientious evaluation with this in mind helps to rationalise investigations and referrals.
Significant haematemesis or any faeculent vomiting should prompt urgent referral to the emergency department.
Reduced bowel output does not always indicate constipation, particularly if the child has no notable history of constipation. Being specific about the timing and nature of reduced bowel output can avoid later re-evaluation.
Recommended investigations
If pyloric stenosis is suspected in an infant, an abdominal ultrasound scan should be performed.
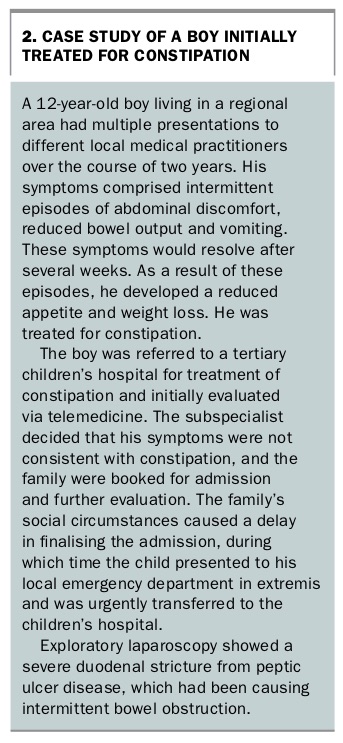
Urgent referral to the emergency department for investigation is indicated if intestinal obstruction, malrotation or volvulus is suspected (see case study in Box 2).
{kind=link}
Intussusception
Intussusception most often presents in infants and young children aged between three and 18 months, but it is also an important cause of acute intestinal obstruction in preschool and school-aged children.2 It occurs when a primary lead point (usually an enlarged mesenteric lymph node) causes telescoping of one segment of bowel into the immediately distal segment. If not reduced, the trapped bowel becomes ischaemic.
Key red flags
The key red flags for intussusception are:
- bloody stools or altered bowel habits
- vomiting
- irritability and pallor
- palpable mass.
The classic description of redcurrant jelly stool is a late sign. Although intussusception is, by definition, an acute obstruction, diarrhoea is common and often preceded by viral illness, making diagnosis tricky.
Recommended investigations
An urgent abdominal ultrasound scan is indicated if the child is clinically stable. If the child is unwell or there is a high level of suspicion, referral to a tertiary centre for further diagnostic and therapeutic investigations is appropriate.
Peritonitis
Peritonitis can be caused by several surgical diagnoses, including a perforated appendix, pancreatitis or trauma. Family physicians are usually efficient at detecting and referring for peritonitis.
Key red flags
The key red flags for peritonitis are:
- the child is septic and unwell
- increased abdominal pain with movement
- guarding or rigidity on abdominal palpation.
Foreign body
Diagnosis of a foreign body should be particularly considered in young children who are mobile and inquisitive but have not yet developed the skill to discriminate between food and nonfood items. A high index of suspicion is also needed for neurodevelopmentally delayed children.
The two scenarios involving foreign body ingestion that concern gastroenterologists the most are a button battery that becomes lodged in the oesophagus and the ingestion of magnets. A button battery impacted in the oesophagus causes severe mucosal injury and ongoing liquefaction necrosis. In severe cases, an oesophageal-aortic fistula can develop, which causes exsanguination and death.
A single small ingested magnet will usually pass through the entire gastrointestinal tract without trouble. The ingestion of more than one magnet or the ingestion of one magnet plus another ferromagnetic object becomes problematic. In these scenarios, the objects can become drawn together within the gastrointestinal tract, pinching mucosa between them and compromising perfusion. Left alone, the mucosa becomes ischaemic and a fistula forms between two sections of gut, leading to peritonitis and ischaemic bowel.
Other foreign objects that become impacted in the oesophagus can also cause pressure necrosis and perforation if not removed. Hence, patients with a foreign body impacted in the oesophagus should be promptly referred to the emergency department.
Key red flags
The key red flags for a foreign body are:
- drooling
- vomiting
- irritability
- retrosternal or abdominal pain
- poor oral intake
- gastrointestinal bleeding (late sign).
Recommended investigations
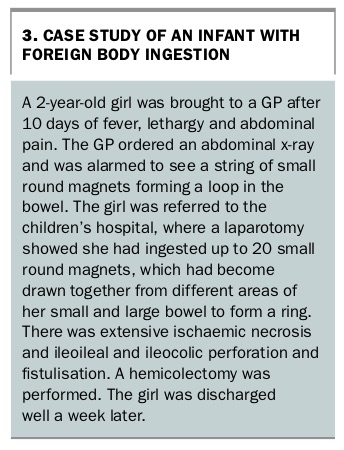
Any suspicion of a foreign body as a cause of abdominal pain should prompt plain chest and abdominal x-rays (see case study in Box 3).
{kind=link}
Inflammatory bowel disease
The incidence of paediatric inflammatory bowel disease (IBD) is on the rise worldwide, accounting for 20 to 25% of all patients with IBD. Five per cent of all patients with IBD are children aged under 10 years, while 1% of patients with IBD are aged less than two years (infantile IBD).3,4 It is thought that genetics play a prominent role in the pathophysiology of infantile IBD, and disease tends to be severe at diagnosis.
IBD is an important differential diagnosis to consider when a child presents with diarrhoea and abdominal pain of extended duration, particularly if there is concurrent iron deficiency and poor weight gain or weight loss. Symptoms may resolve between exacerbations, so establishing if there have been recent episodes of ‘gastroenteritis’ is helpful. Loose stools mixed with blood indicate colonic disease.
Key red flags
The key red flags for IBD are:
- diarrhoea
- blood in stools
- nocturnal stooling
- abdominal pain
- weight loss or growth failure.
Recommended investigations
Faecal calprotectin level has a sensitivity of up to 97% for predicting IBD, but levels can be elevated in other scenarios in young children, including infectious gastroenteritis, NSAID use and irritable bowel syndrome.5 Infectious gastroenteritis should be ruled out with a stool polymerase chain reaction test for viruses and bacteria. Blood tests (full blood count, electrolytes and liver function, C-reactive protein, iron studies) should be performed to correlate suspicions. Referral to a paediatric gastroenterologist is indicated.
Infection or sepsis
Abdominal pain and fever in the unwell infant or young child should prompt screening for infection (e.g. urinary tract infection) or sepsis.
Infectious hepatitis may manifest with some abdominal discomfort and generalised lethargy in older children. Examination may reveal a tender hepatomegaly from stretching of the liver capsule.
Older children may also complain of abdominal pain as a symptom of pneumonia, illustrating how a consultation for abdominal pain is never complete without an examination of other systems.
Key red flags
The key red flags for infection or sepsis are:
- lethargy
- irritability
- fever
- poor oral intake.
Recommended investigations
Recommended investigations include a urine culture and microscopy, full blood count, electrolytes and liver function test and inflammatory markers.
Other causes of acute abdominal pain
Other possible causes for an older child presenting with abdominal pain are:
- appendicitis
- pancreatitis
- testicular or ovarian torsion.
What are the common diagnoses for abdominal pain in children?
For infants or young children who do not present with red flags or who have had dangerous conditions ruled out through investigations, the diagnoses that should be considered are:
- reflux
- constipation.
For older children, diagnoses to consider are:
- reflux
- constipation
- coeliac disease
- abdominal pain-associated functional gastrointestinal disorders.
Reflux
Reflux and regurgitation are common throughout infancy, peaking at four months of age. In most cases, regurgitation resolves by 12 to 14 months of age.6
Although infant reflux is physiological and does not require further investigation, gastro-oesophageal reflux disease manifests as feed refusal, failure to thrive, oesophagitis, chronic cough or wheeze, recurrent otitis media and aspiration pneumonia. In these infants, a two- to four-week trial of hydrolysed or amino acid formula should be considered, or dairy elimination from the mother’s diet if the baby is still breastfeeding.7 If there is no improvement, referral to a paediatrician or a paediatric gastroenterologist would be appropriate.
The dilemma arises with infants who present with fussiness, poor sleep and vigorous crying, often interpreted as ‘reflux’ pain by distressed parents. The practitioner may feel pressured to investigate or medicate. However, there is no evidence to support empirical proton pump inhibitor therapy for gastro-oesophageal reflux disease in infants.7 Careful assessment for red flag symptoms and confirmation of appropriate growth and developmental milestones should reassure parents.
Reflux disease in older children presents as epigastric pain, heartburn and regurgitation. If proton pump inhibitors are ineffective, referral to a paediatric gastroenterologist for further investigation is indicated. Gastroenterologists do not encourage noninvasive screening for Helicobacter pylori infection, as most children with H. pylori infection are asymptomatic. If peptic ulcer disease is suspected, endoscopy is the investigation of choice.8
Constipation
Most constipation is functional, but children should always be screened for an organic cause, such as cow’s milk protein intolerance (e.g. history of atopy, early constipation, blood and mucus in stools), coeliac disease, hypothyroidism, Hirschsprung’s disease, sphincter achalasia, anteriorly placed anus or spinal cord anomalies. Faecal incontinence results when passive overflow occurs during chronic faecal retention.
Initial management of constipation lays the ground work for parental expectation. It should be explained to parents that management requires a consistent approach with the child at home, which begins with encouraging hydration, sitting on the toilet after meals and adopting correct posture on the toilet (feet flat on a stool or the floor, knees flexed). Osmotic laxatives (polyethylene glycol 3350 or, for infants, lactulose) are the most appropriate therapy to soften stools and encourage easy passage of bowel motions. Extra fibre is not recommended. School teachers should be informed so they can allow the child prompt access to the toilet to reduce the likelihood of accidental soiling.
Referral to a paediatrician is appropriate if adequate treatment fails or if the child remains dependent on medication after six months.
Recommended investigations
Screening investigations for coeliac or thyroid disease include coeliac serology, total IgA and thyroid function tests. Tertiary investigations may include lumbosacral magnetic resonance imaging, rectal biopsy to rule out Hirschsprung’s disease and colonic transit studies.
Coeliac disease
An Australian study estimated the prevalence of coeliac disease to be 1.2% in men and 1.9% in women.9 Common symptoms include either diarrhoea or constipation, abdominal pain, iron deficiency and poor weight gain after the introduction of gluten. There may be a family history of coeliac disease or autoimmune disease, such as type 1 diabetes, Hashimoto’s thyroiditis or Graves’ disease.
Recommended investigations
Coeliac serological testing, which in the first instance includes a total IgA and IgA anti-tissue transglutaminase antibodies, should be undertaken in children over the age of two years in whom coeliac disease is suspected.
In 2012, the European Society for Paediatric Gastroenterology, Hepatology and Nutrition recommended that if the IgA anti-tissue transglutaminase antibody titres are greater than 10 times the upper limit of normal, the patient can undergo a second serological test for IgA anti-endomysial antibodies and HLA typing. If the anti-endomysial antibody test result is positive, the diagnosis can be confirmed without the need to progress to gold-standard tissue biopsy.10 Any other combination of results requires a referral to a paediatric gastroenterologist. However, this practice has not been universally adopted in Australia, and practitioners should check with their tertiary hospital or preferred gastroenterologist.
First-degree relatives should undergo screening after diagnosis of an index patient.
Abdominal pain-associated functional gastrointestinal disorders
Much can be, and has been, written about functional gastrointestinal disorders. Functional abdominal pain disorders comprise:11
- functional dyspepsia
- irritable bowel syndrome
- abdominal migraine
- functional abdominal pain – not otherwise specified.
A diagnosis of an abdominal pain-associated functional gastrointestinal disorder is considered in children without any red flags after a thorough clinical evaluation. It is sensible to perform basic investigations to screen for occult organic disease and to review the patient over several follow-up appointments to ensure symptoms do not progress.
A multidisciplinary approach is required to ensure the family resumes a normal lifestyle, with the child back at school. Pharmacological therapy that the physician can trial includes antireflux and antispasmodic drugs. Nonpharmacological therapy includes cognitive behavioural therapy and family therapy with a psychologist, dietary modification with the help of a dietitian, probiotics and gut-directed hypnotherapy. Referral to a paediatrician or paediatric gastroenterologist is appropriate if there are concerns about an organic cause or if the child fails to make progress with treatment.
Recommended investigations
Investigations for functional abdominal pain disorders include a full blood count, C-reactive protein level, electrolytes and liver function test, iron studies, faecal calprotectin level and stool polymerase chain reaction screening for viruses and bacteria.
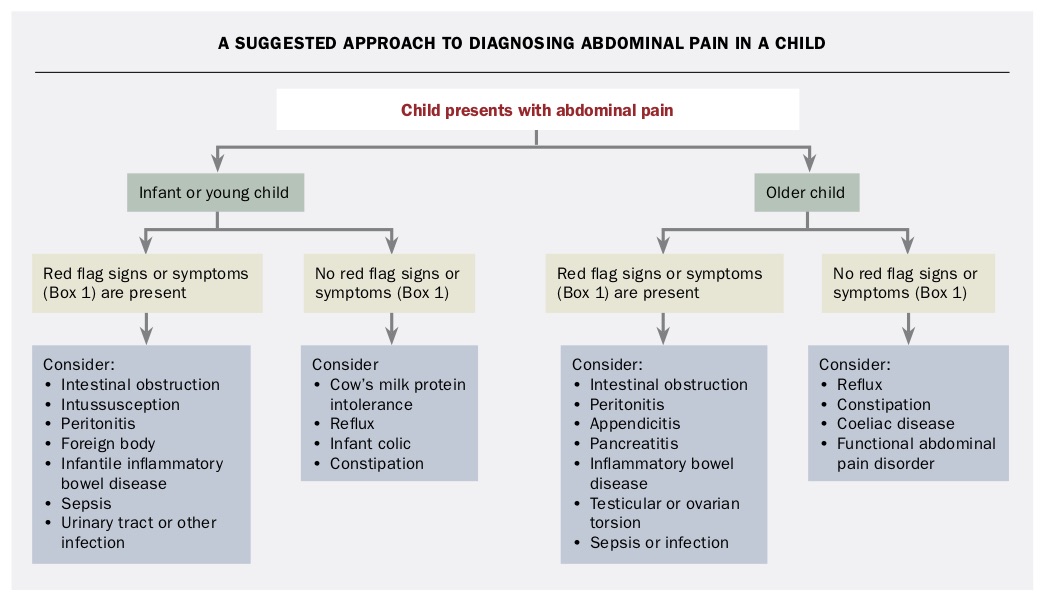
A suggested approach to diagnosing abdominal pain in children is shown in the Flowchart.
{kind=link}
Conclusion
The diagnosis and management of abdominal pain can confound even the most experienced of specialists, and GPs should never hesitate to seek a second (or third!) opinion. No practitioner need practise in isolation; even doctors in the most remote locations have the option of using telemedicine, and help is only a phone consultation away. Referrals that demonstrate a considered, sensible approach, with relevant first-line investigations and honest enquiries, will always be well received by paediatricians and other specialists. MT