Medical termination of pregnancy: the role of the GP

Women's health
With the PBS listing of medications for medical termination of pregnancy, there are likely to be increasing numbers of women requesting access to GP-led medical abortion care. GPs should be aware of the options for the management of an unintended pregnancy and possible post-termination complications and follow-up care.
In many countries, management of an unintended pregnancy is incorporated into primary health care. In Australia, GPs have often been bypassed in this process because most pregnancy terminations take place in private clinics where a referral is not required. However, with the PBS listing of medications for the medical termination of pregnancy (MTOP), GPs may see an increase in the number of women requesting access to GP-led management of an unintended pregnancy or post-termination follow up.
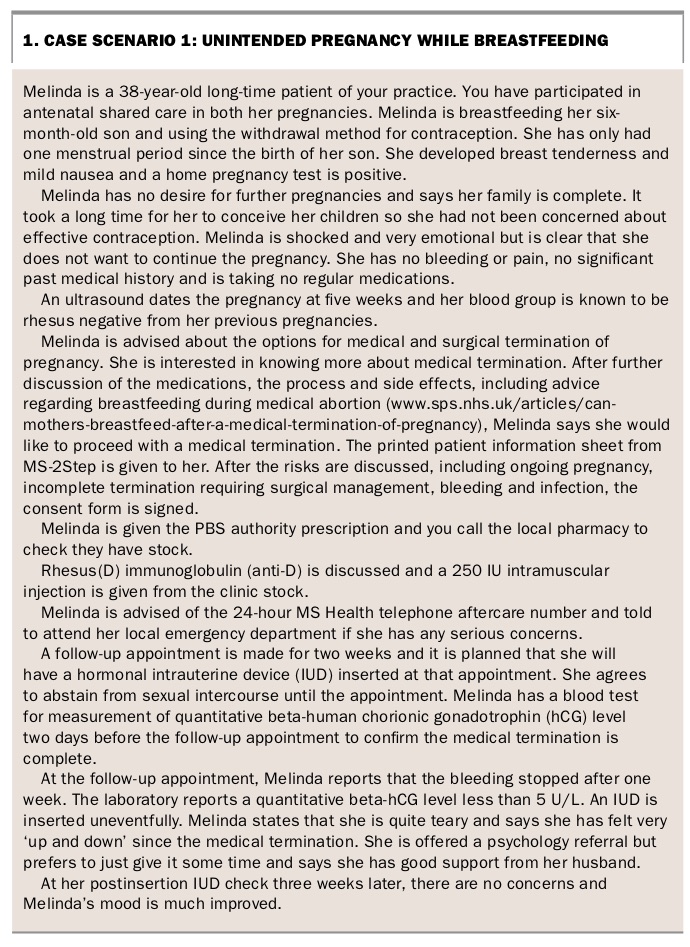
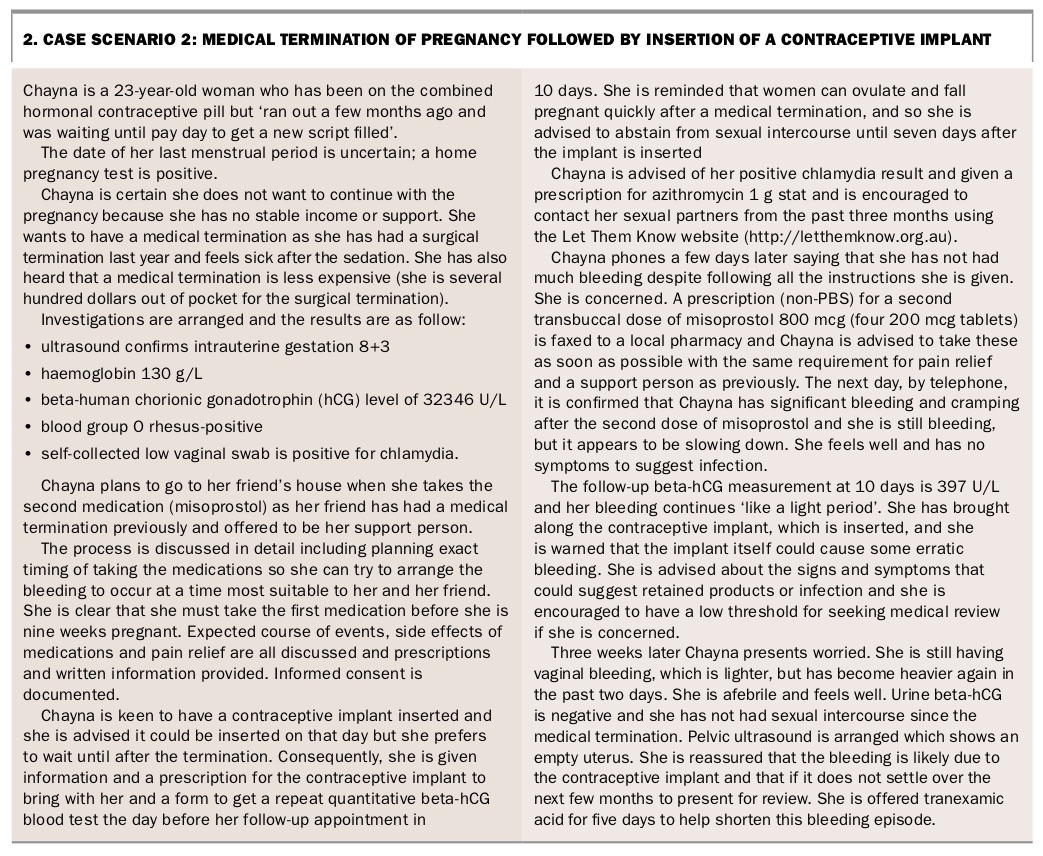
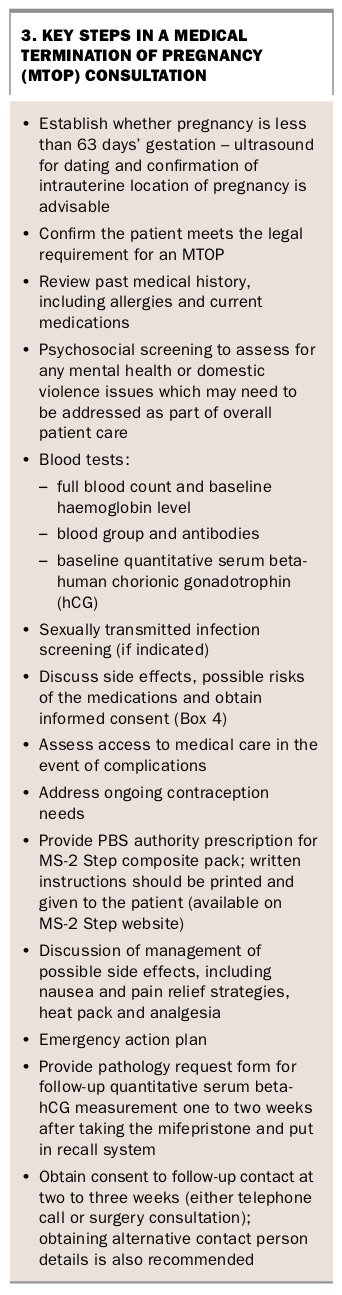
In most states of Australia, nonprocedural GPs are able to provide MTOP after completion of online training through the MS-2 Step program (www.ms2step.com.au). The benefits of GP involvement in the provision of MTOP services are significant and include counselling and post-termination contraception advice. Some example case scenarios are given in Box 1 and Box 2. Key steps in an MTOP consultation are outlined in Box 3.
{kind=link}
{kind=link}
{kind=link}
Pre-termination counselling
For most women, the decision to terminate a pregnancy does not require intensive counselling; many have come to a decision themselves before seeing a healthcare professional.1 However, some women experiencing an unintended pregnancy may require significant emotional support and counselling. The involvement of a GP is important because they are well placed to discuss available options, to facilitate referral to an appropriate social worker or psychologist if required, provide information on the steps involved in continuing with antenatal care or adoption, or the process of terminating the pregnancy by medical or surgical means.
There are several excellent resources available to GPs to assist with counselling a woman with an unintended pregnancy, including Children by Choice (www.childrenbychoice.org.au) and the Pregnancy Options booklet from Family Planning NSW (www.fpnsw.org.au). Training in nondirective pregnancy counselling is available online through RACGP GP learning (www.racgp.org.au/education/courses/activitylist/activity/?id=56276).
Process for the provision of medical termination of pregnancy
Medical termination is a two-step process performed for women with a pregnancy of up to 63 days’ (nine weeks’) gestation using one tablet of mifepristone 200 mg orally, followed 36 to 48 hours later by four 200 mcg tablets of misoprostol:
- Mifepristone is a synthetic steroid. It is a competitive progesterone receptor antagonist blocking the effects of progesterone thereby destabilising a pregnancy and making the myometrium more sensitive to prostaglandins that induce uterine contractions.
- Misoprostol is a synthetic prostaglandin E1 analogue. It induces contractions in the smooth muscles of the myometrium and stimulates the cervix to relax, leading to the evacuation of the uterine contents. It is considered teratogenic because it has been associated with fetal limb abnormalities.2,3
The buccal route of administration of misoprostol has been shown to be more effective than oral dosing, especially for a pregnancy with a gestational age of more than 49 days.4
Used buccally, the average time for commencement of contractions is 40 minutes; sustained contractions last about 90 minutes and the peak activity is contained within five hours after administration.
Contraindications
It is important to exclude the following contraindications to MTOP:
- allergy to mifepristone, misoprostol, prostaglandin or pharmaceutical constituents
- current ectopic pregnancy or pregnancy of unknown location
- pregnancy with a gestational age of more than 63 days
- intrauterine device (IUD) in situ (the IUD must be removed before the MTOP)
- severe uncontrolled asthma
- significant bleeding risk due to an inherited disorder or anticoagulant therapy
- chronic adrenal failure, including iatrogenic adrenal failure from long-term current corticosteroid therapy
- inherited porphyria.
Caution is recommended in women older than 35 years of age who smoke 15 or more cigarettes daily (these women were generally excluded from clinical trials).
Breastfeeding and MTOP
The manufacturer of MS-2 Step does not recommend its use in women who are breastfeeding. However, recently updated UK Medicines Information suggests that breastfeeding does not need to be interrupted with mifepristone or misoprostol use, but that breastfeeding infants should be monitored for gastrointestinal symptoms.1,5,6
Initial assessment
Accurate dating of the pregnancy is crucial because MS-2 Step for medical abortion is only licensed in Australia for a pregnancy of up to 63 days’ gestation. Ultrasound dating is generally recommended, which also has the important benefit of confirming the intrauterine location of the gestational sac. The possibility of an ectopic pregnancy should always be considered. Importantly, mifepristone and misoprostol are not indicated for the management of ectopic pregnancy and referral for urgent specialist care is required.
Quantitative measurement of beta-human chorionic gonadotrophin (hCG) levels is performed initially to correlate with ultrasound findings and is often repeated to confirm a successful MTOP. A high beta-hCG level with no intrauterine fetal pole on ultrasound would raise concern of an ectopic pregnancy and should be discussed with a specialist. Repeat measurement of quantitative beta-hCG level showing a decrease of more than 80% at seven to 10 days after taking mifepristone suggests the termination process has been completed. Initial assessment of haemoglobin is also recommended to detect anaemia because this may make MTOP unsafe.
As with any pregnancy, establishing the rhesus status of the woman is important. MTOP is considered a potentially sensitising event and all rhesus (Rh)-negative women should be offered Rh(D) immunoglobulin (anti-D) to prevent the possibility of haemolytic disease of the newborn in subsequent pregnancies.
Anti-D is a pooled human blood product and the Australian Red Cross Blood Service controls stock in Australia. GPs can request to become an approved health provider and order a small supply to have on hand to administer to appropriate Rh-negative women at the time of prescribing medications for MTOP. The Australian Red Cross Blood Service has an excellent website with useful resources, such as information brochures for women on anti-D and consent and refusal forms (https://transfusion.com.au/resource).
Legislation and consent
At the initial visit there is a substantial amount of information that needs to be discussed, and the involvement of a practice nurse can be an effective model of care. The prescribing doctor must assess the patient and ensure she meets the legal requirement for MTOP in the state or territory in which she resides. Further helpful information regarding abortion legislation can be found on the Children by Choice website (www.childrenbychoice.org.au/factsandfigures/australianabortionlawandpractice).
The possibility of an incomplete or unsuccessful termination must be discussed, as well as the risks of heavy bleeding and infection. Although most women who choose an MTOP wish to avoid a surgical procedure they must understand that in a small number of cases a subsequent surgical intervention is required to manage heavy bleeding or an ongoing pregnancy. A signed record of informed consent should be kept in the patient’s file (Box 4).
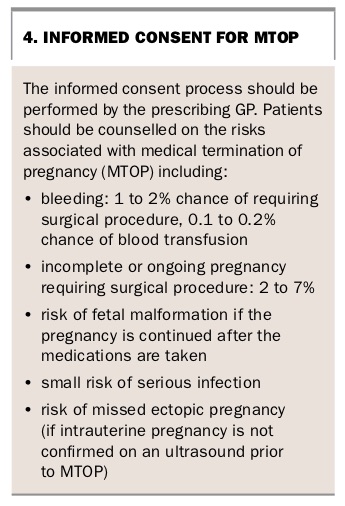{kind=link}
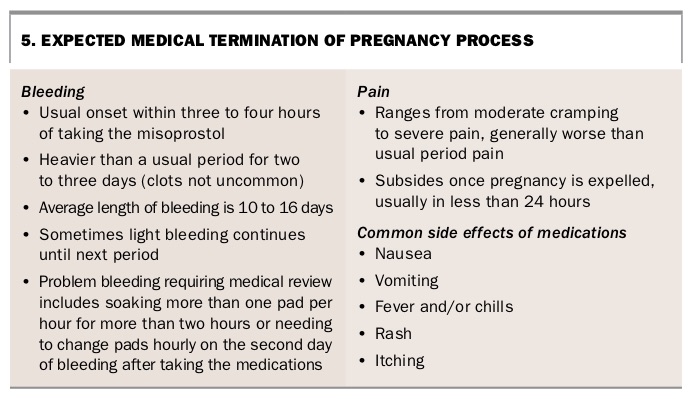
It is also important that written instructions are provided regarding how and when to take the medications, the expected course of events and when to seek medical support (Box 5). A consent form and patient information brochure for GPs to use are accessible on the MS-2 Step website.
{kind=link}
Prescribing the medications
The medications for MTOP are available as ‘MS-2 Step composite pack’, available on PBS Authority prescription when the prescribing GP has completed online training and is registered with the MS-2 Step program. The dispensing pharmacy must also be registered as an authorised dispenser of MS-2 Step.
Patients should receive clear, written instructions on managing expected pain and bleeding. It is recommended to take ibuprofen (or another NSAID) at least 20 minutes before taking the misoprostol (step 2 medication) and a paracetamol/codeine combination medication should be prescribed as this is usually required. Prescription for an antiemetic, such as metoclopramide or ondansetron, is also advisable in case significant nausea or vomiting is experienced as a side effect of the misoprostol. It is important not to understate the expected pain and other effects of the medications so that women can be well prepared to manage these at home.
To decrease the risk of infection, advice should be given to not use tampons or go swimming, and to avoid sexual intercourse for seven days after bleeding starts.
Cost
Financial issues can be a barrier for many women accessing termination of pregnancy, and the costs involved vary widely from clinic to clinic. For GPs providing MTOP services it is useful to list their MTOP consultation fees on the practice website or have the receptionist provide these to the patient at the time of booking.
There is currently no Medicare item number for the provision of MTOP services and so a timed consultation item number is appropriate. If the woman holds a Medicare card, the MS-2 Step medications are covered on the PBS as a single prescription.
Assistance and support
It is important for the patient to understand that a medical abortion takes place in her own home so the presence of a responsible support person is important in case she experiences more bleeding or pain than expected. Patients should be advised to have someone else available to care for young children. MTOP is not recommended in women with restricted access to emergency care due to travel or remote location in the two weeks following mifepristone administration in case of complications.
MS Health provides a 24-hour nurse aftercare helpline (1300 515 883) and all patients should be given this number to contact if they have any questions or concerns in case the prescribing GP is not available. Occasionally patients may need to seek medical care from an emergency department or after-hours medical service during the MTOP process. As this is a relatively new area of practice in Australia, it can be helpful if the patient has printed information about the process to show to medical staff.
Post-termination follow up
Follow up must occur to confirm that the MTOP process has been completed. The MS-2 Step composite pack medication comes with a ‘black box warning’ for medical review within 14 to 21 days. There are several recognised ways to confirm completion of an MTOP:
- clinical history of expulsion of products of conception followed by a resolution of bleeding and pregnancy symptoms
- a follow-up ultrasound showing an empty uterus
- a decreased quantitative beta-hCG level of more than 80% from seven days after the mifepristone.
The method of confirmation of completion and follow up must be agreed and documented in the patient file at the time of prescribing. Many prescribers use a quantitative beta-hCG test for follow-up assessment.
Women may experience a range of emotions following an MTOP including grief, sadness, anger, relief and guilt. However, there is no good evidence to show that women experience long-term adverse mental health outcomes following a pregnancy termination.7
Patients should be advised that fertility returns rapidly after termination of an unintended pregnancy. Ovulation has been documented as early as eight days post-MTOP, so discussion and provision of contraception is important at the time of providing MS-2 Step.8 Oral contraception should be commenced within five days of taking misoprostol and will be effective immediately. A contraceptive implant can be inserted on the day of the initial visit, before the MTOP medications have been taken, or after the process is complete. It will be effective immediately if inserted within five days of misoprostol administration. IUD insertion should be performed when there has been confirmation of complete termination of pregnancy; generally two to three weeks post-MTOP is appropriate.9
Conclusion
With the PBS listing of medications for MTOP, there are likely to be increasing numbers of women requesting access to GP-led medical abortion care. GPs may choose to undertake training to become providers of medical abortion. All GPs should be aware of the options for the management of an unintended pregnancy and possible post-termination complications and follow-up care. In the general practice setting, teamwork is the key to providing safe and successful MTOP outcomes for patients. The multidisciplinary team can include the GP, practice reception staff, practice nurse and local pharmacist, and nonroutine/emergency care providers such as the local public hospital emergency department or early pregnancy assessment clinic, private gynaecologist or local surgical termination provider. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.