Interpersonal psychotherapy: a time-limited treatment for depression

Depression
Psychotherapy
Interpersonal psychotherapy (IPT) is a brief intervention for patients presenting with depression and related disorders. It is supported by an evidence base comparable to that for cognitive behavioural therapy. GPs may find it useful to apply IPT strategies in their own practice or to refer patients for IPT.
General practitioners are confronted each day with patients with depression and related disorders as either their primary presentation or secondary to a physical complaint. Interpersonal psychotherapy (IPT) is a time-limited intervention with a strong evidence base for an array of psychological difficulties. Although it may not be feasible for most GPs to conduct an entire course of IPT, they may find that employing individual elements of IPT helps them manage patients with psychological distress. IPT strategies such as the ‘holistic assessment protocol’, ‘closeness circles’, ‘timeline’ and ‘consideration of the problem area’ may help them understand these patients, provide strategies to assist them and potentially inform referrals to psychologists and psychiatrists.
What is interpersonal therapy?
IPT is a well-established treatment for a range of psychological disorders. It was originally developed by Klerman and colleagues in 1984 to manage depressive disorder in adults.1 It has since been adapted for adolescents with depression and for adults and adolescents with bipolar disorder, mixed anxiety and depression, eating disorders, post-traumatic stress disorder, perinatal depression and other presentations. In patients with moderate- to-severe depression, IPT may be used as an adjunct to appropriate medication.
The effectiveness of IPT is supported by an impressive empirical base, equal to that for cognitive behavioural therapy (CBT).2-4 Like CBT, IPT is supported by Medicare under the Better Access to Mental Health Care initiative for up to 10 sessions per calendar year.
IPT is grounded in attachment theory, developed by John Bowlby, who proposed that humans have an instinctual drive to form relationships, a drive necessary for survival.5 According to Bowlby, we function best when attachment needs are met, and we are left vulnerable to distress or even psychiatric symptoms when these needs are not met. IPT is similarly based on the assumption that, irrespective of the underlying cause of depression, depressive symptoms are inextricably linked with interpersonal difficulties. When people become depressed, their depression impacts on relationships with people who matter, and these ruptured relationships feed and perpetuate their symptoms.
How is interpersonal therapy structured?
The goals of IPT are to decrease symptoms of depression by enhancing patients’ communication skills in significant relationships and by improving the accessibility and structure of their social support networks. IPT is a short-term treatment, typically delivered over 10 to 16 sessions. The notion of an endpoint drives both the patient and therapist to work more rapidly on resolving symptoms and improving interpersonal skills.
The first step of IPT is a comprehensive assessment interview that canvasses how the patient’s biological, psychological, social, cultural and spiritual domains interact to shape their mental health profile (Flowchart 1). The assessment is followed by acute treatment, divided into three phases – initial, middle and conclusion phases – and then maintenance treatment.
During the assessment process and the three phases of acute treatment, the therapist aims to assume the role of transitory attachment figure. This stance shapes the nature of the therapeutic dyad for the remainder of acute treatment. It provides a relationship environment in which the patient will feel safe enough to learn and experiment with new patterns of interpersonal processes that will contribute to more effective attachment-seeking behaviours and associated symptom resolution.
The steps of IPT are illustrated by the case scenario of Jane, a patient who presents with depression (Box).
{kind=link}
Acute treatment phases
Initial phase – interpersonal inventory
The initial phase of acute treatment comprises one to four sessions, held as close to weekly as possible. During the initial phase, the therapist explores the patient’s interpersonal world via the interpersonal inventory, which comprises three steps.
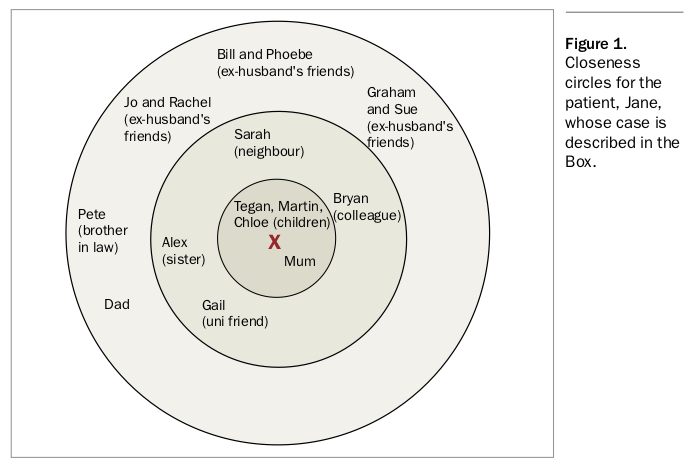
Closeness circles
The first step of the interpersonal inventory is a strategy to map the patient’s interpersonal world. The patient is presented with a series of three concentric circles with a cross representing themselves in the centre. The patient is asked to put the names of those closest to them in the inner circle. The people the patient feels next closest to are placed in the next-to-inner circle, and finally those who are more distant in the outer circle (Figure 1).
{kind=link}
The therapist and patient spend some time discussing these relationships. The focus is on, for example:
- who provides nurture, guidance, trust, fun and so forth
- satisfactory and unsatisfactory aspects of these relationships
- changes that have occurred since the depression began
- how the circles will look when the depression has lifted
- any changes the patient might like to make.
The closeness circles are referred to often during the course of therapy and become a focus of therapy. They help patients track changes in their meaningful relationships and become aware of the two-way association between having their attachment needs met more effectively and changes in their depressive symptoms. This process facilitates discussion of specific relationships, how they might change, and individuals to whom the patient might turn for support and care of various kinds.
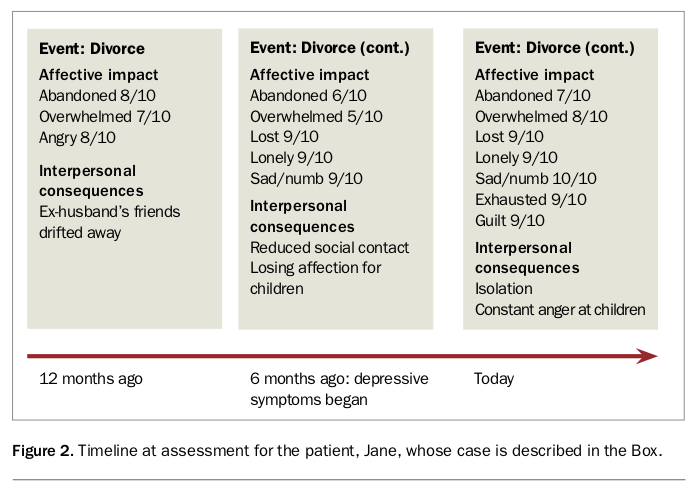
Timeline
The second step of the interpersonal inventory involves placing the patient’s symptoms in a timeframe. For this, a timeline is used to record life events that occurred in the months before the onset of symptoms. The affective impact of these events and their interpersonal consequences are explored (Figure 2).
{kind=link}
Consideration of the problem area
The third step represents a major departure from other therapeutic interventions. It consists of the therapist and patient collaboratively identifying which of four problem areas is most closely associated with the patient’s distress: complex grief, interpersonal disputes, role transitions or interpersonal gaps.
Complex grief is identified when the patient’s distress is most closely linked to significant loss, usually where this loss has not been sufficiently processed. The loss may be a death, but other examples include loss of a limb, a job, a pet or a relationship. Often the patient has not had the opportunity to grieve the loss, and the unresolved grief has progressed into depression or other symptoms.
Interpersonal disputes are identified as the problem area when unresolved conflict dominates the clinical picture. The crucial feature of interpersonal disputes is that the patient feels ‘stuck’, unable to move because of intransigence. The disputes are usually between the patient and people who matter in their interpersonal world, including between parent and child, spouse and spouse, or employer and employee. Often unmet expectations about others feature in this problem area. Dispute leads to distress, and with no end in sight the distress progresses to symptoms.
Role transitions occur when the patient takes on a new role in life that causes them significant distress. Examples include divorce, retirement, having children, starting a new job, becoming a single parent, leaving home to begin university, finishing university and loss of health. When patients lack sufficient psychosocial support, these changes can precipitate debilitating stress that may progress into disorders such as depression or anxiety. Role transitions are usually accompanied by ambivalence about the new role, grief about the loss of the old role, loss of social support associated with the old role, and anxiety due to lack of familiarity with the new role.
Interpersonal gaps refer to a lack of social and communication skills that impairs the conduct of interpersonal relationships. Patients with interpersonal gaps lack the skills to initiate and maintain relationships but simultaneously crave relationships and become depressed or anxious within the context of rejection and loneliness. If this problem area is identified as central to the depression then the therapist will help the patient develop new relationship strategies that will reduce the likelihood of rejection. This involves modelling new behaviours, rehearsing in session, the patient practising with ‘safe others’ outside of therapy, then analysis and review of the patient’s application of these strategies.
After the problem area has been identified, the therapist emphasises the link between the problem area and symptoms. The therapist explains that as the problem area becomes the focus in therapy, the symptoms will begin to resolve.
Middle phase
The middle phase of acute treatment comprises four to eight sessions, held as close to weekly as possible. In this phase, the therapist and patient work together to resolve the problem area identified in the initial phase. The therapist uses strategies relevant to the particular problem area. For example, this may include:
- for complex grief, helping patients effectively grieve the loss and connect to their new life without the lost person or object
- for interpersonal disputes, promoting skills and insight in understanding and resolving conflict
- for role transition, helping patients to disconnect from the old role (including mourning the loss of the old role) and then to develop interpersonal skills relevant to managing the new role
- for interpersonal gaps, developing social and interpersonal skills relevant to initiating and maintaining relationships.
The therapist strives to develop a safe and accepting relationship with the patient that will provide an opportunity for the patient to identify, explore and experiment with interpersonal processes relevant to their problem area, before using these processes outside the therapy room.
Conclusion phase
The conclusion phase of acute treatment comprises one to four sessions, spread over eight to 12 weeks. The aims of this phase of treatment are:
- to help the patient internalise and generalise the gains made in the middle phase
- for the therapist to step back from the role of transitory attachment figure and encourage the patient to identify individuals from their closeness circle who may fulfil elements of this role
- to assess the requirements of maintenance treatment.
The focus remains on the problem area addressed in the middle phase. Interpersonal incidents from the patient’s world outside therapy are analysed for effectiveness in moving towards independent functioning.
Maintenance treatment
The maintenance treatment phase of IPT is negotiated with the patient and usually involves sessions once every two to three months. The aim of this phase is to prevent relapse. Sessions are similar to those in the conclusion of the acute treatment phase, maintaining the focus on the identified problem area and troubleshooting any interpersonal difficulties that may arise.
Maintenance treatment in IPT has significant parallels with a GP model of care, in which short-term treatment for an acute problem is provided until it is resolved, then maintenance treatment is provided as needed. The relationship with the therapist is ongoing; the patient is welcome to return if another acute problem arises. In that sense, IPT can be viewed as a modular approach to therapy, as described in Flowchart 2.
After the maintenance treatment phase, therapy concludes. The patient is encouraged to be vigilant for interpersonal stressors that might trigger a return of symptoms.
Conclusion
IPT provides GPs with strategies that may be directly applicable to patient care. In addition, referring patients to an IPT practitioner can provide a time-limited therapy whose effectiveness is supported by an evidence base for patients with depression and related disorders. To explore IPT further, clinicians can refer to Interpersonal Psychotherapy – a Clinician’s Guide.6 MT
COMPETING INTERESTS: None.