An updated guide to contraception. Part 1: Short-acting methods

Women's health
This first article in an updated three-part series on contraception provides a practical guide to the short-acting methods – combined hormonal contraceptives (combined oral contraceptives and the vaginal ring) and the progestogen-only pill. Subsequent articles will provide updates on othe contraceptive methods.
- Combined hormonal contraceptives (CHCs), which contain an oestrogen and a progestogen, are available as combined oral contraceptives (COCs) and the vaginal ring.
- The advantages of CHCs include beneficial effects on acne, a decrease in menstrual pain and bleeding and the ability to manipulate menstrual cycles.
- CHC use is associated with some serious risks, but the absolute risk is low for most women of reproductive age.
- No increased risk of venous thromboembolism or arterial vascular disease has been associated with use of the progestogen-only pill (POP), although evidence is limited.
- The option of using long-acting reversible contraceptives (intrauterine devices and subdermal implants), which require minimal ongoing user actions, should be discussed with women renewing CHC and POP prescriptions.
Contraception allows women, and couples, to determine if and when to have children. This updated series of three articles provides the latest evidence-based information on the different methods of contraception available in Australia. In this article, the short-acting methods – combined hormonal contraceptives (CHCs), which are available as combined oral contraceptives (COCs) and the vaginal ring, and progestogen-only pills (POPs) – are covered. The second article will discuss long-acting reversible contraceptives (the subdermal implant, intrauterine methods and the depot medroxyprogesterone acetate injection), and the last article will cover emergency contraception and barrier, permanent and fertility awareness methods.
Most contraceptive methods are dependent on women rather than men taking the active role. With few male contraceptive methods available, further research and advocacy are required in this area. Although gendered language has been used throughout this series of articles, clinicians also need to be aware that transgender men may be at risk of unintended pregnancy.
Choosing a contraceptive method
The role of the clinician is to ensure that patients are aware of all suitable methods of contraception to allow well-informed choices. Women presenting for a repeat COC prescription may be unaware of other options available to them. There are many useful resources, including fact sheets from family planning organisation websites, to help inform women of their options.
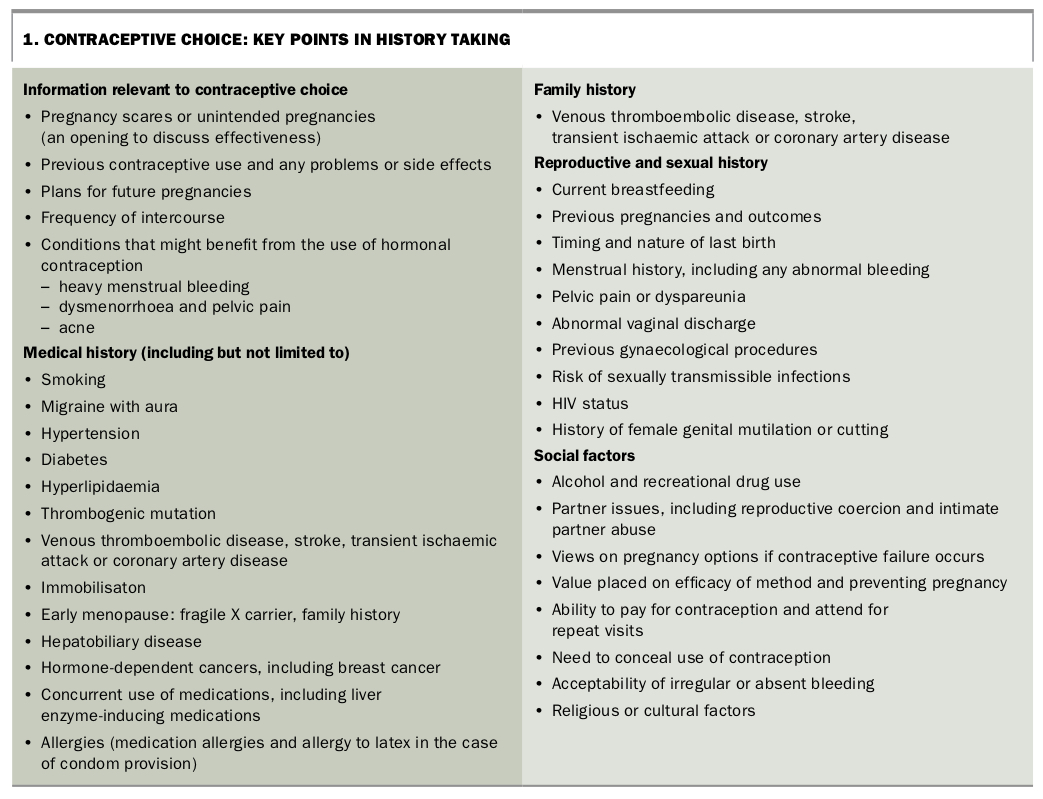
Contraceptive choice is determined by many factors, including cost, access, the presence of medical conditions, concurrent medications, relationship status and personal preferences and beliefs. Taking a thorough medical and social history is essential, with key points highlighted in Box 1.
{kind=link}
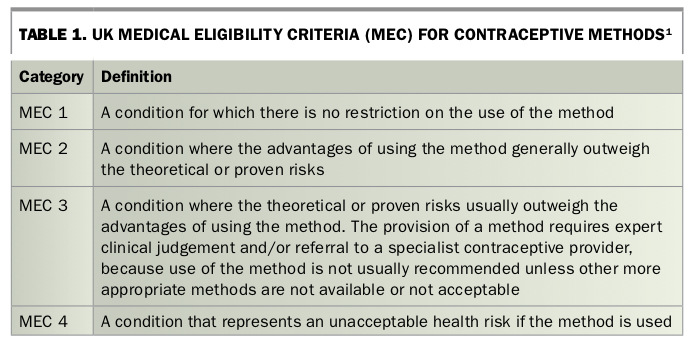
The UK Medical Eligibility Criteria (MEC) system supports the safe provision of contraception and is a useful framework within which to consider contraindications to contraceptive pills and the vaginal ring (Table 1).1 Conditions affecting eligibility for the use of each method are classified in one of four categories. A MEC 1 condition is one for which no restrictions exist, whereas a MEC 4 condition represents an absolute contraindication.
{kind=link}
As well as taking a relevant history, the clinician’s role is to provide evidence-based information about the different contraceptive methods. This may include challenging frequently held misunderstandings and myths about side effects or risks. Information provided will include the following:
- how effective the method is when used ‘perfectly’ and ‘in real life’
- how the method works
- the risks and side effects of the method
- costs of the method and associated consultations
- how to start the method and how long it will take to work
- how easily or quickly the method’s effect is reversed
- the effect on vaginal bleeding patterns, where relevant
- what to do if ‘things don’t go according to plan’, such as missed pills or late insertion of a vaginal ring
- advice on the additional use of condoms if there is a risk of sexually transmissible infections
- the availability of emergency contraception.
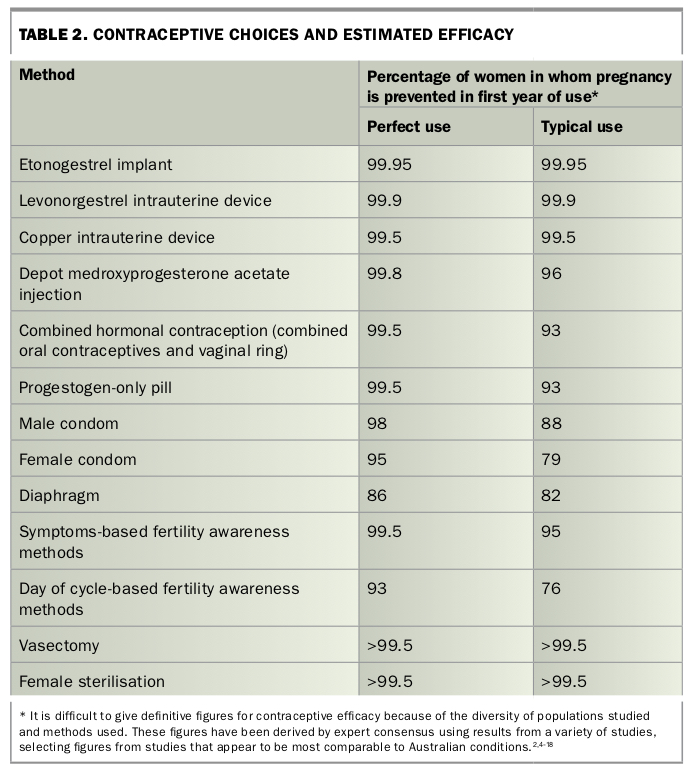
Contraceptive effectiveness is presented as the number of women in whom pregnancy is prevented among 100 women who use the method over a one-year period. Methods such as the levonorgestrel intrauterine device (IUD), the COC and the vaginal ring have similar efficacy in ‘perfect use’ (no mistakes), but the levonorgestrel IUD is much more effective in ‘typical use’ (real-life settings) because it requires minimal user action to ensure efficacy is maintained.2 As the effectiveness of long-acting reversible contraceptives is almost identical in perfect use and typical use (Table 2), it is important to include information about the benefits of such methods in all contraceptive consultations.
{kind=link}
This article discusses important information to consider when initiating COCs, the vaginal ring or POPs, as well as some of the common clinical issues that arise during their use, such as a missed pill or late ring insertion.
Combined hormonal contraceptives
Hormonal contraceptives containing an oestrogen and a progestogen (a hormone with progesterone-like activity) are available as COCs (‘the pill’) and the vaginal ring (Figure 1 and Figure 2). COCs are the most commonly used contraceptive method in Australia.3
{kind=link}
{kind=link}
The contraceptive vaginal ring provides slow release of ethinylestradiol (EE) and etonogestrel into the circulation from a soft ring made of ethylene vinyl acetate. The ring is inserted into the vagina by the woman, left there for three weeks, then removed. A new ring is inserted after a ring-free break of seven days, during which a withdrawal bleed usually occurs.
Combined hormonal transdermal patches (used weekly for three weeks, with a patch-free week) and monthly combined hormonal injections are available in some other countries.
Mechanism of action and efficacy
CHCs all work to suppress ovulation and have an efficacy rate of about 99.5% when used perfectly, but only 93% during the first year of typical use, largely because of user error (Table 2).2,4-18 This includes deviations from the pill or ring schedule, such as missed pills or late ring insertion, and running out of supplies. Prescribing the maximum allowed quantity of pills and rings is important to maximise continuation rates.19
Starting combined hormonal methods
CHCs can be prescribed if there are no medical contraindications.20 Packaging of COCs in Australia varies. Most newer pill packaging directs women to start with an ‘active hormone pill’, whereas traditional packaging directs women to start with either an inactive or an active pill depending on the timing of their menses.
CHCs can be used continuously for extended periods to minimise bleeding by either running pill packets or vaginal rings together without a hormone-free break or by using a dedicated product (see ‘Extended regimens and packs with fewer inactive pills’). A hormone-free break of four to seven days can be initiated if unscheduled bleeding occurs.
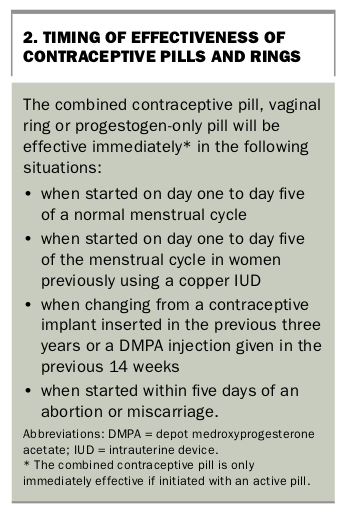
The COC (if starting with an active pill) and the vaginal ring are effective immediately when initiated on day one to day five of the menstrual cycle, as well as in certain other situations listed in Box 2.20
{kind=link}
Initiation of CHCs at other times using the ‘quick start’ method (starting a method outside the recommended time, such as on the day of the consultation) requires seven days of active hormones to be administered before contraceptive protection is achieved.21 This is sometimes known as the ‘seven-day rule’ and is based on the understanding that seven days of hormone administration are required to suppress ovulation. If pregnancy cannot be excluded at the time of initiation, the woman should be advised to have a urine pregnancy test in four weeks, even if she has a scheduled withdrawal bleed.22
Women using a pill pack that directs starting with an inactive pill rather than an active pill may need to wait up to 12 days for their COC to become effective as a contraceptive method (i.e. up to five days of taking inactive pills plus seven days of active hormone pills).
Examination and investigations
In women who are medically well and using CHCs, blood pressure and body mass index should be documented at initiation and then annually. No routine investigations are necessary.22 A review at three to four months after initiation can be helpful to check for side effects or other method-related problems.
Benefits
CHCs offer several advantages, including a beneficial effect on acne, a decrease in menstrual pain and bleeding and an ability to manipulate menstrual cycles.23 They also lower the risk of ovarian, endometrial and bowel cancer.24
Side effects
Many side effects are attributed to COCs, but evidence is limited. Weight gain is a frequent concern, but it has not been demonstrated in studies of low-dose pills containing 35 mcg or less of EE.25 Change in mood is another common concern. Although a Danish national database study found an association between first prescription of an antidepressant medication and the COC, particularly in adolescents, other studies have not found an association between COCs and depression.26,27
The following side effects have been reported by users of CHCs:
- headache
- nausea
- breast tenderness
- unscheduled bleeding
- amenorrhoea
- acne (usually improves)
- bloating
- mood changes
- reduced libido
- weight gain (no evidence it is directly related)
- melasma (also known as chloasma).
Additional device-related side effects reported by users of the vaginal ring are:
- increased vaginal discharge
- device discomfort for the user or sexual partner
- expulsion of the ring.16
As general side effects from CHCs often settle with time, women can be encouraged to persist for two to three months after starting use of a formulation.
Serious risks
Although there are some serious risks associated with CHC use, the absolute risk for most women of reproductive age is low.
Venous thromboembolism
All CHCs increase the risk of venous thromboembolism (VTE), but the absolute risk is very low, with the highest risk occurring in the first year of use.28,29 Pills containing 20 mcg of EE and 100 mcg of levonorgestrel appear to be associated with a lower risk of VTE than levonorgestrel pills with 30 mcg or more of EE.30
CHC formulations containing 30 to 35 mcg of EE plus desogestrel, gestodene, cyproterone acetate or drospirenone appear to increase the risk of VTE compared with pills containing levonorgestrel or norethisterone by a factor of about 1.5 to 1.8.31 There may also be a small increase in the risk of VTE in women using the vaginal ring compared with those using levonorgestrel- containing pills.31
The newer pills with estradiol or estradiol valerate in place of EE appear to have less impact on clotting factors.32 The risk of VTE in women using these newer combined contraceptive pills compared with those using EE-containing formulations is the subject of a multinational study that is underway.
Ischaemic stroke and myocardial infarction
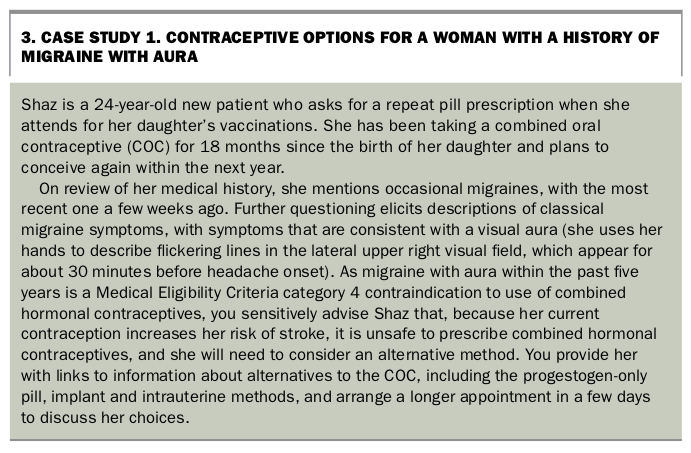
There are conflicting results as to whether use of low-dose CHCs (35 mcg or less of EE) increases the risk of myocardial infarction and stroke.33 Any risk appears to rise with increasing doses of EE.30 The absolute risk of these conditions is extremely low. Smoking, increasing age, hypertension, diabetes and hyperlipidaemia are important risk factors for both conditions, and migraine with aura increases the risk of ischaemic stroke.34,35 For women aged 35 years or older, CHCs are classified as MEC 4 for those who smoke 15 or more cigarettes a day and MEC 3 for those who smoke fewer than 15 cigarettes a day.1
Cancer
There is a small increase in the risk of cervical cancer associated with the use of CHCs,24 although in the Australian setting, which offers human papillomavirus vaccination and routine cervical screening, other risk factors such as smoking are likely to be more significant. There also appears to be a small increase in the risk of breast cancer for current users.24,36
Other risks
Use of CHCs is associated with a small increase in blood pressure; the exceptions to this are drospirenone pills, which are associated with a small decrease, and estradiol or estradiol valerate pills, which are associated with no change in blood pressure.37-39 The risk of hypertension increases in women using COCs, but the number of cases attributable to CHCs is small.40
There is a small increase in the risk of inflammatory bowel disease with use of COCs.41 Evidence is insufficient to determine whether there is an increase in gall bladder disease, but there are some restrictions on use of CHCs in women with the condition.42
Contraindications
It is important to take a medical and family history that will identify women who have contraindications to oestrogen-containing contraceptive methods. The contraindications for the vaginal ring are the same as those for the COC.
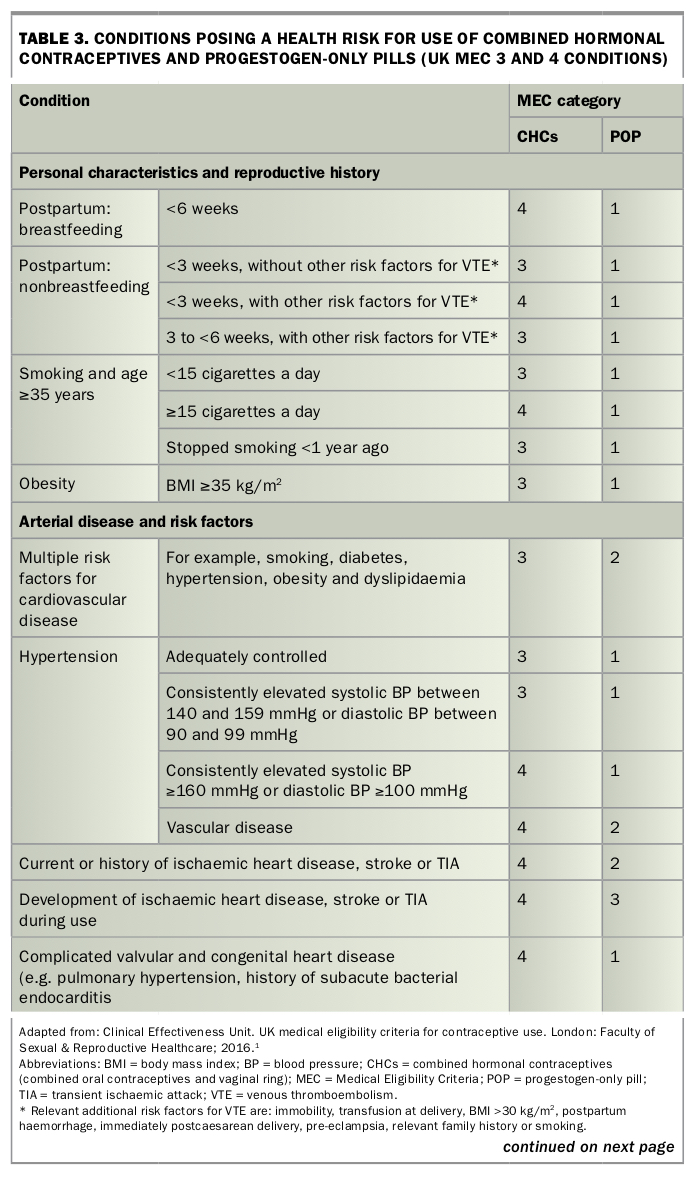
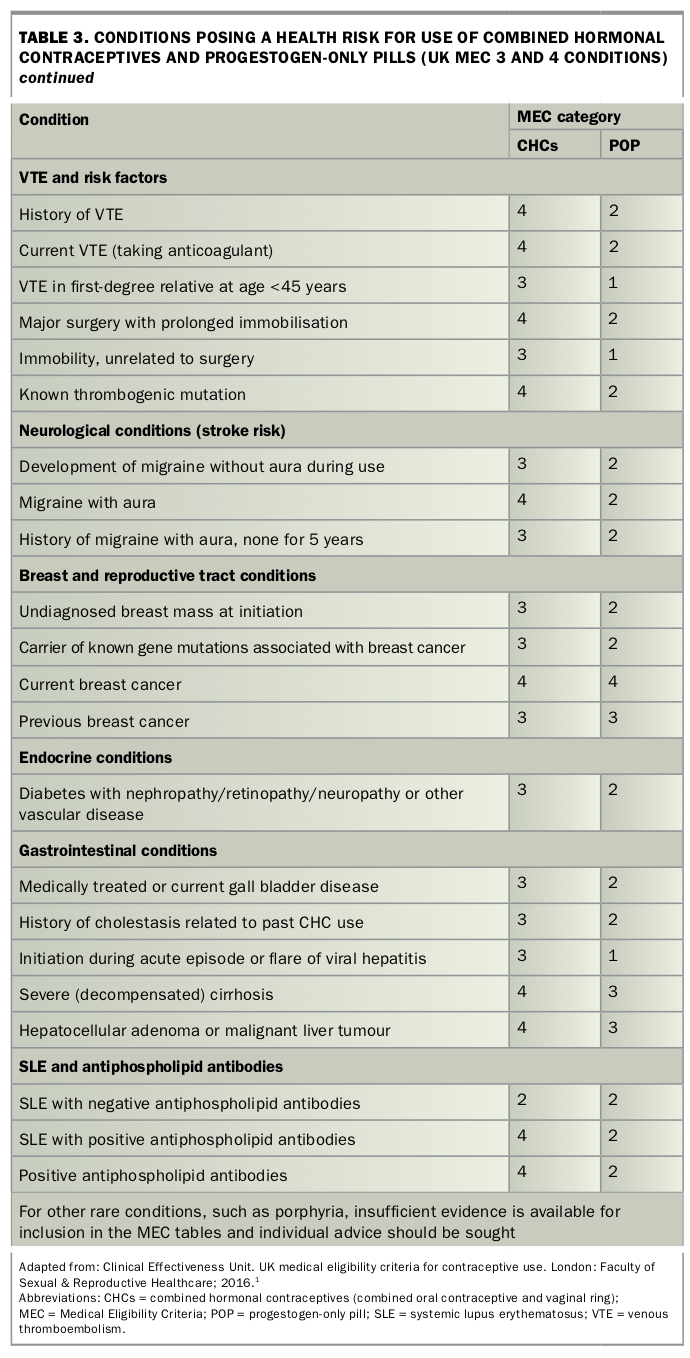
Contraindications are mostly related to risk factors for arterial and venous disease. MEC 3 and 4 contraindications include a history of migraine with aura (see Case Study 1 in Box 3), smoking over the age of 35 years or a personal history of breast cancer. Table 3 and Table 3 Pt 2 summarises the important MEC 3 and 4 conditions.
{kind=link}
{kind=link}
{kind=link}
Other important considerations for the use of CHCs include difficulties in taking pills on a regular basis (e.g. shift workers) or inserting a ring at the correct time, as well as being able to access an ongoing contraceptive prescription and supply.
Choosing a combined hormonal contraceptive
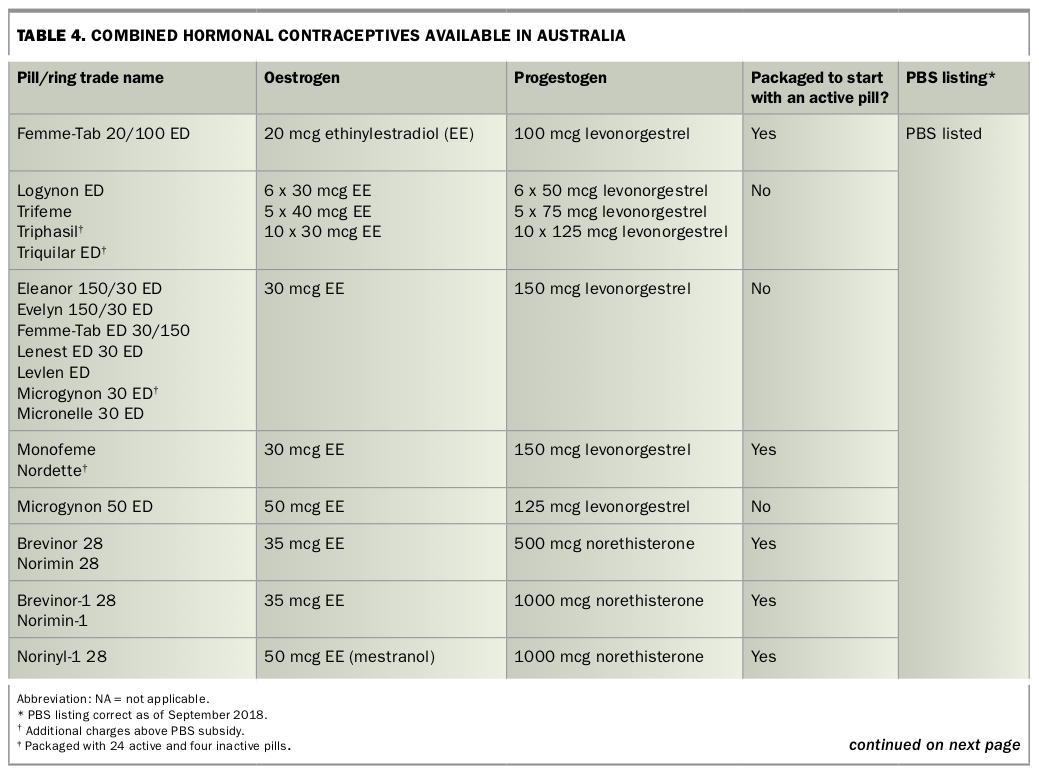
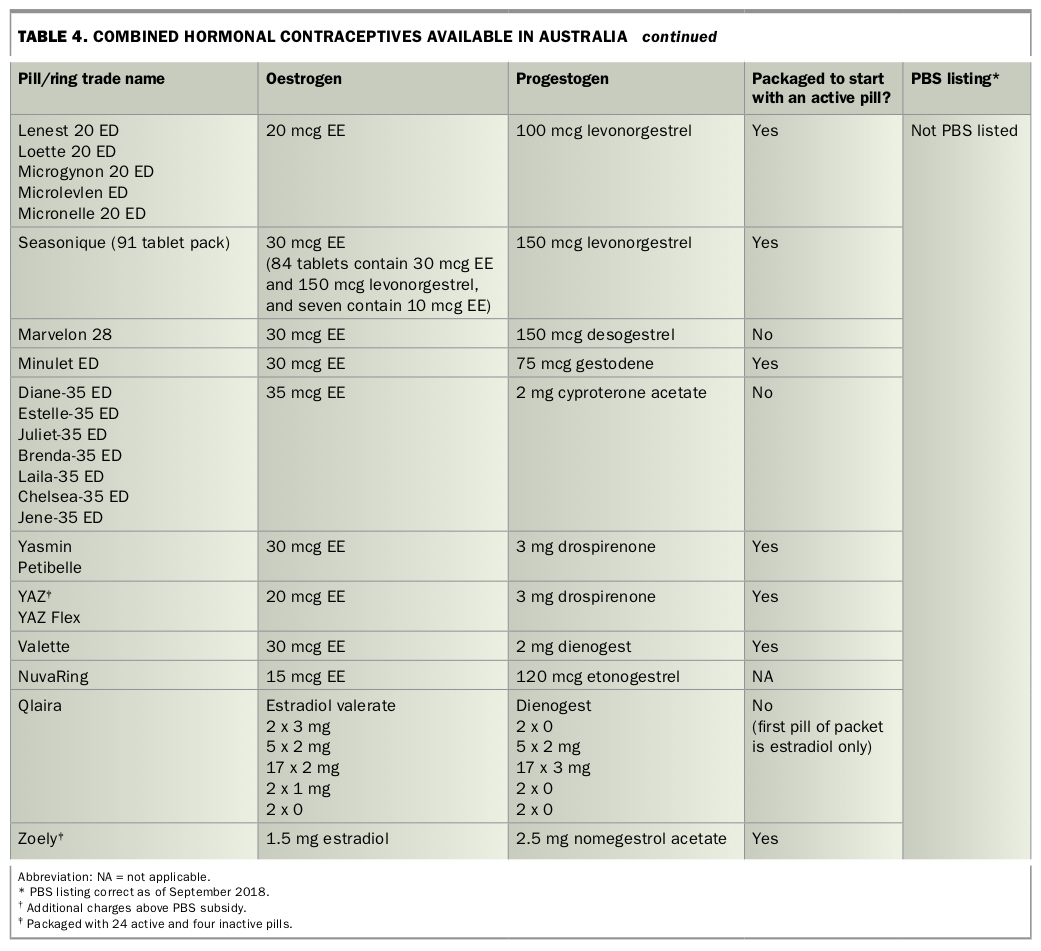
There is a large and sometimes confusing choice of combined contraceptive pills. Those available in Australia are listed in Table 4 and Table 4 Pt 2.
{kind=link}
{kind=link}
It is important to be aware that although some pills have other brand-specific indications in addition to contraception, this is almost always based on comparison with placebo rather than with other pills. For example, some COCs have an indication for treating acne, yet a Cochrane review concluded that ‘Few important and consistent differences were found between COC types in their effectiveness for treating acne’.43
Low-dose pill
A low-dose pill containing 20 or 30 mcg of EE and levonorgestrel is the recommended first choice.22 These pills have been extensively studied and have had similar discontinuation rates as other CHCs when compared in head-to-head trials.44,45 Some brands of these pills are subsidised under the PBS and are inexpensive (Table 4 and Table 4 Pt 2). Pills containing 20 mcg of EE are associated with a higher rate of unscheduled bleeding than pills containing 30 or 35 mcg of EE, which can lead to early discontinuation.46 However, there appears to be a small safety benefit in terms of risk of VTE and arterial vascular disease with pills containing 20 mcg of EE.30
Alternative first choices are as follows.
The vaginal ring
The vaginal ring offers an alternative delivery system to the COC that may be preferred by some women. Compared with the combined contraceptive pill, the lack of need for daily activity may improve compliance; it also offers an advantage when malabsorption might be an issue and it may be associated with less unscheduled bleeding.45,47-49 The ring is not subsidised by the PBS.
Alternative progestogens
Over the past few decades, progestogens (including dienogest, drospirenone, desogestrel and gestodene) have been developed with the aim of reducing metabolic impact and enhancing beneficial effects on acne and hirsutism.50 Some have been designed with additional potential benefits; for example, drospirenone is a spironolactone analogue and has a mild diuretic effect.51 There is insufficient clinical evidence to preferentially prescribe these newer progestogens. However, although evidence is lacking, logically the pills containing an antiandrogenic progestogen (i.e. dienogest, drospirenone and cyproterone acetate) can be considered for women with acne and hirsutism, particularly if there has been a limited response to a pill containing levonorgestrel or norethisterone. Pills containing cyproterone acetate are licensed for the management of severe acne and hirsutism and can be used to deliver contraception in women taking them for these indications.
Extended regimens and packs with fewer inactive pills
Two approaches – extended-regimen formulations where consecutive active pills are taken beyond the traditional 21 consecutive days, and packs with fewer inactive pills – may provide a greater margin for error if pills are missed.52-55 These regimens may also minimise oestrogen withdrawal symptoms, including headache and pelvic pain, that can occur in the hormone-free break.56
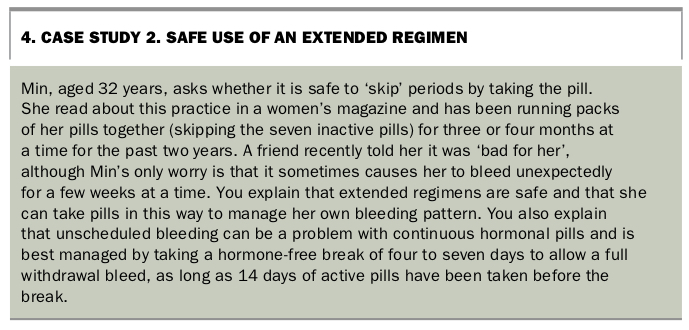
- Extended regimens. COCs and vaginal rings can be used continuously without a hormone-free break. This regimen may, be chosen for convenience or to avoid symptoms associated with hormone withdrawal; it can be used with any monophasic pill, or a new vaginal ring can be inserted every four weeks without a ring-free break. There is no upper limit to the number of hormone-free breaks that can be skipped.22 Although many women achieve amenorrhoea with continuous use of CHCs, unscheduled bleeding can be problematic.57 If troublesome breakthrough bleeding occurs for four or more days, the woman can be advised to stop use of the COC or vaginal ring for four to seven days, as long as active hormones have been administered for 14 days before the break (see Case Study 2 in Box 4).58 Persistent unexplained bleeding requires consideration of other causes, such as a sexually transmissible infection or polyp. Two dedicated extended-regimen formulations are available in Australia. A pill containing 30 mcg of EE and 150 mcg of levonorgestrel that is taken for 84 consecutive days, followed by seven days of 10 mcg of EE, became available in Australia in 2016. This formulation is designed for women to have four withdrawal bleeds per year. In theory, oestrogen withdrawal symptoms should be minimised because of the absence of hormone-free breaks, but no supportive evidence is available. A flexible regimen using an electronic dosing device is also available. This device, which has proven acceptable to women, allows a four-day break at any time if at least 24 consecutive pills have been taken previously.59
- Pill packs with fewer inactive pills. The estradiol-nomegestrol pill and the 20 mcg EE-drospirenone pill are packaged with only four inactive pills per cycle. The estradiol valerate pill is packaged with only two inactive pills and four pills containing estradiol valerate and has been shown to be effective at reducing the headache and pelvic pain that can occur with traditionally packaged pills during the seven-day hormone-free break.44
{kind=link}
Pills with estradiol and estradiol valerate
Since 2010, pills containing estradiol or its prodrug estradiol valerate have become available. Unlike EE, these oestrogens are identical to the oestrogen produced by the ovary. They have been shown to have less impact on clotting factors and so have a theoretical but unproven benefit in terms of VTE risk.32
Special situations
Drug interactions
With the exception of rifampicin and rifabutin, antibiotics do not decrease the efficacy of CHCs, and additional precautions are not needed during concurrent use.
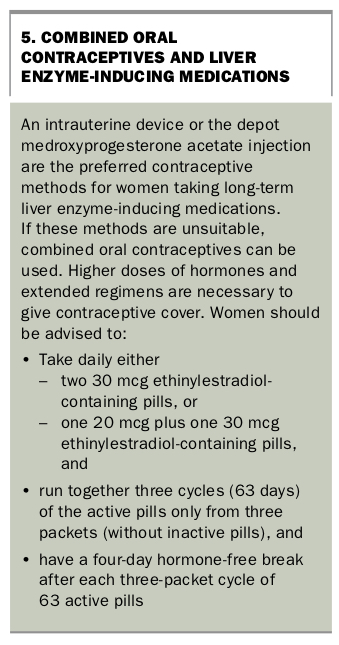
Liver enzyme-inducing medications, which include several antiepileptics, antiretrovirals and the herbal remedy St John’s wort, reduce the effectiveness of COCs and the vaginal ring (as well as the POP and implant). It is recommended that women taking these medications use either an intrauterine contraceptive method or depot medroxyprogesterone acetate. Women who choose a COC will require a higher dose and an extended regimen (Box 5).60 The vaginal ring is not recommended owing to its inflexible dosing regimen.
{kind=link}
Missed pills and incorrect ring use
Advice for when a pill is missed is summarised in Flowchart 1. The advice is based on international guidance and may differ from package information. It is important to remember that a COC is not missed until it is more than 24 hours late (i.e. it is 48 hours since the last pill was taken). The most ‘risky’ pills to miss are the first seven after the hormone-free break, when the chance of breakthrough ovulation is highest.
The same advice can be used in the case of a vaginal ring that has been inserted more than 24 hours late or has fallen out or been taken out during use and has not been reinserted within 24 hours. It is important to discuss the dual use of condoms and access to emergency contraception with all pill and ring users.
Stopping at menopause
CHCs are generally not recommended for women aged 50 years or older. Unlike progestogen-only methods, follicle-stimulating hormone (FSH) level cannot be used as an indicator of ovarian failure in women using CHCs.61
Alternatives include:
- switching to a progestogen-only pill (see below), an implant or an IUD, then following the recommendations for stopping at menopause (covered in other articles in this series)
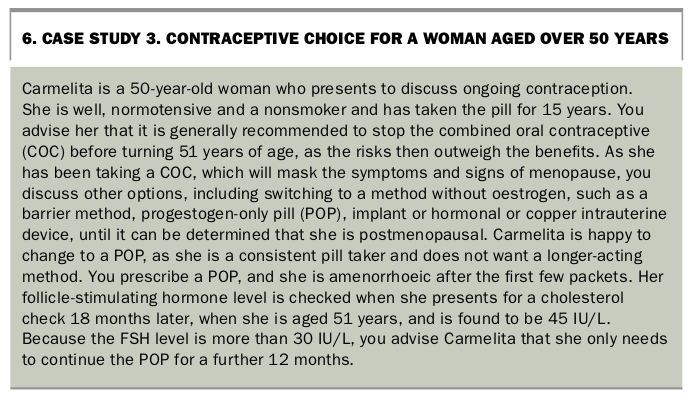
- changing to a barrier method. If the woman is amenorrhoeic for a year (or two years if she is aged under 50 years), she no longer needs contraception (see Case Study 3 in Box 6). If regular periods occur after ceasing the CHC, resumption of contraception should be considered.
{kind=link}
Progestogen-only pill
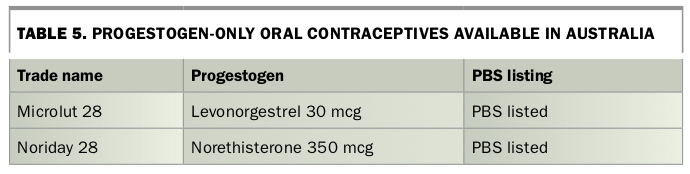
Two POPs are available in Australia: one containing 30 mcg levonorgestrel and the other containing 350 mcg norethisterone (Table 5). The POP is often used for women who are intolerant of or have a contraindication to oestrogen but prefer an oral contraceptive method.
{kind=link}
Mechanism of action and efficacy
POPs containing levonorgestrel or norethisterone primarily act by thickening cervical mucus and affecting the luteal phase of the menstrual cycle.62 The effect varies between women and between cycles.63
There is limited evidence on the efficacy of POPs, but it is considered the same as that of CHCs: 99.5% in perfect use and 93% in typical use (Table 2).2 However, the POP is also considered to have a more vulnerable efficacy, and strict adherence to taking it within a daily three-hour timeframe is important for maximum efficacy. Failure rates are lower in women aged over 40 years than in younger women.64
Starting the progestogen-only pill
POPs can be started in women of any age and can be used until menopause is established if there are no contraindications. All POP packs have 28 active pills and no inactive pills. POPs are immediately effective in the same situations as CHCs (Box 2) and when initiated immediately after giving birth. In most other situations, they are effective after three tablets have been taken, as the cervical mucus is thickened by 48 hours.
Examination and investigations
Although it is good medical practice to check blood pressure, no examination or investigation is necessary before initiating the POP in a woman who is medically well.
Side effects and serious risks
No increased risk of VTE or arterial vascular disease has been associated with use of POPs, although evidence is limited.29,65 Recent evidence has indicated there may be a small increased risk of breast cancer in users of the levonorgestrel POP; however, the number of breast cancers was small and further studies are needed.36 The most common side effect is irregular bleeding, with about 20% of women taking POPs experiencing amenorrhoea, 40% having irregular bleeding and 40% having regular cycles.66-68 Although a Danish national database study found an association between first prescription of an antidepressant medication and POP use, the number of women using POPs and antidepressants was low.27 Use of the POP in women with depression is classified as MEC 1.1
Contraindications
The POP is generally considered safe, and the only MEC 4 contraindication to its use is current breast cancer.1 The important MEC conditions are summarised in Table 3 and Table 3 Pt 2.
Choice of POP
When choosing a POP, there is no evidence that one type is more beneficial than the other. Either a levonorgestrel or a norethisterone POP can be initiated as first choice.
Special situations
Drug interactions
POPs are not recommended for women taking liver enzyme-inducing drugs.
Missed pills
A POP is considered missed when it is three or more hours late. Condoms should be used until three consecutive daily pills have been taken (i.e. it is 48 hours since the first POP after the missed one was taken), and the woman should consider emergency contraception options if she has unprotected sex during this time (see Flowchart 2). Unlike for the COC, emergency contraception is not required for any sexual intercourse occurring in the five days before the missed pill, as the cervical mucus effect remains until a pill is missed.
Bleeding irregularities
For women who experience bleeding irregularities while taking a POP, a change of formulation or a double dose may be considered. There is no evidence to support either option and, although the latter is ‘off label’, it is unlikely to cause harm. There is no indication to use a double dose in women with a high body mass index.
Stopping at menopause
The FSH level should be measured once a woman taking a POP has a year of amenorrhoea after turning 50 years of age. If the FSH level is greater than 30 IU/L, the POP can be stopped after a further 12 months. Alternatively, POP use can be continued until the woman is 55 years old. Conception in women aged 55 years or older is extremely unlikely.61
Conclusion
The COC remains the most commonly used method of contraception in Australia. The COC and vaginal ring offer several benefits, including a beneficial effect on acne and the ability to manipulate menstrual cycles. Although most women can safely use CHCs, history taking with reference to the MEC framework is extremely important, so that those at higher risk of VTE, stroke and ischaemic heart disease can be offered alternative methods. The POP is a very low-dose option and is safe to use in most situations. Strict timing of POP intake is important to maintain contraceptive efficacy.
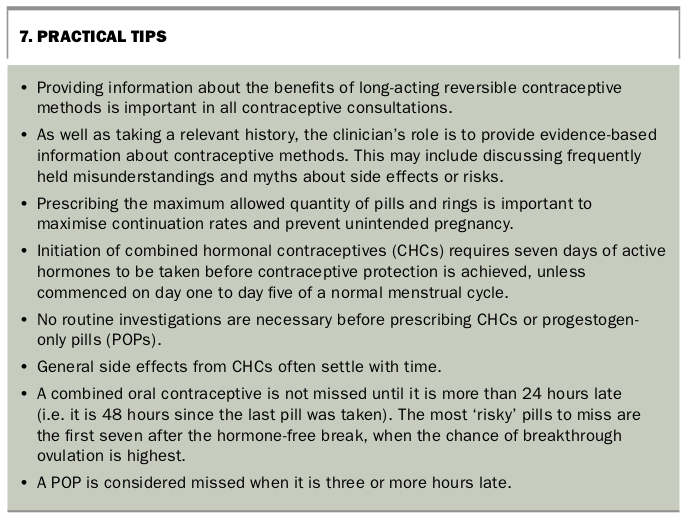
Practical tips for GPs are given in Box 7. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.