Managing anxiety disorders in adults

Mental health
The GP has a key role in identifying patients presenting with anxiety symptoms and ensuring appropriate acute and long-term management. There are two key messages for GPs to follow: once you have made a diagnosis of an anxiety disorder, tell the patient you have a treatment for it. Second, do not let your anxiety lead you to prescribe inappropriately or overinvestigate for all possible differential diagnoses.
- Management of anxiety disorder requires a biopsychosocial and lifestyle approach.
- Anxiety disorders are common and often disabling but are under-recognised and often poorly treated in clinical practice.
- Effective first-line treatments are cognitive behavioural therapy (CBT), either face-to-face or digitally delivered (dCBT), and the serotonergic antidepressants.
- No matter what treatment is selected, it is likely to take four to six weeks to begin to show an effect.
- Functional recovery is the goal and is achievable through effective use of evidence-based treatments.
- Use of evidence-based clinical practice guidelines for treatment has been shown to result in better outcomes.
Anxiety disorders, like all mental disorders, lie on a spectrum that extends from normal anxiety to transient symptoms, through to severe and disabling symptoms that can persist for years. The specific thoughts and behaviours that characterise each of the anxiety disorders are covered in the RANZCP Clinical Practice Guidelines for anxiety disorder.1 These disorders include variants of excessive worry, acute attacks of anxiety or panic and avoidance of anxiety-provoking situations.
Panic disorder, social anxiety disorder (SAD) and generalised anxiety disorder (GAD) are the most common anxiety disorders in Australia and New Zealand. Obsessive compulsive disorder (OCD) and post-traumatic stress disorder (PTSD) have been moved out of the DSM-5 chapter on anxiety disorders and placed in their own categories of ‘Obsessive compulsive and related disorders’, and ‘Trauma and stressor-related disorders’, respectively.
The systematic implementation of anxiety disorder guidelines has been shown to result in earlier treatment gains and shorter treatment times.2 This article draws from the RANZCP guidelines to focus on the use of psychological treatments and pharmacotherapy to treat panic disorder, SAD and GAD, for which there is considerable evidence of efficacy. The key features of these anxiety disorders are presented in Table 1. This article also provides practical clinical guidance on cognitive behavioural therapy (CBT) as the principal psychological treatment for the anxiety disorders as it has the most extensive evidence base for its efficacy. Furthermore, it is available online, allowing easy and extensive dissemination. The selective serotonin reuptake inhibitor (SSRI) and serotonin and noradrenaline reuptake inhibitor (SNRI) antidepressants are also covered because the evidence base of benefit is larger, the side effect profile is better, and the experience of practitioners is wider than with other classes of medication, especially the older, or first generation, antidepressants.
Factors contributing to the onset of anxiety disorders
Anxiety disorders arise from a combination of vulnerable personality traits, early life stressors and psychosocial adversity (for example, lack of support, hardship, dysfunctional relationships) and are often triggered by stressful significant life events (such as the death of a loved one, an illness, childbirth or workplace bullying). Temperamental traits, with a moderate level of heritability (such as neuroticism or negative emotionality), are important vulnerability factors for anxiety; neuroticism, in particular, seems to confer greater vulnerability to how an individual responds to psychological distress, which may precipitate an anxiety disorder in the context of environmental or interpersonal stressors.
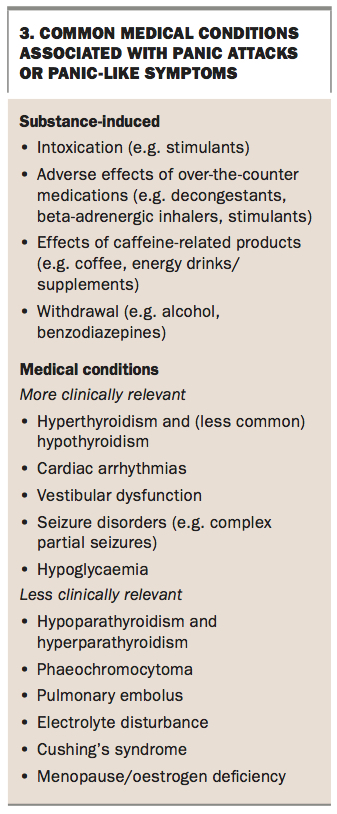
Substance use and misuse (including over-the-counter medications, herbal medications and intoxication) or withdrawal are often missed as a cause of anxiety, hence it is important to screen for these.
Prevalence, cost and functional impact
Anxiety disorders, as conceptualised in previous classification systems such as DSM-IV (that included OCD and PTSD as anxiety disorders), form the most common class of mental disorders.3-6 The second Australian Survey of Mental Health and Wellbeing, based on the DSM-IV, estimated that one in seven adults (14.4% of the population) experienced an anxiety disorder in the past 12 months. A very similar rate (14.8%) was estimated in New Zealand.7,8 SAD is the most prevalent anxiety disorder, followed by GAD and panic disorder/agoraphobia (Table 2).8,9 Anxiety disorders are more common in women than men; in people who are separated, divorced or widowed; and those who are less educated or unemployed. Demographic status may be both a consequence and a cause of anxiety disorders.10
Anxiety disorders are associated with high levels of distress, disability and service use.10 In the second Australian Survey of Mental Health and Wellbeing, in people who met criteria for an anxiety disorder, about half reported an inability to work or do normal tasks for less than one day during the previous month because of anxiety, a third reported one to seven days and one-sixth reported more than seven days.
Onset and course
Anxiety disorders typically start early in life (Table 3), and prevalence declines with age.7,11 Developing an anxiety disorder after the age of 40 years is uncommon, and so when a person over 40 presents with an initial onset of an anxiety disorder, alternative causes of anxiety such as mood disorders, alcohol and substance use disorders, trauma, physical illness or its treatment should be considered.9,10
Panic disorder often follows a waxing and waning course with periods of increased anxiety (characterised by worsening or episodic flares of symptoms) and periods of remission in between. Some experience a fluctuating course with exacerbations that are often precipitated by life-event stress, excess caffeine, sleep disruption, physical illness or hormonal changes, whereas others have a more chronic course. Only a minority have complete, sustained remission without relapse.12-14
SAD is usually a chronic disorder. Periods of remission are most common in milder, nongeneralised SAD, in nonclinical patients, and in those with fewer social fears.15-17 The US National Comorbidity Survey Replication estimates that only 20 to 40% of people with SAD recover within 20 years of onset and only 40 to 60% recover within 40 years.16
GAD is a chronic disorder that can be exacerbated by stressful life events. Most patients are still affected after 10 years, and half of those who remit will relapse (Table 4).18,19
Service use
It is estimated that less than half of people with anxiety disorders seek treatment from a health professional. Those who do seek treatment commonly attend primary care, where anxiety is largely under-recognised.20 Only 30 to 60% of people who see their GP for an anxiety disorder receive a treatment regarded as adequate9,21 and Australian data suggest that overall, only a third of treatment-seekers receive minimally adequate treatment, with the rest receiving counselling or inadequate advice.22,23
People with panic disorder seek help more frequently, often from medical specialists or emergency departments, probably because of concerns about their physical symptoms.24-27 They are sometimes referred for unnecessary investigations to rule out possible medical causes for the symptoms.
Comorbidity
There are high rates of comorbidity between anxiety disorders and depressive disorders. Most patients seen in a clinical psychiatric practice will meet criteria for more than one mental disorder, and this comorbidity is associated with most disability days and consultations due to mental disorders.28-30 Comorbidity should be routinely assessed, as it is an indicator of increased functional impairment and economic costs.29,31-33
Comorbidity has been associated with a slower rate of recovery and a poorer response during active treatment. However, the presence of comorbidity should not lead to undue pessimism about the value of treatment and prospects for eventual recovery, since both antidepressant medication and CBT may still be effective.34,35
Overall, medical comorbidity across anxiety disorders is not associated with poorer outcomes;36 and several studies have shown that people with or without comorbid disorders respond similarly to face-to-face CBT and digitally-delivered CBT (dCBT).37-39
Suicide risk
People with anxiety disorders have an increased risk of suicidal ideation and attempts, especially when comorbid with depression. All patients with anxiety disorders should be assessed for suicidal thinking, risk of self-harm and the presence of comorbid depression.
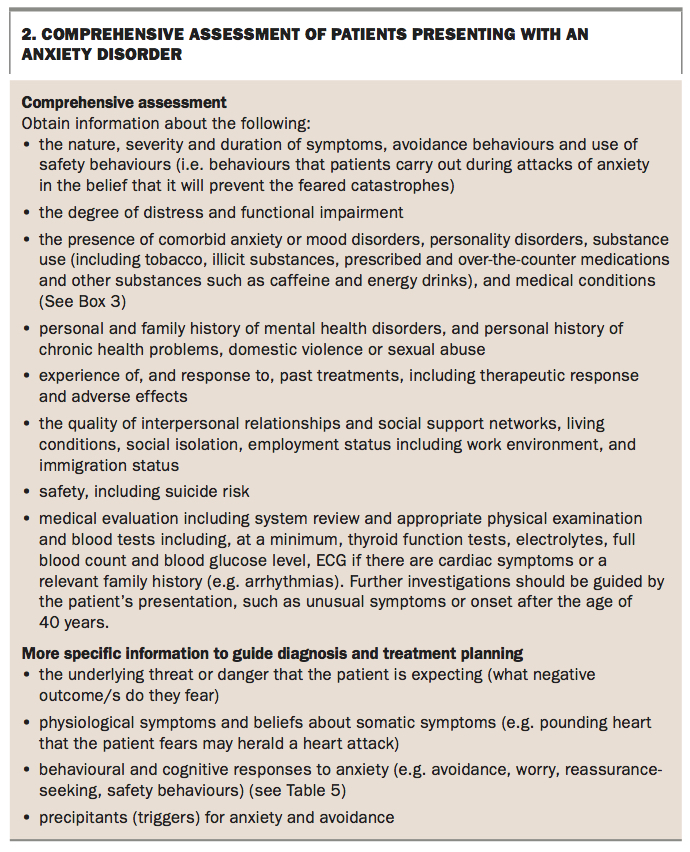
Assessing patients presenting with an anxiety disorder
When a patient presents with a suspected anxiety disorder (Box 1), a comprehensive assessment to obtain as much relevant information as possible is essential to providing an optimal treatment plan (Box 2 and Box 3). The aims of the assessment are to:
{kind=link}
{kind=link}
- establish a good therapeutic relationship with the patient
- develop a detailed biopsychosocial and lifestyle formulation
- consider differential diagnoses and establish a primary diagnosis
- identify comorbid disorders that may affect treatment and outcome and assist treatment planning
- assess psychosocial and lifestyle factors that could help or hinder the recovery process
- assess the capacity of the patient to benefit from self-help material independent of the clinician (for example, ask about digital competence, possibly indicated by social media and other online activity).
Most cases of anxiety disorder are likely to be diagnosed by a GP, but in cases of uncertainty, a second opinion from a psychiatrist or clinical psychologist may be helpful.
Differentiating anxiety disorders
One of the most important ways of differentiating between anxiety disorders is to examine the associated cognitions. People with panic disorder worry that their panic will result in physical or mental harm to themselves, people with SAD worry that they will be judged negatively, and those with GAD worry excessively across a variety of contexts (Table 1). Importantly, panic attacks can occur in any anxiety disorder (including specific phobias), whereas OCD and PTSD occur when people are confronted by their feared or triggering situation. Being anxious a lot of the time is not synonymous with GAD as there are specific concerns and features that are required for a clinical diagnosis of GAD. There is a range of self-report measures that can assist with symptom assessment and monitoring (Box 4).40-59
Treatment
These guidelines recommend a pragmatic approach to selecting therapy in collaboration with the patient, beginning with psychoeducation and advice on lifestyle factors, followed by specific treatment.
Selection of treatment should be based on:
- evidence of efficacy
- patient preference
- accessibility
- cost
- tolerability
- safety
- consideration of symptom severity and comorbidity.
If symptoms are mild, transient and without associated impairment in social and occupational function, patients may not require treatment.60 In such cases, reassurance, psychoeducation and review may be the most appropriate approach.
If symptoms are impairing the patient’s ability to function, recommended initial treatment options include:
- CBT, delivered face-to-face or digitally, using a smartphone, tablet or computer (dCBT)
- medication with an SSRI (or an SNRI if SSRIs are ineffective or not tolerated), accompanied by instructions for graded exposure to anxiety triggers
- a combination of CBT and medication.
The choice of treatment should be made in collaboration with the patient, taking into consideration patient preference and prior responses to treatment, with one proviso: that people with severe anxiety disorders or severe comorbid major depression be advised to consider a combination of antidepressant medication and CBT. When possible, the patient’s family or significant others should be involved in management planning decisions and in supporting the patient through their treatment. Despite the frequent use of CBT and pharmacotherapy for anxiety disorders in clinical practice, there is currently limited evidence to support routine use of this combination.
Cognitive behavioural therapy
At the simplest level, CBT helps patients recognise and change the dysfunctional thoughts, emotions and behaviours that are part of the fear and avoidance that typify and maintain their disorder. CBT is a skills-based approach that consists of psychoeducation about the nature and maintenance of anxiety, providing skills in identifying and challenging anxious thoughts and repeated and graded exposure to feared or avoided stimuli (situations, sensations or thoughts).
CBT can be delivered face-to-face (individual or group), digitally, or through self-guided CBT books for patients (self-help books). Face-to-face delivery of CBT, particularly individual therapy, has been the most extensively studied with its efficacy supported by meta-analyses.61 CBT has been manualised for therapists and patients, and CBT manuals can be digitised.62-64 Benefiting from CBT, whether face-to-face or online, requires the patient to practise their skills regularly.
Face-to-face CBT is effective, especially when conducted by a trained clinical psychologist, and is as or more acceptable than digital help or self-help methods. However, it is much less accessible, and there is a risk of loss of fidelity, that is, a risk that the treatment delivered may not include all the elements of the treatment package that research has shown to be effective. Digital CBT and self-help have fidelity and are more accessible and may be as effective but are not acceptable for some.
Psychotherapy is generally less associated with side effects than pharmacotherapy. Pharmacotherapy can be associated with adherence problems, but medications are usually accessible. The direct financial costs to the patient are highest with any face-to-face intervention, i.e. talking therapy or medication.
It is likely that some patients will only respond to CBT and others only to antidepressants. Therefore, persisting with either when there is no response may not be beneficial, and switching to the alternative may be more productive.65-68
Medications
The advantages of pharmacotherapy are that the recommended medications are easily prescribed in primary care, they are widely available at relatively low cost, and the quality of medicines is assured. Antidepressants, especially the SSRIs and, to a lesser extent, the SNRIs, are the first-line medications for panic disorder, SAD and GAD based on evidence from placebo-controlled randomised controlled trials, overall safety and low misuse potential.69,70 Pharmacotherapy for anxiety disorders should always be accompanied by instructions for graded exposure to feared situations.
SSRI and SNRI antidepressants
For about half of the participants in clinical trials of SSRIs or SNRIs, symptoms improve to the point that they no longer meet criteria for the disorder. Disability decreases and quality of life improves. Although the tolerability profiles of SSRIs and SNRIs in patients with anxiety disorders are not fully established, systematic reviews of studies in depressed patients suggest that duloxetine and venlafaxine may be less well tolerated than the SSRIs.71,72 Overall, the evidence does not indicate that any one of these medications be preferred over another and selection should be made based on previous success with the individual patient, patient preference, and clinician familiarity with the medication.
SSRI and SNRI antidepressants can have adverse effects including initial exacerbation of anxiety (particularly where there is a history of panic attacks), nausea, headache, sleep disruption and sexual dysfunction. It is important to be aware that people with anxiety disorders, particularly those with panic disorder, are very aware of and concerned about bodily symptoms. They should receive careful education about likely adverse effects if prescribed SSRI and SNRI antidepressants and be warned that adverse side effects usually occur early in treatment before benefits are seen, and these side effects usually settle. In younger people, there has been an association of SSRIs with suicidal thoughts, but not completed suicide.73,74 Clinicians should therefore use caution in prescribing any antidepressant in childhood or early adolescence.
Dosing of SSRIs and SNRIs
To reduce the likelihood and severity of side effects, and the risk of exacerbating anxiety, it is advisable to start treatment with antidepressants at a low dose (about half of the starting dose given to depressed patients) and to titrate slowly, increasing the dose as tolerated to therapeutic effect. Patients should be advised to take the medication daily as prescribed, not just when they feel anxious, and that it can take up to six weeks to feel a benefit from the medication, or even up to 12 weeks to experience the full benefit.
There is inconsistent evidence for a dose-response relationship; however, some patients who have not responded to a lower dose may respond to a higher dose within the therapeutic dose range. Little evidence is available to guide the duration of treatment. If the desired response is achieved, the medication should be continued for 12 months. Discontinuation should be gradual, for example, over three to four months to minimise discontinuation symptoms or withdrawal syndrome.
Other antidepressant classes
Tricyclic antidepressants (TCAs) have demonstrated efficacy in the treatment of panic disorder and GAD, but they are associated with more side effects, poorer tolerability and toxicity in overdose. TCAs should be reserved for patients who have not responded to, or are unable to tolerate, SSRIs and SNRIs. Abrupt discontinuation of TCAs may cause similar symptoms as well as lead to cholinergic rebound.75
The irreversible monoamine oxidase inhibitors (MAOIs) have proven efficacy in SAD and panic disorder. However, their use in the treatment of these disorders has been limited because of serious potential adverse effects, the need for dietary restrictions, toxicity in overdose and important pharmacokinetic interactions; referral to a psychiatrist to prescribe MAOIs is advisable.
Moclobemide, a reversible inhibitor of monoamine oxidase A (RIMA), has been shown to be modestly effective in the treatment of SAD, and there is limited evidence that it is effective in the treatment of panic disorder. Doses of RIMA up to the recommended maximum dose do not require dietary restriction. Above this dose, dietary restrictions will be necessary for foods containing tyramine.
Very few studies have evaluated mirtazapine in the treatment of anxiety disorders, but it is used by some clinicians. There is some evidence to support the use of agomelatine in GAD, but not the other anxiety disorders.76
Drug-drug interactions with antidepressants
Interactions with other drugs can occur because of pharmacokinetic or pharmacodynamic effects. Prescribers are strongly advised to check for the risk of interactions when prescribing for a patient who is taking other medications.77
Stopping and switching antidepressants
When ceasing some SSRIs and SNRIs (especially paroxetine and venlafaxine), many individuals experience a withdrawal syndrome, with flu-like symptoms, shock-like sensations, dizziness, insomnia, vivid dreams, irritability and crying spells, as well as excessive sweating and myalgia. Fluoxetine and its metabolite have a very long half-life, which means that discontinuation symptoms are unlikely, but this also means that a washout period of five weeks is required before changing to another antidepressant or other medication.
Benzodiazepines
Benzodiazepines have well established anxiolytic effects, but there is concern about their use because of adverse effects, (including cognitive impairment, falls, and sedation) tolerance and dependence.78 Their use can undermine the effectiveness of CBT by becoming a safety behaviour when patients see taking a benzodiazepine as their main source of relief. Such a belief may present a barrier to considering other means of managing their anxiety in patients with panic disorder and SAD. Because of these concerns, benzodiazepines should not be used as first-line agents, but be reserved for patients whose symptoms have not responded to other treatments. There is also potential for abuse of benzodiazepines and, although it is difficult to predict which patients will develop long-term problems, benzodiazepines should be avoided in those with a previous or current history of substance abuse.79
Benzodiazepines may have a favourable safety profile in the management of treatment-refractory anxiety disorders, compared with atypical antipsychotic agents.
Benzodiazepines are not recommended routinely when commencing patients on SSRIs – slow titration and frequent review in the early stages of treatment will enable most patients to start SSRIs without significant worsening of their anxiety.
Follow-up and monitoring
The onset of beneficial effects typically occurs 4 to 6 weeks after starting treatment with either CBT or medication. GPs should initially see the patient weekly to monitor adherence and adverse effects, to identify any exacerbation of symptoms until there is a response and symptoms have stabilised, and to listen to any concerns or anxieties the patient has regarding treatment (the latter builds and strengthens the connection with the patient that in turn will enhance the efficacy of treatment). The effectiveness of treatment should be reviewed after four to six sessions of weekly CBT or after four to six weeks of pharmacotherapy with advice on graded exposure to feared situations. Rating scales (Box 4 and Table 5) can be used to monitor change and are often helpful for both patients and GPs.
Education
All patients should be educated about anxiety, especially the adaptive aspects; an increase in alertness and anxiety facilitates problem-solving, whereas severe anxiety impairs the ability to problem-solve and can be debilitating (Yerkes-Dodson curve; Figure).80,81 This information is extremely beneficial because the patient often feels that what they have been experiencing is frightening and unique to them. Education about managing anxiety involves outlining fear-reinforcement cycles to the patient as an explanation for why anxiety has persisted and the need to eventually confront what is feared.
Educating patients also includes the promotion of healthy lifestyle behaviours including healthy eating, good sleep, regular exercise and reduced use of caffeine, tobacco and alcohol. Reliable, plain-language information for patients is available online (www.yourhealthinmind.org).
What can GPs do to help someone who is acutely anxious?
In patients experiencing acute anxiety, just sitting in the waiting room often helps to reduce symptoms because they know that a doctor is near. However, if they are hyperventilating severely and do not respond to reassurance, they can be guided through a slow-breathing technique, in which they are instructed to take light (not deep) breaths in and out over cycles of about six-seconds. It is likely to take at least five minutes of this to have an effect, and if the patient becomes distressed again during the consultation it can be repeated. The management of significant distress from acute anxiety, as marked by extreme and severe symptoms, is outlined in Box 5.
Patients suffering from chronic anxiety require a more comprehensive management approach. It is important to remember that anxiety often fluctuates, and GPs will almost certainly be seeing the patient at their worst. Resist the urge to write a prescription immediately, as many people are instantly reassured just by knowing from the GP that they have a recognisable and treatable condition.
There are also a number of online resources that GPs can refer patients to. These are listed in Box 6.
Managing the doctor’s anxiety
As with all illnesses, patients with anxiety disorders visit their GP when their symptoms are severe. The GP may interpret this high level of anxiety as an urgent need to do something. A GP’s anxiety can lead them to prescribe sedating medication (including sedating antidepressants, antipsychotics, benzodiazepines or antihistamines) or overinvestigate for all possible differential diagnoses. Our anxiety as doctors comes from our uncertainty about being able to relieve a patient’s distress, a mistaken sense that this needs to be done urgently and excessive concern not to miss a physical cause of anxiety. Unless the patient is expressing urgent suicidal ideation and intent, anxiety or even an acute panic attack does not cause serious harm. It is important for GPs to manage their anxiety about the patient’s anxiety. Patients frequently feel reassured when a diagnosis and treatment plan are provided.
Conclusion
Anxiety disorders are common in adults, but often missed and poorly treated in clinical practice. The RANZCP Clinical Practice Guidelines for anxiety disorders provide updated and relevant information for clinicians regarding the management of anxiety disorders. We have drawn from the guidelines to provide GPs with practical clinical tools to help manage patients with panic disorder, SAD and GAD. The full guidelines concern the acute, continuation and maintenance phases of treatment, and provide clear guidance to ensure the optimal management of patients with anxiety disorders. The advice provided in the clinical practice guidelines should equip GPs to navigate the complexities of managing these conditions. MT
Professor Philip Boyce has received speaker fees, consultancy fees and an educational grant from Servier Laboratories Australia Pty Ltd outside of the submitted work. He has also received speaker fees from Eli Lilly Australia Pty Ltd and Lundbeck Australia Pty Ltd outside of the submitted work.
Dr Christopher Gale is a member of the Cochrane Common Mental Disorders Group and contributor to Clinical Evidence 1999 to present.
Professor Ronald Rapee is the author of self-help books for child anxiety and adult SAD from which he receives royalties. He has also developed a manualised CBT program for child anxiety from which he receives no direct income.
Associate Professor Lisa Lampe has received payment for a presentation from Lundbeck Australia Pty Ltd outside of the submitted work.
Dr Greg Wilkins and Associate Professor Caroline Bell: None.
References
165: 45-52.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.